
Abstract
In case of high output cardiac failure, an arteriovenous fistula should be considered.
High-output heart failure due to ilio-iliac arteriovenous fistula is a rare phenomenon. We describe a case where patient initially presented with features of heart failure. He had a history of dilated cardiomyopathy and cardiac ablation procedure done for atrial flutter. Subsequent decompensation and multiorgan failure led to extensive diagnostic work-up revealing a normal heart and an arteriovenous fistula that was managed successfully with endovascular repair.
Case presentation
A 58-year-old driving instructor presented with a four-week history of worsening breathlessness, abdominal distension and leg swelling. He had presented with similar features about six years ago. He was then diagnosed with alcohol-related dilated cardiomyopathy with impaired left ventricular systolic function (ejection fraction 25%) as he was then drinking over 120 units of alcohol a week and had a normal coronary angiogram. He had an atrial ablation procedure for atrial flutter four years ago and following a period of abstinence his heart failure symptoms had resolved. He also had a history of hypertension and recently diagnosed with type 2 diabetes. He had started drinking moderate amounts of alcohol again. On examination, he had a heart rate of 92 and blood pressure of 128/54. He had 94% oxygen saturation on pulse oximetry on air with a normal respiratory rate. He had an elevated jugular venous pressure up to his right ear lobe. Auscultation of heart and lungs revealed a loud pan-systolic murmur and bi-basal crepitations. His abdomen was markedly distended with 5 cm non-tender hepatomegaly and shifting dullness. He had significant peripheral oedema up to his umbilicus. Chest X-ray showed pulmonary congestion. Electrocardiography on admission showed sinus rhythm with no ischaemic changes and no evidence of left ventricular hypertrophy. Blood tests on admission were normal other than a slightly elevated international normalised ratio (1.5).
The patient was initially diagnosed and managed as decompensated heart failure. The patient’s oedema and ascites did not improve with diuretics and his weight increased from 128 kg to 142 kg. His renal and liver functions deteriorated and he became increasingly jaundiced (bilirubin 83, aspartate aminotransferase 188, alkaline phosphatase 179, international normalised ratio 2.6). An up-to-date echocardiogram showed only mild left ventricular dilation with normal left ventricle and right ventricle function (left ventricular ejection fraction 60%). A liver ultrasound scan confirmed hepatomegaly and showed a dilated portal vein and evidence of periportal fibrosis. With a working diagnosis of liver cirrhosis, a computed tomography scan was arranged that did not show any radiological evidence of cirrhosis. After discussion at the hepatology multidisciplinary meeting, it was decided to perform a transjugular biopsy of the liver to rule out cirrhosis and paracentesis to relieve his worsening ascites.
Transjugular biopsy showed greatly elevated systemic venous pressures (inferior vena cava pressure: 40 mmHg, normal 5–10 mmHg) and elevated portal pressures (wedged portal pressure: 45 mmHg, normal range 1–5 mmHg) but a normal hepatic venous pressure gradient (normal range < 5 mmHg); findings consistent with systemic venous hypertension rather than portal hypertension. An ultrasound scan guided paracentesis drained 8 L of ascitic fluid.
After excluding cirrhosis, other causes of hepato-renal dysfunction were considered as the patient was progressively getting worse. He eventually started complaining of pain and paraesthesia in his lower limbs. Acute limb ischaemia was suspected and urgent duplex ultrasound scan arranged. Duplex scan showed poor distal flow in both lower limbs. A large right sided common iliac aneurysm was noted with turbulent arterial flow and highly phasic flow in the common femoral vein suggestive of an arteriovenous fistula. These findings were confirmed with computed tomographic angiogram (Figures 1 and 2).
Coronal view of right common iliac artery aneurysm and fistula between it and right common iliac vein. Note the significantly dilated inferior vena cava and hepatic veins. Angiogram with contrast being injected through left groin: Right Common Iliac artery aneurysm and fistula. Note markedly dilated inferior vena cava.

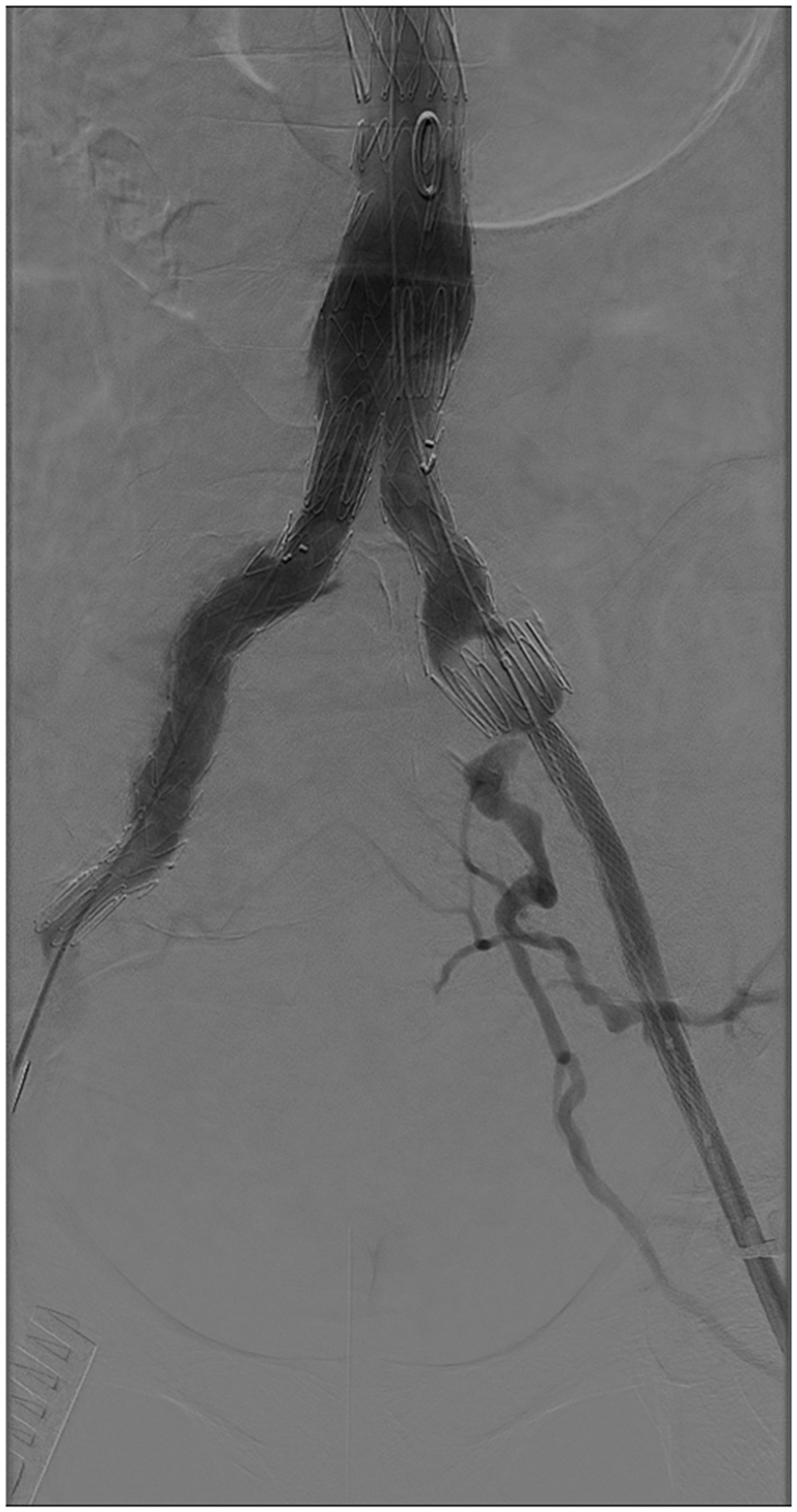
The patient was urgently transferred to the regional vascular surgery unit where he underwent endovascular repair. A satisfactory exclusion of the fistula was achieved with placement of a stent graft from just below the renal artery to both iliac bifurcations (Figures 3 and 4). There was an immediate improvement with reduction in his central venous pressure and improvement in urine output after the repair. Four days after the procedure (first two days in high dependency unit), patient was feeling much better and renal and liver function was markedly improved. He was discharged home nine days after the operation. He was reviewed in outpatients after two weeks and was significantly better clinically with no requirements for any antihypertensive or diabetic medicines. His liver biopsy showed changes consistent with hepatic congestion (cardiac cirrhosis) but confirmed there was no evidence of alcohol-induced liver injury.
Post-endovascular repair. Stent grafts inserted from just below renal arteries to bifurcation of right common iliac artery to exclude the fistula. Empty aneurysmal sac can also be seen. A completion angiogram showing exclusion of fistula by the stent graft.
Discussion
An ilio-iliac arteriovenous fistula presenting with decompensated heart failure, ascites and deranged liver and kidney function is rare.1,2 This case was more unusual as the patient had a previous history of heart failure attributed to alcohol-related dilated cardiomyopathy that recovered completely after a period of alcohol abstinence. Causes and presenting features of an arteriovenous fistula are quite varying and depend on their location, size, duration, calibre of vessels and the cardiopulmonary reserve of the patient. 3
An ilio-iliac arteriovenous fistula is a rare type of extra splanchnic abdominal arteriovenous fistula. Causes include aneurysmal rupture (spontaneous), trauma, surgery (iatrogenic), malignancy and infection. Cardiac catheterisation procedures are a known cause of groin arteriovenous fistula and the incidence reported is less than 1%. 4 Patients are classically reported to have high output heart failure, abdominal and/or lower back pain, palpable abdominal lump with a bruit and signs of local venous hypertension, i.e. lower extremity oedema, haematuria. 5 These features, however, were found in only 20–50% of patients in one reported study. 3 High-output heart failure is characterised by cardiac index of more than 4 L/min per m2. It is more common, present in 35% to 58% of cases, in aorto-iliac arteriovenous fistula due to the large calibre of vessels. 6 An arteriovenous fistula causes haemodynamic instability by increasing cardiac output as a result of shunting blood from high resistance arterial flow to low resistance venous circulation. It increases blood volume and heart rate and contractility by affecting the sympathetic and renin-angiotensin-aldosterone system (RAAS). One study describes an increase of 10% in cardiac output within two weeks of making an arteriovenous fistula fistula. 7
Arteriovenous fistulae, as in this case, can lead to multiorgan failure associated with increased morbidity and mortality. Surgical mortality in symptomatic arteriovenous fistula can be as high as 22–51%. 8 Mortality is potentially higher in patients without a preoperative diagnosis of such fistula. 3
The diagnosis remains unestablished in almost half the cases of Iliac and aortic arteriovenous fistulae.8,9 This is probably due to unusual presentations of these patients going through a few working diagnoses before the final diagnosis of arteriovenous fistula and acquiring a presumed clinical urgency by then. Abdominal bruit was the most consistent feature in such patients and yet was frequently overlooked. 3 Contrast-enhanced computed tomography or an angiography is the most commonly utilised diagnostic modality. Principles of fistula repair can be achieved by both open and endovascular techniques. Endovascular repair has shown promising results with benefits of being less invasive and causing less risk of major blood loss as shown in our case. 10
Footnotes
Declarations
Acknowledgements
None.
Provenance
Not commissioned; peer-reviewed by Nicola Mumoli.