
Abstract
The macroscopic appearances of florid cystitis cystica et glandularis can be mistaken for malignancy, and it is therefore important to perform a prompt resection to confirm the histological diagnosis and exclude sinister pathology.
Case report
A 16-year-old boy with no urological or medical history presented to his general practitioner with a six-month history of strangury, poor flow, suprapubic discomfort, urinary frequency and urgency. He had also noticed one recent episode of visible haematuria. There was no family history or congenital abnormality noted. Blood tests revealed a normal renal function. An ultrasound of his urinary tract had been ordered in the community, which had shown two large polypoidal masses arising from the right and left lateral walls of the bladder, measuring up to 2.1 cm and 2.5 cm, respectively. The remainder of the urinary tract was unremarkable, and there was no significant post-void residual volume (Figure 1).
Transabdominal ultrasound of bladder showing two large polypoid masses near bladder neck.
The patient was referred urgently to be seen by the urology team. Following further discussion in clinic with the patient and his parents, a decision was made to proceed directly to cystoscopy under general anaesthetic for further evaluation and possible resection of these lesions. A urine cytology was sent which showed a few inflammatory cells but no overtly malignant cells to be present. Serial urine cultures had revealed no growth and he had no history of previous urinary tract infections. On cystoscopic examination, following dilatation of a tight urethral meatus from 14Ch, the two large polypoid lesions were identified on either side of the bladder neck that they were partially obstructing, resembling malignancy in some areas and inflammatory masses in others (Figure 2). The remainder of the urethra was normal. Neither ureteric orifice was visualised. Both lesions were resected using a 17Ch resectoscope, and a small red area on the posterior wall was biopsied. A decision was made to remove the majority of the lesions from around the bladder neck, leaving as much normal or non-polypoid tissue as possible to reduce the risk of bladder neck stenosis. The patient was kept overnight for bladder irrigation, and the catheter was removed the following day with no postoperative complications.
Cystoscopic views of large polypoid lesions arising from either side of bladder neck.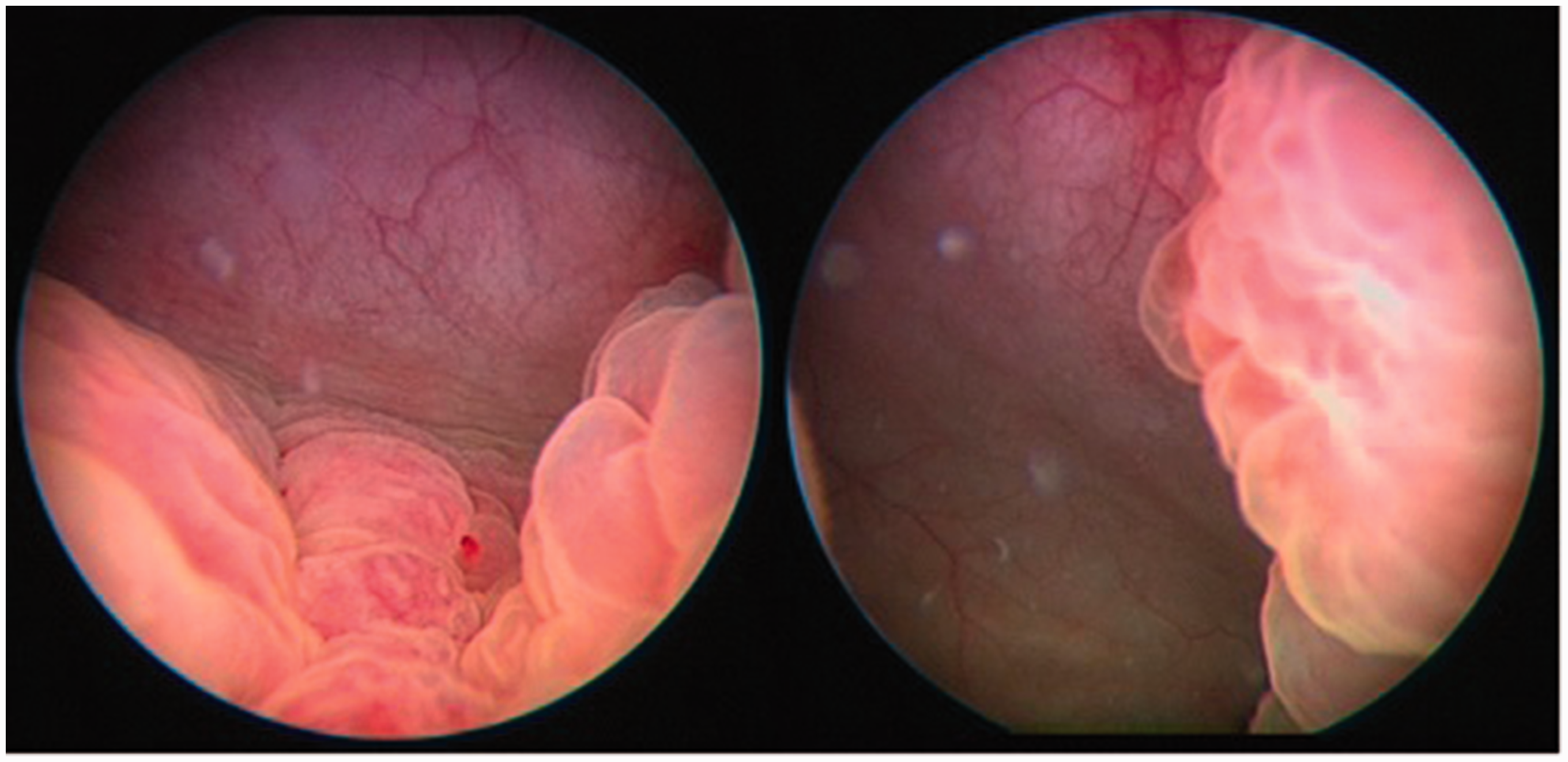
Histological examination of the resected tissue revealed florid cystitis cystica and cystitis glandularis in all three specimens. Muscle was included in two of the three specimens. No intestinal metaplasia was seen, and no evidence of dysplasia or malignancy was identified (Figure 3). The patient subsequently underwent an MRI scan of the pelvis which showed no other abnormalities in the pelvis (Figure 4). The LUTS symptoms had subsided one month post-operatively and flow rate returned to normal. Following discussion in our multidisciplinary meeting, a recommendation was made for repeat cystoscopy in six months time.
Micrograph of specimen showing nests of urothelial cells surrounding dilated lumen consistent with cystitis cystica. T1-weighted MRI images showing a coronal (bottom) and axial (top) section of the pelvis. Residual bilateral polypoid lesions can be seen inferoposteriorly within the bladder, but there are no other associated abnormalities.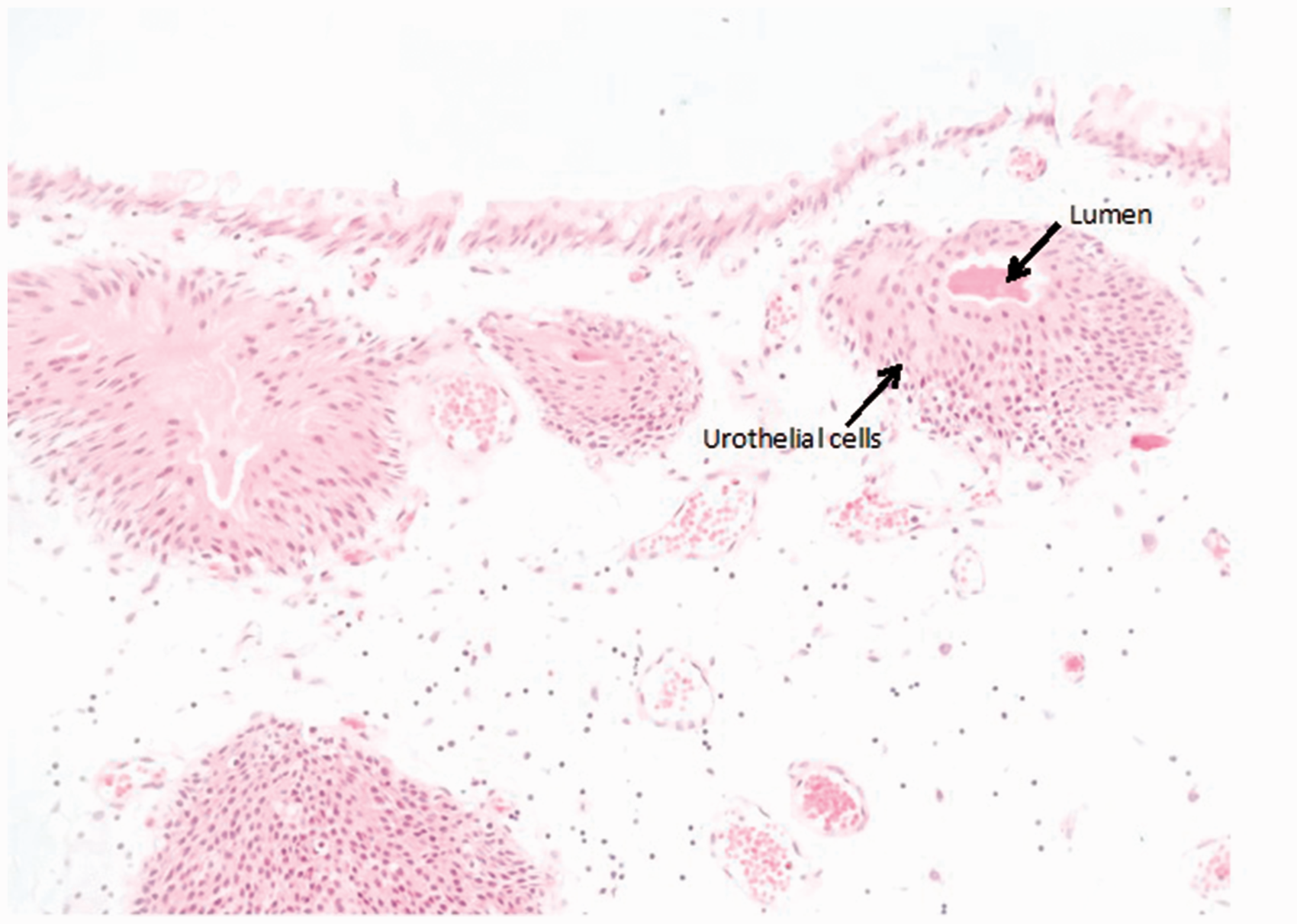

Discussion
Cystitis cystica is a hyperproliferative condition where initial submucosal masses of epithelial cells, termed ‘Brunns nests’, undergo cavitation to form fluid-filled cystic structures. 1 This is thought to represent a local immune response to a chronic inflammatory stimulus and has been associated with recurrent urinary tract infection. When present in children, it very rarely affects the male population. In one study by Milošević et al. looking at patients with confirmed cystitis cystica and no concurrent urinary tract abnormality over a 20-year period, of the 127 patients identified, only two were male. 1
Cystitis glandularis occurs when there is metaplasia in a mucous secreting epithelium and is characterised by a central lining of cuboidal or columnar cells. 2 It is a rare entity in children, and there have been only a handful of reported cases in the literature. In one study looking at all paediatric specimens taken from the urinary bladder over a 21-year period at the Children’s Hospital of Philadelphia, only three patients were identified with cystitis glandularis. A clinical history for only one of these patients was available in this retrospective study, and it remarked on a prior bladder exstrophy repair. 3 A small number of individual cases have been reported in children over the years.4–6 An association has been documented with bladder exstrophy, pelvic lipomatosis and recurrent urinary tract infections. 6 Both cystitis cystica and cystitis glandularis can present with irritative lower urinary tract symptoms and haematuria. As there was an absence of UTIs and no anatomical abnormality, the only factor that could have contributed to this patient’s florid pathology was the meatal stenosis and the effect of the resulting chronic outflow obstruction on his bladder. This has never been described in isolation previously.
The significance of cystitis glandularis with regard to premalignant risk is the subject of much debate. Currently, although cystitis glandularis can be found to exist in conjunction with bladder carcinoma, there is not sufficient evidence at present to confirm that the presence of cystitis glandularis increases future malignant potential. 7 However, the premalignant risk with very widely proliferative cystitis glandularis lesions cannot completely be excluded. 6 At present, the treatment of patients with cystitis cystica involves long-term antibiotic prophylaxis for urinary tract infections. 1 For cystitis glandularis, transurethral resection of the lesions is generally the only treatment required. 6
In conclusion, we report a rare case of cystitis glandularis in a child with no prior urological history, along with florid cystitis cystica, an uncommon finding in male children. The macroscopic appearances on cystoscopy can be mistaken for malignant tumours. Prompt resection of the lesions and subsequent histological analysis successfully excluded the presence of malignancy, as well as providing relief of the patient’s symptoms. It is important to thoroughly evaluate children who present with haematuria in order to exclude sinister pathology, and in this case, we were able to achieve a good clinical outcome. There may be a role for surveillance cystoscopy or imaging in children with cystitis glandularis as recurrence risk and premalignant potential cannot be completely excluded.
Footnotes
Declarations
Acknowledgements
None.
Provenance
Not commissioned; peer-reviewed by Marios Hadjipavlou.