
Abstract
Sodium glucose co-transporter 2 inhibitors lower blood pressure by osmotic diuresis and can be considered in diabetic patients with resistant hypertension.
Case presentation
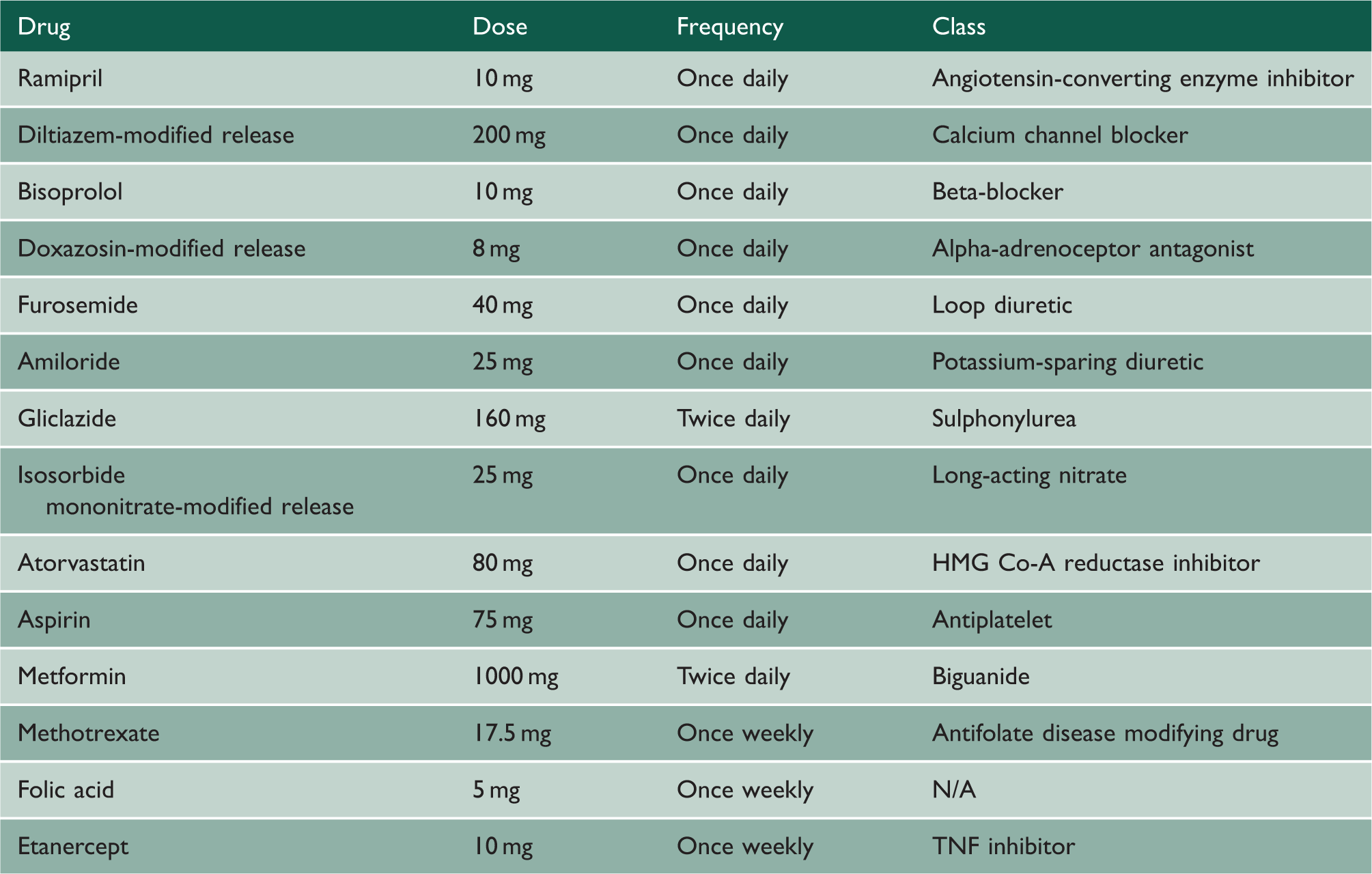
Medications the patient was taking prior to the addition of canagliflozin.
In view of apparent resistance to treatment, the patient was admitted to hospital for directly observed therapy in June 2013 to exclude non-adherence. His adherence was also confirmed on two separate occasions in 2014 when urinary drug screening became routinely available. Renal denervation (radio-frequency ablation of the renal sympathetic nerves surrounding the renal arteries) was conducted in October 2013. This had no effect, and in fact his blood pressure in June 2014 was higher with a mean daytime blood pressure of 181/105 mmHg.
Timeline of the patient’s blood test results, weight and clinic blood pressure in relation to canagliflozin dose.

At this point the canagliflozin was stopped as it was not felt necessary for his diabetes control and because of the reduction in estimated glomerular filtration rate. In the next clinic in August 2015, blood pressure measurement was again high, the lowest being 151/87 mmHg. In view of the apparent remarkable effect on the patient’s blood pressure, a decision was made in conjunction with the patient to restart the canagliflozin at a low dose of 100 mg daily and cautiously monitor the kidney function. After re-starting the canagliflozin 100 mg in August 2015, the blood pressure reduced to 138/86 mmHg in the next clinic. The blood pressure remained well controlled at 136/83 at the clinic visit in November 2015.
Discussion
Almost all of the glucose filtered by the glomeruli is reabsorbed, primarily in the early proximal convoluted tubule via action of sodium glucose co-transporter 2, a high-capacity, low-affinity transporter that is selectively expressed in the kidney. 1 Sodium glucose co-transporter 2 expression is increased in humans with diabetes mellitus and Zucker diabetic fatty rats, correlating with glomerular hyperfiltration and increased glucose reabsorption, as well as increased sodium reabsorption. 2 This contributes to sodium retention and hypertension in diabetic patients, the two often co-existing. There is also animal model evidence supporting a role for sodium glucose co-transporter 2-mediated sodium reabsorption in the development of hypertension: in hypertensive rats, angiotensin II has been shown to regulate the increase in sodium glucose co-transporter 2 expression via the angiotensin II AT1 receptor. 3
Canagliflozin and dapagliflozin were two of the first sodium glucose co-transporter 2 inhibitors to be approved in Europe and the United States for use in diabetic patients, and others soon followed. Our experience with the patient in this case study is expected to be a class effect, not specific to canagliflozin. Clinical trials with these agents have consistently shown beneficial effects not only on diabetes control but also on blood pressure and weight. They have been shown to produce a reduction in HbA1c of around 0.9%, a mean reduction in weight of 2.5 kg, a drop in systolic blood pressure of 4 mmHg and a drop in diastolic blood pressure of 1.6 mmHg.4–6 In the recently published EMPA-REG study, it has been shown that the sodium glucose co-transporter 2 inhibitor empagliflozin reduces cardiovascular mortality by 38% and all-cause mortality by 32%, in high cardiac risk type 2 diabetes mellitus patients. 5 It has also been shown to reduce heart failure mortality by 35% and this been attributed, in part, to effects on blood pressure, amongst other things. 7
Sodium glucose co-transporter 2 inhibitors have been postulated to reduce blood pressure via their osmotic diuretic action. 1 They work on a different site to loop diuretics and thiazides, which act on the thick ascending limb of the loop of Henlé and the distal convoluted tubule, respectively. Caution is advised when used in combination with loop diuretics such as furosemide due to risk of hypovolaemia, although concomitant use is not contra-indicated.
Typical characteristics of patients with resistant hypertension include co-morbidities such as obesity and type 2 diabetes, as well as obstructive sleep apnoea, older age, target organ damage and atherosclerotic vascular disease. 8 It could be argued that sodium glucose co-transporter 2 inhibitors can play a role in the management of such patients not only for their diabetes but also for their high blood pressure and obesity. However, such medications should be used under close supervision in patients with chronic kidney disease and in those taking a combination of diuretics.
Footnotes
Declarations
Acknowledgements
None
Provenance
Not commissioned; peer-reviewed by Terence Pang.