
Abstract
Lesson
In end stage renal disease patients on dialysis, the use of catheter as a vascular access is associated with a significant risk of sepsis compared to an arterio-venous fistula. Our case emphasizes the importance of having high index of suspicion for unusual complications in patients presenting with possible catheter-related blood stream infection and early use of complementary tools such as trans-oesophageal echocardiography whenever applicable.
Introduction
Sepsis is a major cause of death in end stage renal disease (ESRD) patients on dialysis, with estimated risk being 100- to 300-fold higher than the general population. 1 Infectious complications of the vascular access are an important cause of morbidity and mortality among these patients, and use of a catheter is approximately four times more likely to be associated with sepsis compared to an arterio-venous fistula. 2 While infective endocarditis is relatively common in end stage renal disease patients, 3 intracardiac fistula associated with catheter-related blood stream infection is exceedingly rare and we present one such case here.
Case report
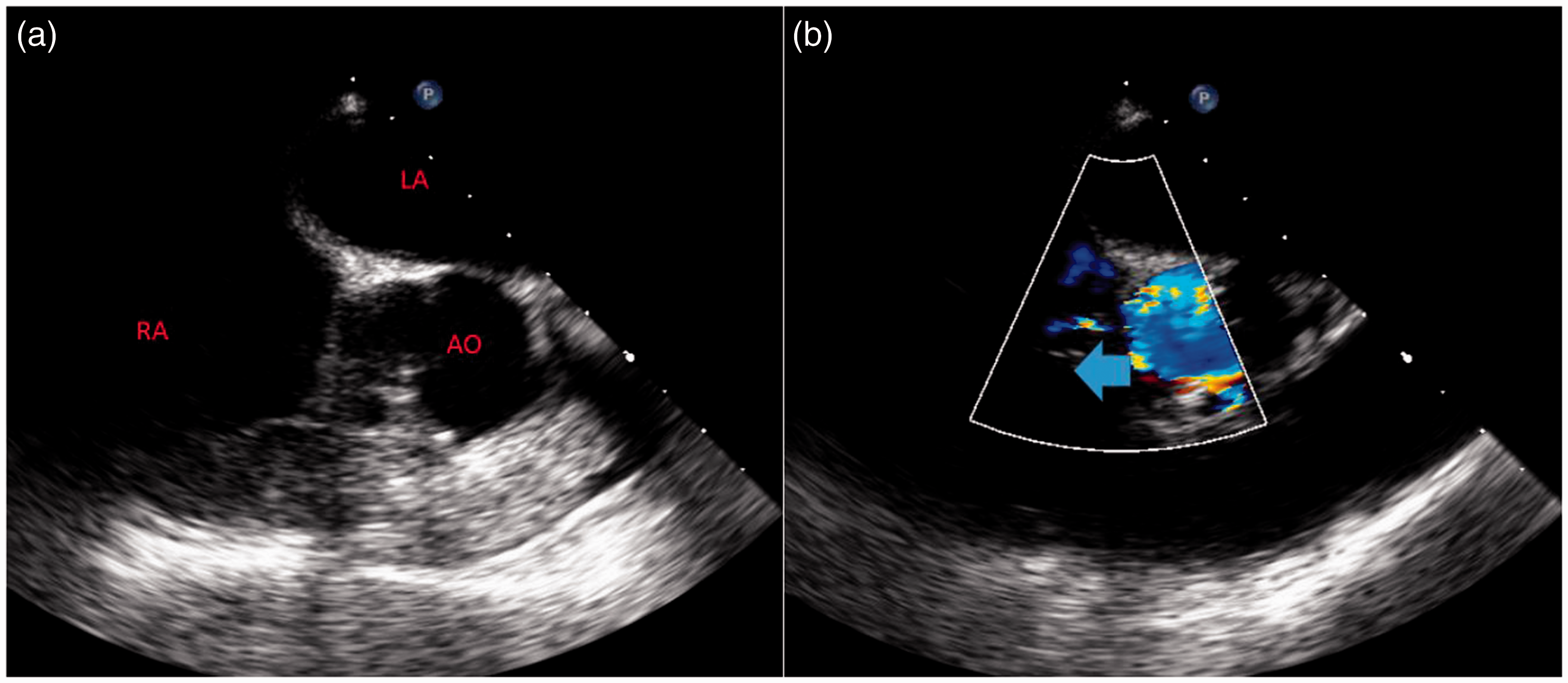
A 59-year-old African-American male with a history of end stage renal disease on haemodialysis for two years, hypertension and diabetes mellitus type 2 presented with intermittent chest pain and fever for two days. He had last haemodialysis session one day before via right internal jugular tunnelled catheter with no reported complications except for ‘feeling chilly’ while on the machine. He was febrile with a temperature of 101.4°F and hypotensive with a blood pressure of 94/58 mmHg. Physical examination revealed a systolic–diastolic apical murmur. Blood cultures were obtained both from the catheter and periphery, and he was started on empiric intravenous antibiotic therapy with vancomycin and piperacillin–tazobactam for presumed catheter-related blood stream infection. Electrocardiogram showed non-specific changes and cardiac markers were elevated. He was admitted and managed conservatively for non-ST elevation myocardial infarction, as he was febrile. Blood cultures grew Staphylococcus epidermidis and his antibiotic therapy was adjusted accordingly. On day 5 of admission, he developed ventricular tachycardia and pulseless cardiac arrest. Electrocardiogram showed ST elevation and he was taken to the catheterisation laboratory after revival and placement of temporary venous pacemaker. Cardiac catheterisation showed non-obstructive coronary artery disease. Trans-oesophageal echocardiogram showed findings suggestive of fulminant aortic insufficiency with possible periaortic abscess and a fistula connecting left ventricular outflow tract to the right atrium (Figures 1 and 2). His dialysis catheter was removed immediately and a temporary catheter was inserted for continuity of haemodialysis. The risks of surgical treatment were deemed to outweigh benefits and he was treated with intravenous vancomycin for six weeks followed by minocycline suppressive therapy. He remained afebrile and asymptomatic throughout the hospital course. Interestingly, transthoracic echocardiogram done before the cardiac event did not show the fistula or vegetation.
(a) Anatomical trans-oesophageal echocardiogram showing right ventricle (RV) and aorta (AO). (b) Trans-oesophageal echocardiogram demonstrating fulminant aortic insufficiency with mosaicism to the jet shown with an arrow. (a) Anatomical trans-oesophageal echocardiogram showing left atrium (LA), right atrium (RA) and aorta (AO). (b) Trans-oesophageal echocardiogram demonstrating flow from aorta to the right atrium suggestive of an intracardiac fistula indicated by an arrow.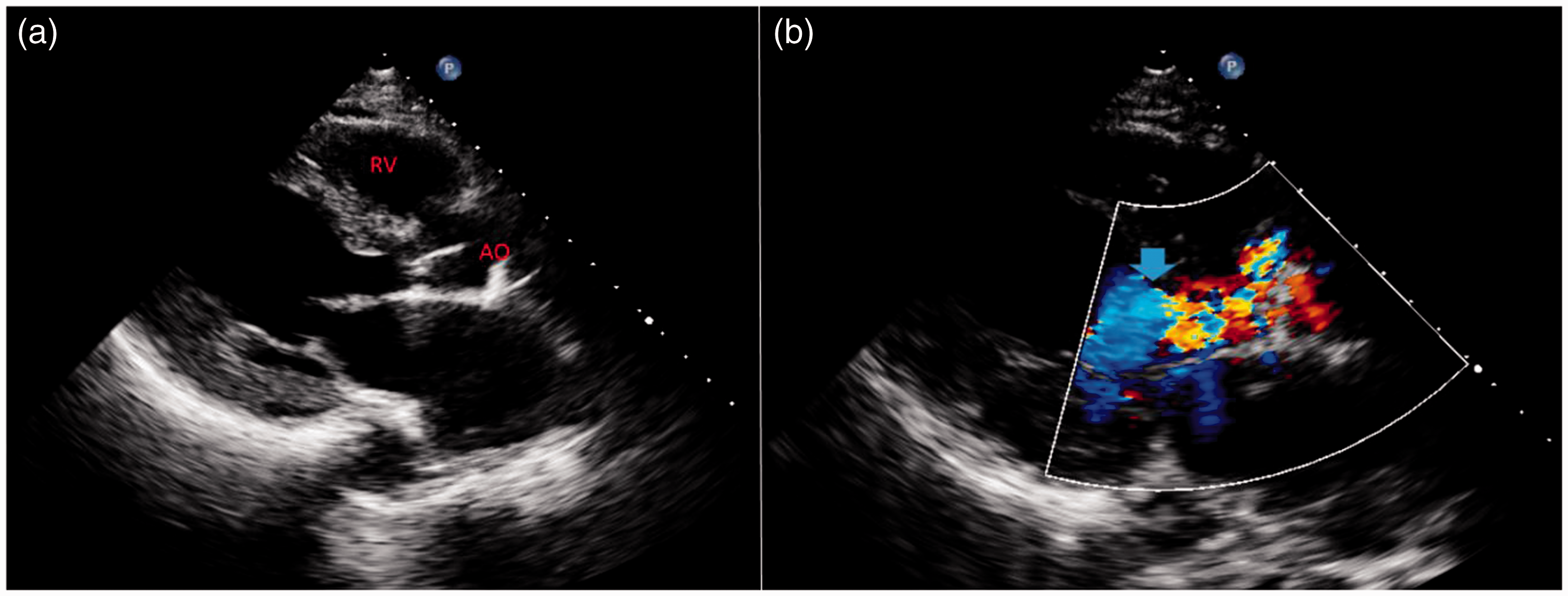
Discussion
The majority of bacteraemias in end stage renal disease patients are caused by infection of dialysis catheters. Compared to those with arterio-venous fistulas or grafts, the incidence of bacteraemia is significantly higher in patients with indwelling catheters. In a study including 472 end stage renal disease patients initiating haemodialysis with catheters, Shingarev et al. 4 have found that the incidence of catheter-related blood stream infection was 35% at 3 months, 54% at 6 months and 79% at 12 months. In some patients, bacteraemia leads to metastatic complications, such as endocarditis, osteomyelitis, epidural abscess, septic arthritis or other soft tissue abscesses. 5 As metastatic complications confer high morbidity and mortality, clinicians should pay close attention to patients’ symptoms and physical examination findings. In addition, early use of investigations such as trans-oesophageal echocardiography whenever applicable may help in early identification of unusual complications and prompt timely interventions. In patients with endocarditis, extension of infection from valvular structures to surrounding perivalvular tissue may lead to intracardiac abscess formation and communicate with the lumen of the aorta or the cardiac chamber. Aorta-to-right atrium fistula, as in our patient, is a rare complication of infectious endocarditis and is associated with higher mortality rates. Some patients would benefit from surgical treatment in addition to antibiotic therapy. However, the haemodynamic deterioration caused by this fistula and annular abscesses increased the technical difficulties and risks associated with surgical treatment. 6
Gram-positive organisms cause most dialysis catheter-related infections with Staphylococcus species accounting for about 35–81% of the cases. Enterococci and Gram-negative rods are responsible for most non-staphylococcal bacteraemias. 7 Most patients with CRBSI present with fever or chills, especially during haemodialysis. Purulence at the catheter insertion site or visible exit-site infection is a more specific sign of catheter-related blood stream infection but not always present. When these patients present with severe sepsis, haemodynamic instability, signs of exit-site infection or metastatic infection, immediate catheter removal is recommended in addition to empiric antibiotic therapy. 8 Empiric broad-spectrum antibiotic therapy usually consists of vancomycin and either gentamicin or third generation cephalosporin. Among the patients without indications for immediate removal of the infected catheter, antibiotic lock and/or catheter exchange over guidewire should be considered as adjunctive therapy to systemic antimicrobial therapy. The antibiotics must be tailored according to the sensitivity of the organism and the recommended duration is usually 2–3 weeks. Among patients with metastatic infections such as osteomyelitis or endocarditis, 6–8 weeks of therapy is indicated. 8
Footnotes
Declarations
Acknowledgements
None.
Provenance
Not commissioned; peer-reviewed by Sanjana Gupta.