
Abstract
Objectives
To determine the diagnostic accuracy of the cardiothoracic ratio on postero-anterior or antero-posterior chest radiographs in predicting left ventricular or right ventricular dysfunction on echocardiography in an inpatient population.
Design
Retrospective study.
Setting
Two secondary care hospitals in the United Kingdom.
Participants
Four hundred consecutive inpatient echocardiograms were screened for inclusion along with chest radiographs (both postero-anterior and antero-posterior). The cardiothoracic ratio was calculated from chest radiographs along with quantitative and qualitative measures of left ventricular or right ventricular dysfunction on echocardiography.
Main outcome measures
Sensitivity and specificity of cardiothoracic ratio across a range of values to detect moderate/severe left ventricular and/or right ventricular dysfunction on echocardiography.
Results
Overall, 272 records met inclusion criteria. The prevalence of left ventricular/right ventricular dysfunction on echocardiography was 26% in an inpatient population with high clinical suspicion of cardiac disease referred for echocardiography. Over a range of cardiothoracic ratio values on postero-anterior films, a value of >0.55 yielded the best sensitivity (62.5%) and specificity (76.5%) for diagnosing left ventricular/right ventricular impairment (positive likelihood ratio 2.56), with a positive predictive value of 29.5%. Cardiothoracic ratio on antero-posterior film was not predictive of left ventricular/right ventricular impairment on echocardiography.
Conclusions
In conclusion, in the context of an acute admission, cardiothoracic ratio measured on postero-anterior or antero-posterior films has limited value in detecting moderate left ventricular and/or right ventricular systolic dysfunction. Previously established absolute values may be unreliable by modern standards.
Introduction
In an inpatient setting, echocardiography is the most widely available standard for assessment of cardiac structure and function. Demand on services has increased, with a 2008 UK survey suggesting that the median inpatient wait for an echocardiogram was two days and that 21% of hospitals had an inpatient waiting time of more than five days. 1 A recent study from the USA suggested that the majority of echocardiograms performed had little clinical impact on patient management. 2 Prior to echocardiography, patients being admitted to hospital are likely to have a chest radiograph, often regardless of cardiorespiratory findings.3,4 Such radiographs have been shown to add little to the subsequent diagnosis or management of patients.3,4
First described in 1919, the cardiothoracic ratio is the classic and most widely known chest radiograph index of cardiac function. 5 Studies over many years have shown that an enlarged cardiothoracic ratio (defined in 1919 as >0.5 on a postero-anterior radiograph) is prognostically significant in healthy men, 6 the elderly 7 and in a variety of patients with congenital 8 and acquired heart diseases.9–14 As new modes of cardiac imaging have become available, studies have tried to improve on the ‘classic’ cardiothoracic ratio using other measurements of cardiac size derived from chest radiography13,15 and computed tomography; 16 or correlate it with measurements of left ventricular function based on angiographic,9,17 radionuclide15,17,18 and a variety of echocardiographic parameters.15,17,18 A cardiothoracic ratio of >0.5 on a postero-anterior radiograph in a primary care setting was a good predictor of subsequent left ventricular systolic dysfunction on echocardiography diagnosed in a heart failure clinic. 19 However, these studies have been in non-acute settings and in selected patient subsets with known left ventricular dysfunction.
Data are lacking on the validity of the cardiothoracic ratio to predict left ventricular dysfunction in ‘real-world’ acute inpatient settings. A significant proportion of admission chest radiographs are antero-posterior, usually due to acute immobility in an ageing population. Also, thoracic diameter is lower in the elderly20,21 which is likely to affect the cardiothoracic ratio. Our clinical experience was that a significant number of echocardiograms were requested on inpatients based on a physician interpreting admission antero-posterior chest radiographs as having an enlarged cardiothoracic ratio or cardiac dimension (often by eye), prior to a radiologist formally reporting the film.
The aim of our study was to investigate in an acute medical setting the relationship between cardiothoracic ratio on admission chest radiographs (both postero-anterior and antero-posterior) with left and right ventricular function (as the cardiac silhouette includes both the left ventricle and the right ventricle) determined from echocardiography during the same admission.
Methods
The retrospective study was undertaken across two sites – Bedford Hospital, Bedford, UK, and Northwick Park Hospital, Harrow, UK, in June and July of 2013.
Patient selection
Consecutive patients who had inpatient echocardiography were selected. In total, 400 echocardiogram reports were screened and included if the study was reported as being technically adequate, and qualitative and quantitative left ventricular and right ventricular data were present. Of these patients, those who had an admission chest radiograph (postero-anterior or antero-posterior) where the cardiothoracic ratio was calculable were identified and included as the final subset for analysis.
Echocardiography data
Echocardiography was performed by seven accredited cardiac physiologists within the two centres. Phillips IE33, CX50 and HD15 echo machines with S5-1 probes were used for image acquisition. All patients were studied according to the recommendations of the American Society of Echocardiography. 22 Measurements of systolic and diastolic left ventricular internal dimensions were collected. Qualitative assessment of left ventricular systolic function was recorded (based on American Society of Echocardiography criteria), as was ejection fraction calculated using Simpson’s biplane method where available. Fractional shortening was calculated as left ventricular internal dimension in diastole minus left ventricular internal dimension in systole divided by left ventricular internal dimension in diastole expressed as a percentage. Visual assessments of right ventricular function and size were also collected. Moderate or severe left ventricular/right ventricular dysfunction was defined as having any one of the following criteria: visual assessment of moderate or severe left ventricular systolic dysfunction, Simpson’s biplane calculated ejection fraction <45%, tricuspid annular plane systolic excursion <1.6 cm, visual assessment of moderate or severe right ventricular systolic dysfunction. The cardiothoracic ratio is used by most clinicians as a surrogate for moderate or severe left ventricular/right ventricular dysfunction, and so we used this pragmatically as our endpoint.
Measurement of cardiothoracic ratio
Chest radiographs were evaluated as being technically adequate if no gross rotational or thoracic abnormalities were noted. All postero-anterior and antero-posterior films, regardless of depth of inspiration, were included. Patients with severe consolidation or pleural effusions where the cardiac silhouette was indistinct were excluded. To obtain accurate measurement, a vertical line was drawn on the radiograph through the midpoint of the spine from the sternum to the diaphragm. The maximum transverse diameter of the heart was obtained by adding the widest distance of the right heart border from the midline and the left heart border to the midline (cardiac diameter). This value was then divided by the maximum transverse diameter of the thorax (the thoracic diameter) to give the cardiothoracic ratio, as shown in eFigure 1 in the Supplement. 5 Chest radiograph data were collected using digital imaging software separately, in a blinded manner to echocardiographic data, by two observers at Bedford hospital, and one observer at Northwick Park hospital, all of whom are experienced clinicians. Inter-observer variability was assessed using the same sample of 20 (10 postero-anterior and 10 antero-posterior) radiographs on which observers calculated cardiothoracic ratios. These were selected from the existing data by a computer-generated random number sequence.
Statistical analysis
Continuous data are presented as mean (standard deviation) and categorical data as counts or percentages. Analysis and comparisons of continuous data were performed using analysis of variance, whilst the χ2 test was used to compare categorical data. Fisher’s exact test was used if χ2 assumptions were not met. Correlations were investigated using the Pearson’s product moment correlation coefficient. The presence or absence of either left ventricular or right ventricular dysfunction (moderate or severe) was modelled as a binary categorical variable. Standard measures of test validity including sensitivity, specificity, likelihood ratios and predictive values with 95% confidence intervals were calculated. Disease prevalence was assumed to be the same as in the sample. Receiver-operator characteristic curves were used to investigate cut-off points and values selected that maximised the Youden index. 23 A two-sided probability level of <0.05 was considered significant. Inter-observer variability was assessed using Lin’s concordance correlation coefficient. 24 Calculations were performed using SPSS version 20.0 (IBM Software, USA).
Results
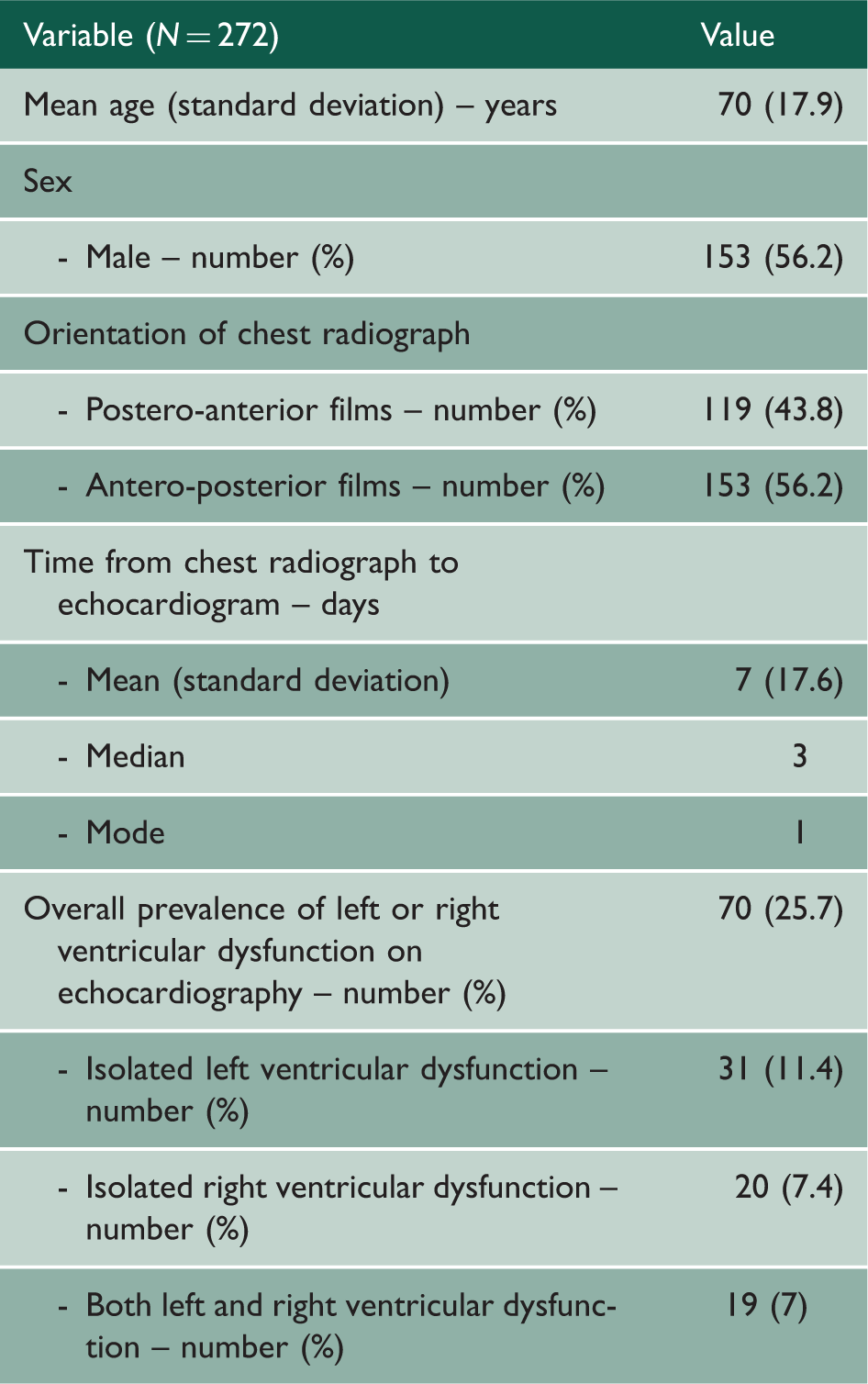
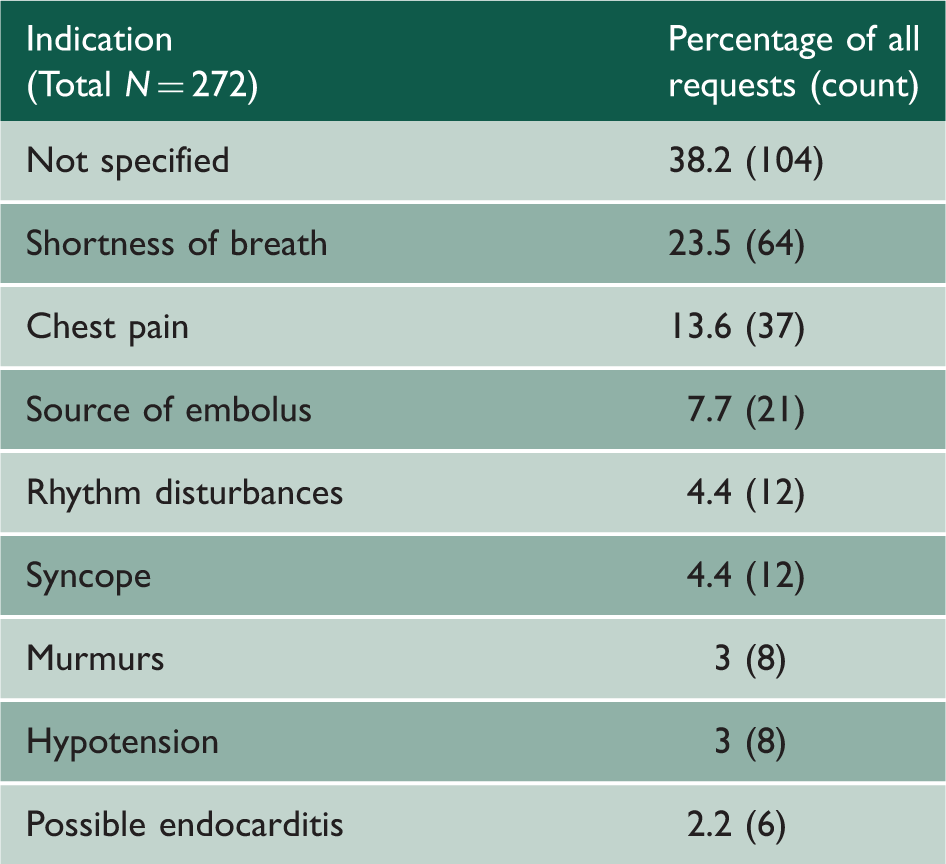
Three hundred and forty-four echocardiograms performed between March and May 2013 were deemed to have adequate windows and measurements to include in the study. Of these, 51 had no chest radiograph during the same admission and were excluded. A further 21 patients had chest radiographs where a cardiothoracic ratio was unable to be calculated (8 with consolidation masking heart borders, 5 with significant pleural effusions masking heart borders and 8 were technically too poor to evaluate). Two hundred and seventy-two patients had suitable inpatient echocardiograms and chest radiographs and these formed the final set for analysis (Figure 1). Baseline demographics are shown in Table 1. Prevalence of moderate/severe left ventricular or right ventricular systolic dysfunction was 20% in the postero-anterior film group (24 out of 119 patients) and 30% in the antero-posterior film group (46 out of 153 patients). Lin’s concordance correlation coefficient for inter-observer variability for cardiothoracic ratio measurements was 0.982 (95% confidence interval: 0.958 to 0.991). Indications for inpatient echocardiography were clear in 62% of requests and are listed in Table 2.
Flow chart showing selection of final subset of data that underwent testing. LV: left ventricle; RV: right ventricle. Baseline characteristics. Indications for inpatient echocardiography.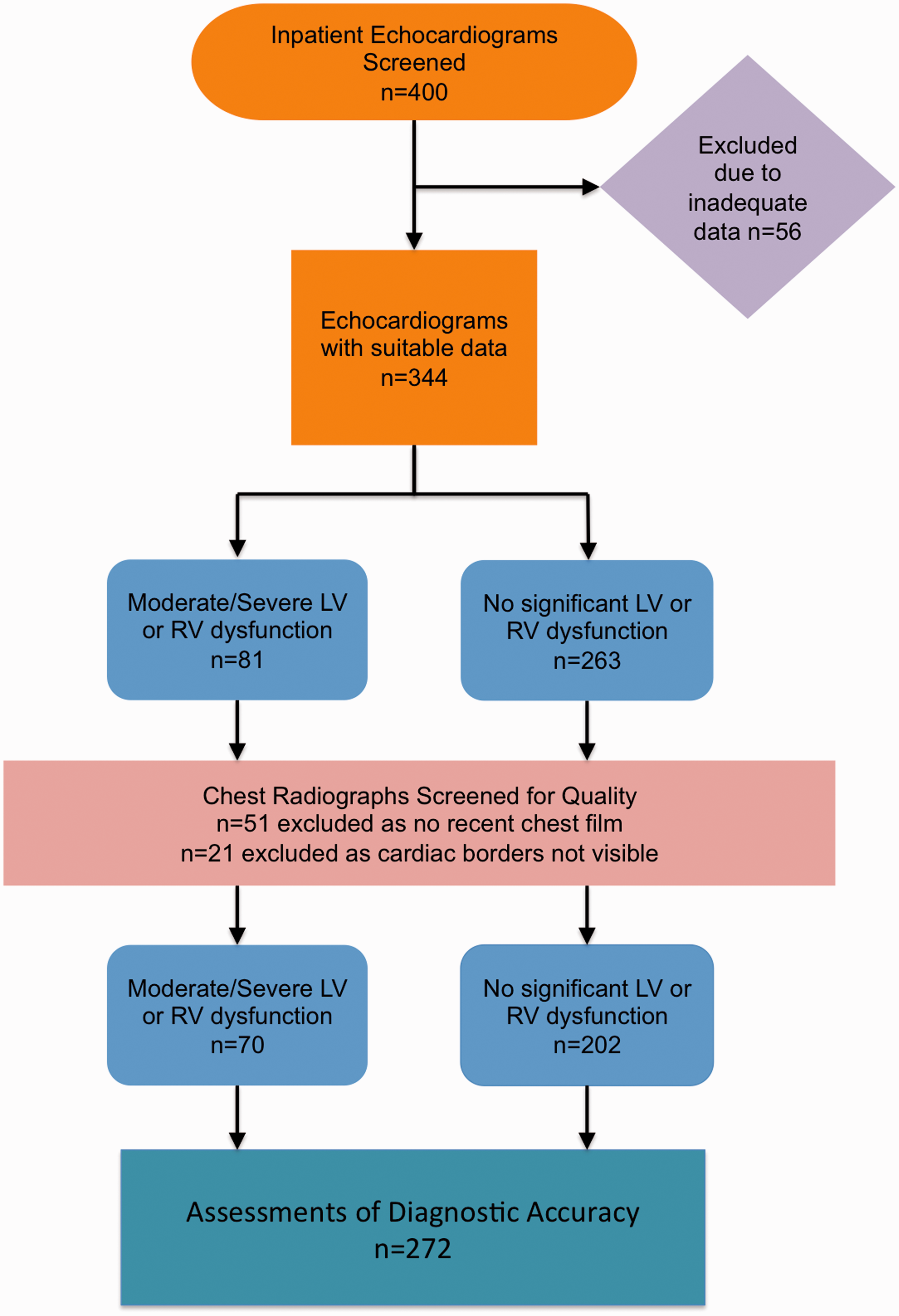
Cardiothoracic ratio
There was a significant difference in the mean cardiothoracic ratio between postero-anterior and antero-posterior films (0.52 vs. 0.56, 95% confidence interval for difference: −0.06 to −0.02, p < 0.001). Cardiothoracic ratio correlated strongly positively with age in the postero-anterior film group (r = 0.41, p < 0.001), and more weakly in the antero-posterior film group (r = 0.19, p = 0.022). In those cases where ejection fraction was calculable, cardiothoracic ratio correlated strongly negatively with left ventricular ejection fraction in the postero-anterior film group (r = –0.43, p = 0.008), but there was no correlation in the antero-posterior film group (r = 0.04, p = 0.79). There was no correlation between cardiothoracic ratio and fractional shortening in either group. Additionally, there was no correlation between left ventricular internal dimension in diastole (as a measure of chamber dilation) and cardiothoracic ratio in either postero-anterior or antero-posterior film groups.
In the postero-anterior film group, there was a significant difference in mean cardiothoracic ratio between those who had moderate/severe left ventricular or right ventricular dysfunction on echocardiogram and those who did not (0.56 vs. 0.51, 95% confidence interval for difference: 0.01 to 0.09, p = 0.012). In the antero-posterior film group, the difference in cardiothoracic ratio between those with moderate/severe left ventricular or right ventricular dysfunction on echocardiogram and those without was not significant (0.58 vs. 0.54, 95% confidence interval for difference: 0 to 0.05, p = 0.058).
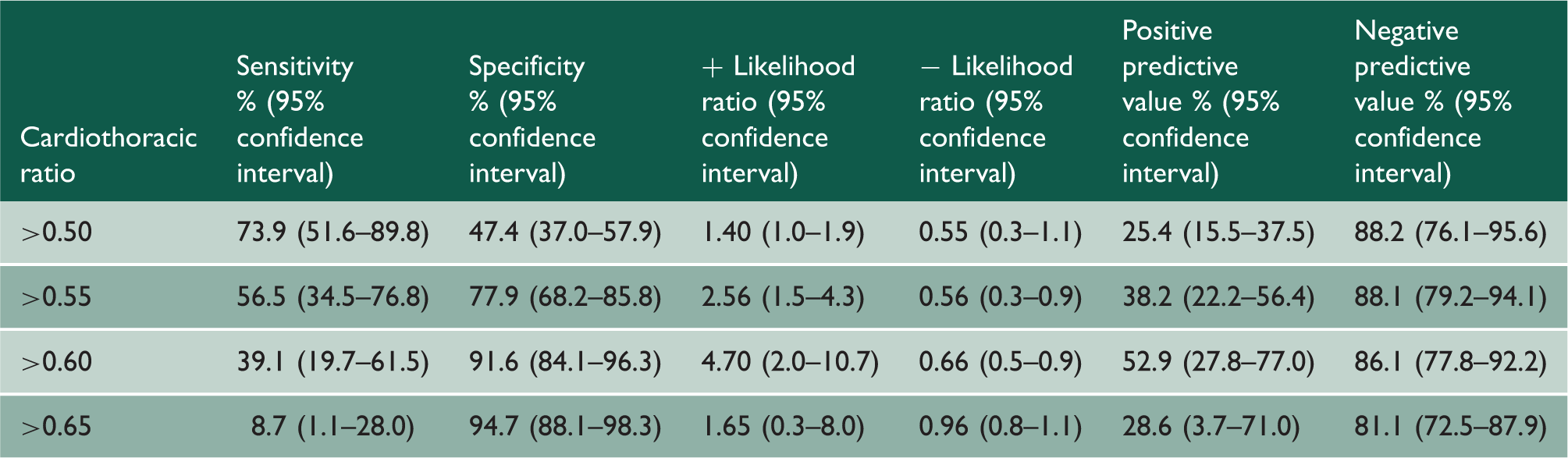
Receiver-operator characteristic curve modelling prediction of moderate/severe left ventricular or right ventricular dysfunction by cardiothoracic ratio in postero-anterior and antero-posterior film groups is shown in Figure 2. The area under the curve for cardiothoracic ratio on postero-anterior film was better than expected by chance (0.70, 95% confidence interval: 0.60 to 0.78, p = 0.002). Sensitivities, specificities, likelihood ratios and predictive values for a variety of cardiothoracic ratios for postero-anterior films are shown in Table 3. The value maximising the Youden index of sensitivity and specificity was a cardiothoracic ratio >0.55 (Youden J, 0.32), and a cardiothoracic ratio >0.6 maximised the positive predictive value and negative predictive value.
Curve of receiver-operator characteristics at different points of cardiothoracic ratio on postero-anterior and antero-posterior chest radiographs. ROC: receiver-operator characteristic; PA: postero-anterior; AP: antero-posterior. Diagnostic accuracy of cardiothoracic ratio in postero-anterior chest radiographs to predict left or right ventricular dysfunction on echocardiography.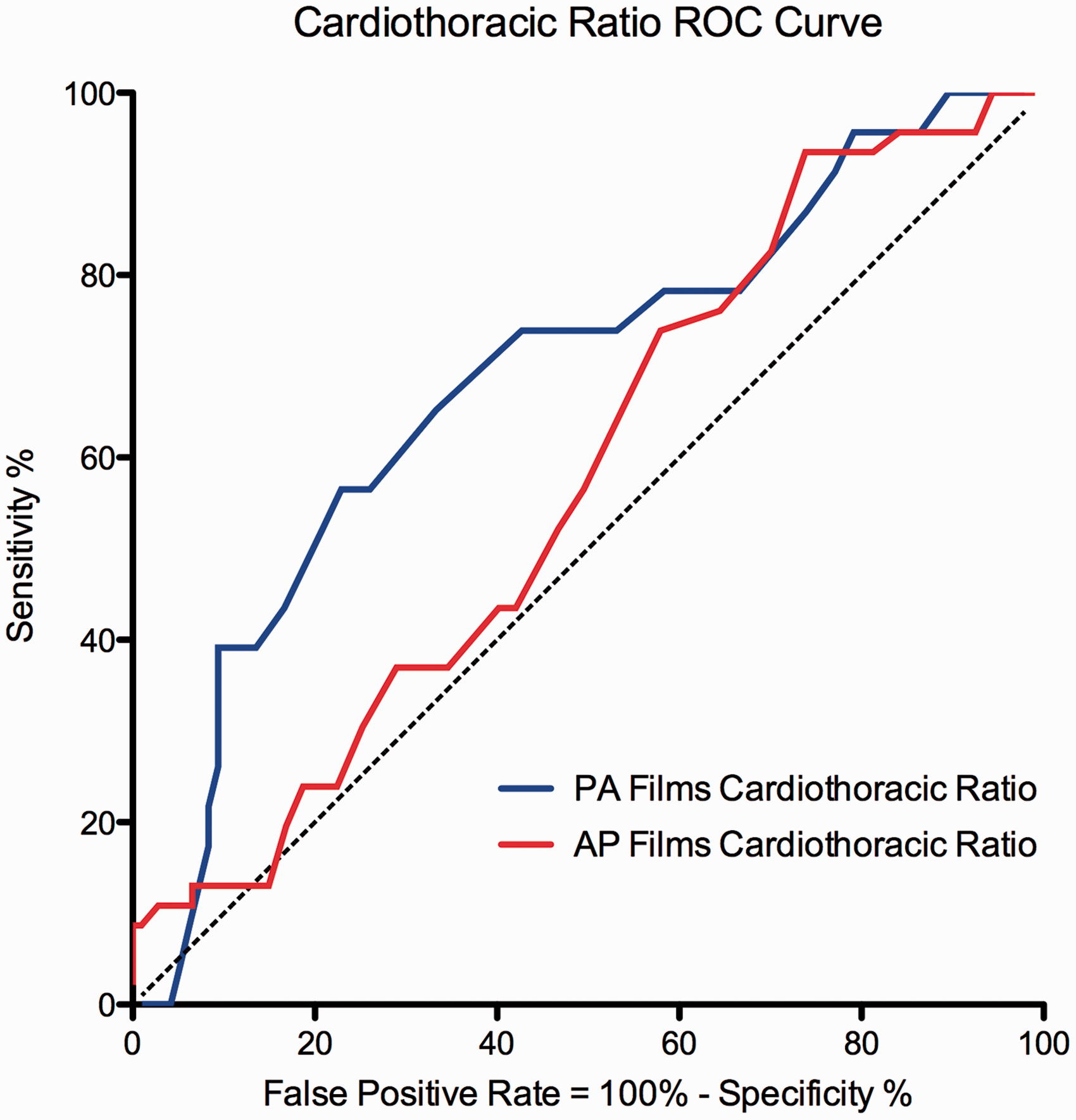
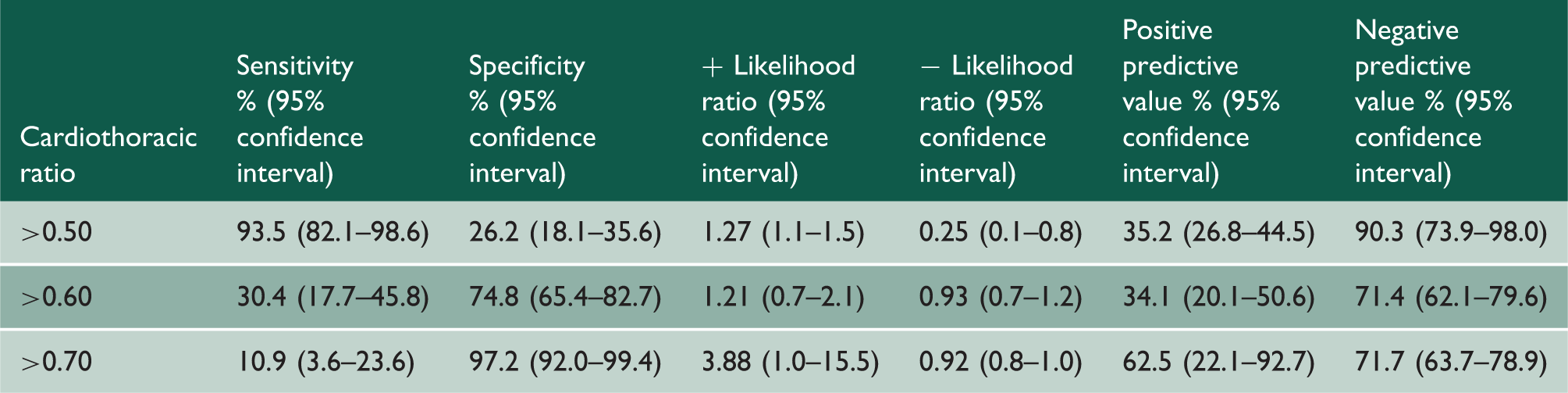
Diagnostic accuracy of cardiothoracic ratio in antero-posterior chest radiographs to predict left or right ventricular dysfunction on echocardiography.
Discussion
In a cohort of acute admissions, our study suggests that the traditional cardiothoracic ratio on a postero-anterior chest radiograph has moderate sensitivity and specificity but is ultimately not a good predictor of left ventricular or right ventricular dysfunction on echocardiography. The cardiothoracic ratio on an antero-posterior film does not appear to correlate well with echocardiographic measures of left ventricular or right ventricular dysfunction.
The fundamental assumption of the cardiothoracic ratio is that cardiomegaly indicates left ventricular or right ventricular dysfunction. While this was likely to be the case at the time when the cardiothoracic ratio was validated, the advent of echocardiography and the earlier diagnosis and treatment of heart failure mean the dilated and enlarged heart is no longer the only one with dysfunction. Traditional values for the cardiothoracic ratio and cardiac dimensions were validated by comparing groups of patients with heart failure and controls in an era where there was limited access to echocardiography.5,25 Subsequent studies have shown that progressive changes in the cardiothoracic ratio in groups of patients with known left ventricular impairment have prognostic implications.6–14 However, no study has previously examined the reliability of the cardiothoracic ratio in an inpatient setting as a predictor of left ventricular or right ventricular dysfunction on echocardiography, which is one way that it is commonly employed in clinical practice.
Postero-anterior films taken at a standard distance (180 cm) are the gold standard on which to base cardiothoracic ratio measurements. 5 However, an increasing number of elderly and immobile patients have antero-posterior films taken routinely. Studies have investigated cardiac size measurements on antero-posterior films previously.25,26 The studies all compared groups of patients with known left ventricular dysfunction to controls and made suggestions about calculating the cardiothoracic ratio from an antero-posterior film. Kabala and Wilde 25 reported a sensitivity of 92% and a specificity of 96% using a cardiothoracic ratio of 0.55 on antero-posterior films to diagnose congestive heart failure. Of note, none of the patients with congestive heart failure had echocardiograms, and the inclusion criteria for that group were a history suggestive of congestive cardiac failure as well as radiological signs of cardiac failure. This significantly calls into question their findings, as their inclusion criteria of radiological signs of cardiac failure overlap with the test variable of interest; namely the cardiothoracic ratio. More recently, Chon et al. 26 attempted to compare erect antero-posterior films with supine computed tomography chest measurements and tried to ‘correct’ for the differences in projection based on variable film to detector distances. They validated their method by comparing 18 patients with echocardiographic evidence of heart failure with 17 patients with normal echocardiograms and found a sensitivity of 61% and a specificity of 54% based on a ‘corrected cardiothoracic ratio’ of ≥0.5. Their sample was small and our results were unable to show any reliable association between cardiothoracic ratio and left ventricular or right ventricular dysfunction on echocardiogram in antero-posterior films.
The syndrome of heart failure remains a clinical diagnosis and has become challenging due to an emphasis on early detection with fewer and less sensitive signs. Advances in understanding have led to a change in the nomenclature with an increasing emphasis on categorising patients into heart failure with reduced ejection fraction (formerly systolic heart failure) and heart failure with preserved ejection fraction (formerly diastolic heart failure). Clinical examination of patients with known coronary disease to try to detect left ventricular dysfunction showed sensitivities, specificities and positive predictive values for pulmonary crepitations of 13%, 91% and 27%; oedema on examination of 10%, 93% and 3%; and a raised jugular venous pressure of 10%, 97% and 2%. 27 Interestingly, previous studies have shown no correlation between the cardiothoracic ratio and markers of diastolic dysfunction. 28 Overall, studies appears to suggest that an increased or increasing cardiothoracic ratio may be useful as a surrogate of progressive left ventricular dilatation in patients with known left ventricular systolic dysfunction, 29 but our findings suggest that it has only a limited positive predictive value in the diagnosis of left ventricular systolic dysfunction. In our cohort, the negative predictive value was high, which may reflect the variety of reasons for requesting an echocardiogram.
There are several limitations of our study. This cohort of patients included all-comers with an in-patient request for echocardiography (including heart failure and non-heart failure indications) and a preceding chest radiograph. While this may introduce an element of ascertainment bias as the patients were obviously suspected of having cardiac disease, this should increase the pre-test probability and accurately replicates one commonly used method of using the cardiothoracic ratio. Not all the echocardiograms were purely for assessment of left/right ventricular dysfunction. We did not exclude chest radiographs on the basis of poor inspiratory effort. Changes in respiratory phase are known to affect the cardiothoracic ratio, but we included everyone as this is often overlooked when physicians (rather than radiologists) look at initial films. Additionally, a period of time passed between the initial chest radiograph and the echocardiogram. This was generally short but in some patients, intervening therapies may have caused alterations which then were noted on echocardiography later.
While we measured quantitative measures of left ventricular function on echocardiography, unlike other studies,17,18 we opted to use qualitative measures of left ventricular or right ventricular dysfunction as our primary endpoint, as this is predominantly what is in the mind of clinicians and has been shown to be equally reliable. 30 We used a cut-off of moderate left ventricular/right ventricular systolic dysfunction (rather than mild) to make the study clinically meaningful and eliminate subjective inter-observer variability in the assessment of left ventricular or right ventricular function. For practical reasons, it was not possible to provide data on inter- and intra-observer variability for assessment of echocardiographic parameters. However, all cardiac physiologists were accredited and performed echocardiograms based on American Society of Echocardiography recommendations. 22 Other pathologies causing left ventricular hypertrophy may be postulated to increase the cardiothoracic ratio, but previous studies have not found any correlation, thus limiting potential usefulness as a diagnostic tool. 28
Our study shows that in an inpatient population where the clinician suspects cardiac disease and requests an echocardiogram, the cardiothoracic ratio on postero-anterior chest film has moderate sensitivity and specificity but a poor positive predictive value in the diagnosis of left ventricular or right ventricular systolic dysfunction. The cardiothoracic ratio on an antero-posterior film was not able to detect left ventricular or right ventricular systolic impairment. In isolation, the cardiothoracic ratio should be at best regarded as ‘suggestive’ evidence for the diagnosis of heart failure.
Footnotes
Declarations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.