
Abstract
Objective
To examine the association between venous thromboembolism and prolonged work- and computer-related seated immobility.
Design
A case-control study.
Participants and setting
Cases were 200 patients attending venous thromboembolism clinics with a history of deep vein thrombosis and/or pulmonary embolism in the past six months, and controls were 200 patients treated in fracture clinic for an upper limb injury in the past six months.
Main outcome measures
Logistic regression was used to estimate the association between venous thromboembolism and prolonged work- and computer-related seated immobility in the 28 days before the index event. Prolonged work- and computer-related seated immobility was defined firstly as a categorical variable with at least 10 h seated in a 24-h period, including at least 2 h without getting up; and secondly as the actual time spent seated in a 24-h period.
Results
Prolonged work- and computer-related seated immobility (categorical variable) was present in 36 (18%) cases and 31 (15.5%) controls. In multivariate analysis, there was no significant association between prolonged seated immobility and venous thromboembolism, odds ratio 1.18 (95% CI 0.56 to 2.48), P = 0.67. For the mean and maximum number of hours seated in a 24-h period, the odds ratios for the association per additional hour seated with venous thromboembolism were 1.08 (95% CI 1.01 to 1.6), P = 0.02 and 1.04 (95% CI 0.99 to 1.09), P = 0.08, respectively.
Conclusion
This study found a weak association between venous thromboembolism and prolonged work- and computer-related seated immobility, with increasing mean hours seated associated with a higher risk of venous thromboembolism.
Introduction
In 1853, Virchow described the triad of contributory factors of endothelial injury, stasis of blood flow and hypercoagulability in the pathogenesis of venous thromboembolism comprising deep vein thrombosis and pulmonary embolism. 1 The association between protracted seated immobility and pulmonary embolism was first described by Simpson during World War II, when he investigated the increased incidence of fatal pulmonary embolism in people confined to air raid shelters during the London blitz. 2 This was attributed to venous compression resulting in endothelial injury and venous stasis due to sitting for protracted periods in deckchairs. The rate of pulmonary embolism was noted to decline substantially, when the deckchairs were replaced with stretchers where the occupants could lie flat.
In the last few decades, studies have shown a likely causal association between venous thromboembolism and prolonged seated immobility associated with long-distance air travel.3–6 Studies have shown that venous stasis occurs in subjects seated in airline seats, with reduced popliteal venous flow of 40% when their feet reach the floor, and up to twofold reduction in popliteal venous flow when their feet do not reach the floor 7 and that there is increasing risk of pulmonary embolism as flight distance and duration increases,3,4 and increasing risk for those travellers who move rarely or not at all during long-distance flights.4,5 Analyses of other modes of transport have shown a similar increased risk of venous thromboembolism with extended periods of bus, train and car travel.8–10 Investigators now postulate that the seated immobility of travel may be more of a causative factor than the mode of travel itself.9,10
More recently, prolonged seated inactivity related to either occupation or lifestyle has also been associated with increased risk of venous thromboembolism, with associations found with single or repeated episodes of prolonged computer use,11–13 women with sedentary lifestyles, 14 workers sitting in cramped positions, 15 and day-to-day prolonged work- and computer-related seated immobility.16,17
In case-control studies of venous thromboembolism risk factors, we have reported a 1.8 – to 2.8–fold increased risk of deep vein thrombosis and/or pulmonary embolism resulting in hospital attendance associated with prolonged seated immobility at work, 16 together with time spent seated at the computer at home, 17 and travelling to and from work. 16 Both studies included a control group selected from patients presenting to the coronary care unit, whose admissions were predominantly due to thrombosis in the arterial system, whilst the cases had thrombosis in the venous system. However, this approach may have underestimated the risk associated with prolonged seated immobility, as patients with cardiovascular disease may be more likely to have a sedentary occupation, due to limitations placed on them by their co-morbidity. For this reason, we undertook a further case-control study to estimate the strength of the association between venous thromboembolism and prolonged work- and computer-related seated immobility utilising a different ‘healthy’ control group, selected on the basis of a presentation to the Emergency Department with an upper limb injury. We hypothesised that prolonged sitting at work and using a computer at home would be associated with a greater risk of venous thromboembolism than that observed in our previous case-control studies.
Methods
Cases for the study were from consecutive patients attending the Capital and Coast District Health Board venous thromboembolism service outpatient clinics between October 2011 and January 2013. For inclusion as a case, the patients needed to be aged between 18 and 65 years and have a confirmed diagnosis of venous thromboembolism within the last six months. With the exception of oncology patients, the venous thromboembolism service sees most cases who have presented for diagnosis and management in both primary and secondary healthcare services. A diagnosis of venous thromboembolism required confirmation by compression Doppler ultrasound, lung ventilation/perfusion scan, or helical computerized tomography with pulmonary angiography. Patients with arterial thromboembolic disease or who had superficial thrombophlebitis without extension into the deep venous system were excluded.
Controls were recruited from orthopaedic outpatient departments at Capital and Coast District Health Board between February 2011 and April 2013. Patients were eligible if they were aged between 18 and 65 years of age, had suffered a traumatic upper limb injury within the previous six months and had no venous thromboembolism, or clinical suspicion of venous thromboembolism, within the same time frame. The choice of upper limb injuries as a control group was made as this patient group would come from within the same community as the venous thromboembolism cases, and, similar to the venous thromboembolism cases, would present to the same local emergency department with an acute event and be managed within an inpatient setting if indicated, with follow-up care provided in an outpatient setting.
Risk factors for venous thromboembolism.
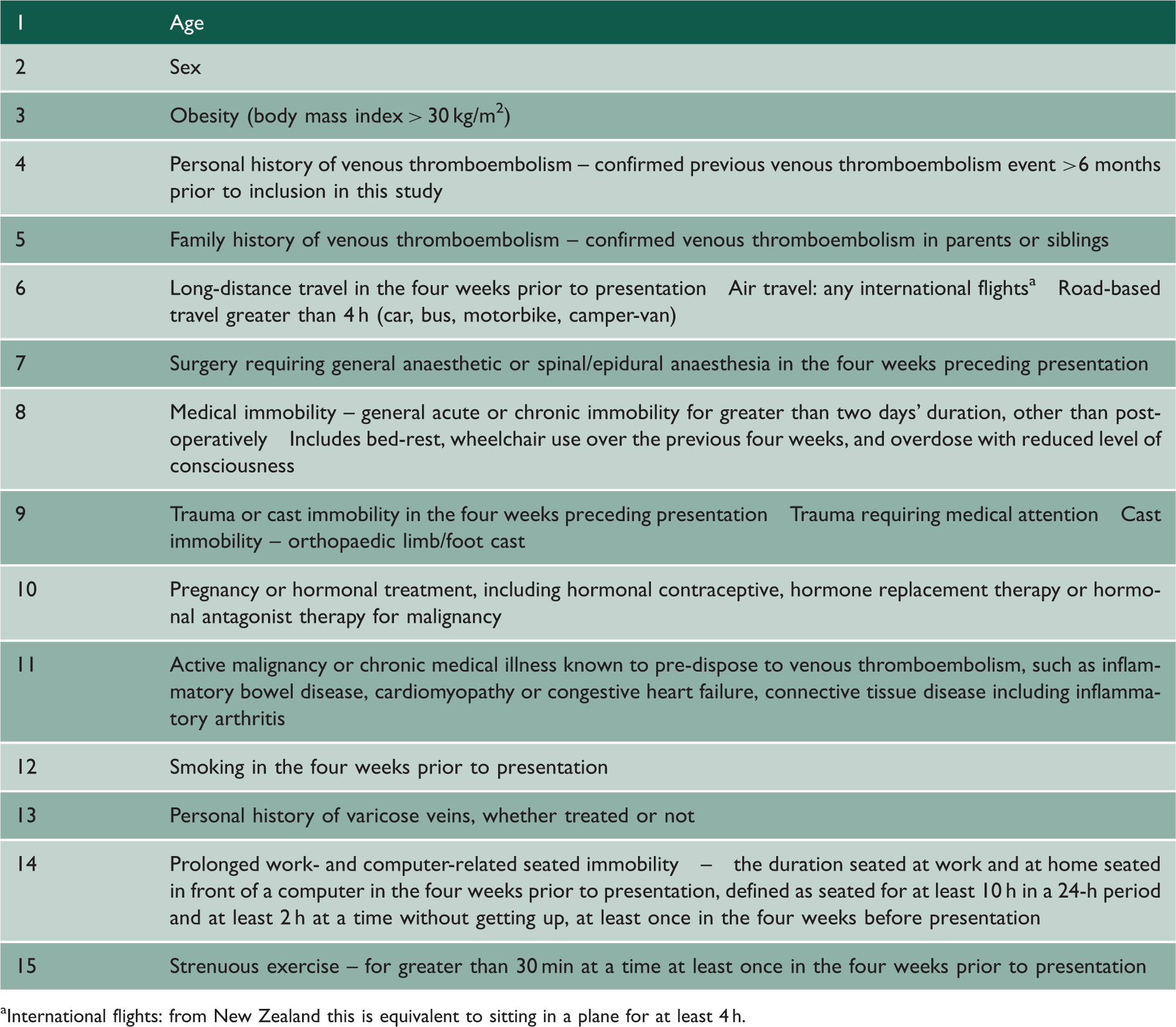
International flights: from New Zealand this is equivalent to sitting in a plane for at least 4 h.
Prolonged work- and computer-related seated immobility was defined in two ways. The first was as a categorical variable; being seated at work, and/or on the computer at home for at least 10 h within a 24-h period and, within that same period, for at least 2 h without getting up. Subjects had to do this at least once in the 28 days before the onset of symptoms in the index event. If participants drove for their occupation (e.g. truck or taxi driver, courier), this was included in the immobility calculation, but commuting to and from work was not included. The second definition of work- and computer-related seated immobility was as continuous variables including the mean and maximum number of hours seated in a 24-h period and the maximum number of hours seated at one time without getting up. This was also for the 28 days before the onset of symptoms in the index event.
Occupation was categorized according to Australia and New Zealand Standard Classification of Occupations then combined into high and low sedentary categories as previously described. 17 Medical records for the cases were reviewed for radiological confirmation of venous thromboembolism, and to assess whether seated immobility for travel or at work were listed as risk factors by the referring medical professional and/or the assessing doctor at presentation. Data collection also included whether the venous thromboembolism event was considered to be idiopathic, whether a thrombophilia screen had been requested, and any subsequent results.
Statistical methods
Univariate logistic regression was used to measure the strength of the association between case-control status and other explanatory variables. For the continuous variables, the difference in mean values was also assessed with a simple t-test. In a multivariate logistic regression, the predictor variables for case-control status were one or more episodes of prolonged work- and computer-related immobility in the 28 days prior to the index event, maximum hours using a computer in one day, average hours of computer use in one day, and maximum and average hours using a laptop in one day. These were adjusted for pre-specified confounding variables: body mass index >30 kg/m2, a personal history of venous thromboembolism, a family history of venous thromboembolism, and any of the following within the 28 days prior to the development of symptoms of the index event; immobility, surgery, cast immobilisation, air travel and/or road travel, and strenuous exercise in the 28 day period prior to the index event.
Power calculation
Based on previous studies,16,17 we anticipated that 10–15% of controls would meet the categorical definition for prolonged seated immobility. It was anticipated that a sample size of 400 (200 cases and 200 controls) would give 80% power to detect an odds ratio for risk of 2.0 if the control rate was 15%, and an odds ratio for risk of 2.25 if the control rate were 10%, with a type 1 error rate of 5%. These odds ratios were based on the previous studies in which similar categorical variables for prolonged seated immobility were associated with venous thromboembolism, with odds ratios of 1.8 (95% CI 0.71 to 4.8)16 and 2.8 (95% CI 1.2 to 6.1, P = 0.013). 17
SAS version 9.3 was used.
Results
Of 206 possible cases approached to take part in the study 4 declined, and 2 were excluded as they did not have radiologically confirmed deep vein thrombosis or pulmonary embolism, leaving 200 cases for analysis. The mean age (SD) of the cases was 46.1 (12.7) years, and 93 were female. There were 136 index deep vein thromboses; 121 in the lower limb (53 proximal, 67 distal and 1 unspecified), 14 in the upper limb and 1 abdominal. There were 71 cases of pulmonary embolism (seven of whom also had confirmed deep vein thrombosis); 14 were sub-massive (large thrombus burden with a troponin T rise or evidence of right ventricular strain), and 4 were massive (large thrombus burden with syncope and/or systolic blood pressure less than 90 mmHg).
Of 250 possible controls approached, 27 declined and 23 were unable to be matched with the cases, leaving 200 age and sex-matched controls. The mean (SD) age of the controls was 45.9 (13.1) years, and there were 93 females. There were 154 fractures, 15 sprains, 31 ‘other’ injuries (e.g. dislocation, laceration). Most injuries (58%) were distal.
Characteristics of study participants and univariate odds ratios between potential risk factors and venous thromboembolism.

n = 200 for cases and controls unless stated.
Univariate and multivariate associations between components of seated immobility and venous thromboembolism event.

All adjusted for body mass index greater than 30, personal history of venous thromboembolism, family history of venous thromboembolism, immobility, surgery, use of cast, recent air travel, recent road travel and exercise status.
Prolonged work- and computer-related seated immobility – defined as seated in front of a computer, at work or at home, for at least 10 h in a 24-h period and at least 2 h at a time without getting up, at least once in the four weeks before presentation.
Study participants by occupational group and sex, N = 200 for both cases and controls.

Discussion
This case-control study has found a weak association between prolonged work-and computer-related seated immobility and venous thromboembolism risk. Although the point estimates for all the categorical and continuous variables were consistent with an increased risk, only the measurement of seated immobility defined as the mean number of hours seated in a 24-h period was statistically significant, with the odds ratio for risk increasing by 1.08 for each 1 h longer seated in a 24-h period.
These findings complement the previous case-control studies undertaken by our group, which utilised similar criteria for prolonged work- and computer-related seated immobility, but a different control group.16,17 In the previous studies, we selected controls from patients presenting to coronary care unit, based on the landmark case-control study on traveller’s thrombosis 8 and recognition of common risk factors for venous thromboembolism and atherosclerosis.17,18 We hypothesised that this coronary care unit group might result in an underestimation of the risk associated with prolonged seated immobility as such patients may be more likely to have a sedentary occupation due to limitations placed on them by their cardiovascular disease. For this reason, we chose a different control group, a ‘healthy’ group presenting to the Emergency Department with upper limb injury in whom there was no clinical suspicion of venous thromboembolism. In addition to age, we also matched by sex in the current study, due to the possibility that women were more likely to be in sedentary employment. This did not turn out to be the case with a similar proportion of men and women reporting a sedentary occupation in the control group.
In this study, using fracture clinic patients as the control group resulted in a greater proportion of controls having prolonged seated immobility than in the previous study with the coronary care unit-derived controls (15.5 vs. 9.6% in fracture controls and coronary care unit controls, respectively). In contrast, the proportion of venous thromboembolism cases reporting prolonged seated immobility was similar (18.0 vs. 16.8%, respectively). The use of the fracture clinic control group may have unexpectedly been inappropriate, as this group may have an association with immobility and their risk of upper limb fracture, perhaps related to reduced bone density secondary to immobility, or a greater tendency to fall and injure themselves because of less physical fitness and balance. It is possible the selection of controls derived from coronary care unit may be preferable, on the basis that it may be more representative of the population at risk of presentation to hospital with a venous thrombosis.17,18
It seems likely that although convenient to treat seated immobility as a dichotomous variable, this may lose information relevant to a causal relationship between this behaviour and venous thromboembolism. We anticipated this might be the case and as previously, we also examined continuous variables relating to the total duration of being seated and the duration seated at a particular time, both of which contribute to the venous thromboembolism risk with prolonged seated immobility associated with long-distance air travel. 4 These included the association with the mean duration of seated immobility, in addition to the maximum duration on a single occasion, to obtain a measure of the burden of seated immobility over a 28-day period. Also, we examined the association with laptop use, in addition to computer use while seated. For these continuous variables, the point estimates all favoured an association between measures of prolonged seated immobility and venous thromboembolism risk, although only the mean number of hours seated in a 24-h period was statistically significant.
We also assessed the role of seated immobility at work by crude classification of individuals into high- and low-sedentary occupations. Sedentary occupations, including managers, professionals (including information technology) and clerical and administrative workers, had a point estimate of association of an odds ratio of association with venous thromboembolism of 1.3 compared to non-sedentary occupations. This is consistent with our previous finding of an odds ratio for association of with venous thromboembolism of 1.7 in the same sedentary occupational groups. In our previous work, however, the association was not significant after adjusting for other confounding variables including prolonged seated immobility at work and at a computer at home. This suggests that prolonged sitting rather than other aspects of the occupation is related to the association. This is also consistent with the findings of a Danish cohort study based on national registers that reported that drivers potentially exposed to prolonged cramped sitting at work were at a 1.28-fold greater risk of pulmonary embolism than a socioeconomically comparable group of construction workers with more dynamic physical work demands. 15 It is unclear why the incidence of venous thromboembolism is not increased in long-haul commercial airline pilots, who are also exposed to prolonged periods of sitting. 18
We assessed seated immobility only as it related to work and recreational computer use. We did not include immobility related to television watching, video-gaming, or tablet technology, nor did we include non-screen-based activities such as reading. Thus, we did not assess the potential role of these or other forms of seated immobility and venous thromboembolism risk and cannot be sure that other immobility-related behaviours were not more prevalent in one group than the other. A comprehensive retrospective study to assess all of these activities is likely to be difficult due to their variability and the uncertainty with recall.
Travel represented the other risk factor related to prolonged seated immobility that was assessed in our study. We observed a significantly increased risk of road travel >4 h in the univariate, but not the multivariate analyses, and a significantly increased risk of international air travel in the multivariate but not the univariate analyses. Together with the observation that long-distance road travel was about twofold more common than long-distance air travel, these findings illustrate the importance of considering all forms of long-distance travel, rather than just air travel in assessing venous thromboembolism risk. This interpretation is consistent with the findings of the landmark case-control study of travel and venous thromboembolism risk, in which travel >4 h in the four weeks preceding presentation was associated with a fourfold increased risk of venous thromboembolism, with about two-thirds of cases related to car travel. 8 Similarly, the large population-based case-control study from the Netherlands reported that the venous thromboembolism risk for flying was similar to the risks of travelling by car, bus or train, and long-distance car travel was the most common form of travel in this population. 9
These findings of increased risk of venous thromboembolism with seated immobility in a growing range of contexts, (occupational, recreational computer use, air travel, road travel), suggest that clinicians should consider seated immobility thrombosis in its widest context when assessing risk for venous thromboembolism. This is all the more important when individuals may present with more than one context in which they are seated for prolonged periods of time.
The clinical relevance of our findings is suggested by the recognition that if protracted seated immobility is not identified as a possible risk factor for venous thromboembolism, then in these settings venous thromboembolism may be classified as idiopathic. This could then lead to recommendations for indefinite, rather than time limited, anticoagulation with its concomitant risks, and failure to give lifestyle modification advice to reduce the risk of recurrence.
Conclusions
This study provides some evidence that prolonged work- and recreational-computer use is associated with venous thromboembolism, particularly as mean hours seated in a 24-h period increases. This type of immobility is unlikely to be recognised in clinical settings and could lead to misclassification of venous thromboembolism as idiopathic, leading to prolonged, inappropriate anticoagulation and a missed opportunity to address modifiable risk factors.
Footnotes
Declarations
Acknowledgements
We would like to thank Matthew McKenzie who collected data for this study as part of a summer studentship between November 2012 and January 2013. We would like to thank all participants for their time and participation in this study. Our thanks to Lifeblood, the Thrombosis Charity and the Health Research Council for their financial support of this study.
Provenance
Not commissioned; peer-reviewed by Joseph Yikona