
Abstract
Objectives
This study aimed to examine if socioeconomic status could affect the likelihood of diagnosis, treatment and control of hypertension in diabetic hypertensive individuals.
Design
Cross-sectional nationally representative study.
Settings
Bangladesh.
Participants
This paper used data from the 2011 Bangladesh Demographic Health Survey. The analyses were based on the responses of 339 diabetes hypertensive individuals.
Main outcome measures
Diagnosis, treatment and control of hypertension.
Results
The age-adjusted prevalence of hypertension in diabetes individuals was 38.4% in the study population. Among diabetic hypertensive subjects only 65.7% had been diagnosed, 58.4% were receiving treatment and 42% controlled their hypertension. Individuals from high socioeconomic status (AOR 2.60; 95% CI 1.16–5.83) had an increased likelihood of reporting diagnosis of hypertension. Individuals from medium (AOR 2.22; 95% CI 1.11–4.46) and high socioeconomic status (AOR 3.47; 95% CI 1.59–7.58) had increased chance of receiving treatment. In addition, individuals belonging to high socioeconomic status (AOR 2.53; 95% CI 1.14–5.63) were more likely to report of controlling hypertension.
Conclusions
This study indicated that hypertension is more prevalent among diabetic patients. Furthermore, diabetic hypertensive patients from the low socioeconomic status group are also less likely to be diagnosed and also less likely to receive treatment for hypertension. In addition, diabetic hypertensive patients from the low socioeconomic status were less likely to control hypertension compared with an individual belonging to the high socioeconomic status group. This reduced likelihood of receiving proper treatment will lead to a rapid increase in the prevalence of macrovascular and microvascular diseases among diabetic hypertensive patients.
Introduction
Although diabetes mellitus (DM) is associated with considerably increased risk of cardiovascular, retinopathy and nephropathy diseases, the presence of hypertension in the DM individual strikingly increases the risk.1,2 People with both DM and hypertension have approximately twice the risk of cardiovascular diseases (CVD) as non-DM people with hypertension. 2 In patients with DM, the prevalence of hypertension is up to three times more as compared to patients without DM. 3 Clinical trials have consistently demonstrated the importance of hypertension control in patients with DM to the prevention of macrovascular and microvascular diseases. 4 Therefore, detection, treatment and control of hypertension are highly desirable in preventing or slowing down the progression of macrovascular and microvascular complications in people with DM. The progress of DM in Bangladesh is increasing at a very fast pace, 4% in 1990 to 10% in 2011, 5 and thus is likely to contribute to a significant burden of hypertension among this group and consequently increases the risk of CVD.
How socioeconomic status (SES) influences control and management of hypertension in the general population has been studied in a range of settings, with different samples.6–8 However, despite the clinical importance of the coexistence of DM and hypertension as comorbid conditions, the association of SES with diagnosis, treatment and control of hypertension in DM hypertensive patients has not been studied. Furthermore, although the relationship between SES and health has been well documented, there is a lack of clear understanding about the combined impact of different SES measures, for example, education and wealth. Although these two variables have often been analysed independently,9,10 they are interrelated to each other at an individual level in reality. We do know both education and economic status positively affect health, but we do not know how the relationship would turn out when we consider two variables at once. It is possible that a DM hypertensive person, who does not have higher education but has higher economic status, has a higher likelihood of controlling and management of hypertension. It could also be possible that a DM hypertensive person with lower economic status, but with higher education, would have a higher likelihood of controlling and managing hypertension.
In addition, the issue of multicollinearity may emerge when these two variables were analysed independently. However, it is believed that education contributes to the socioeconomic development, which implies a high correlation between education and economic status. Thus, to avoid the problem of multicollinearity and to gauge SES more accurately, there is need to combine education and wealth status into one. Based on these considerations, using the first nationally representative sample of Bangladesh, we analysed if SES could affect the likelihood of diagnosis, treatment and control of hypertension in DM hypertensive patients.
Methods
Data source
This study used data from the 2011 Bangladesh Demographic Health Survey (BDHS), conducted by the National Institute for Population Research and Training of the Ministry of Health and Family Welfare of Bangladesh from 8 July to 27 December 2011. 11 A nationally representative household-based sample was created through a stratified, multistage cluster sampling strategy, constructing 600 primary sampling units (207 in urban areas and 393 in rural areas).
A total of 17,964 households were selected for interview, and 17,141 interviews were successfully completed, achieving a household response rate of 98%. Testing of the biomarker component, including and blood pressure measurements, and blood glucose testing, is a relatively new addition to 2011 BDHS and is administered to one-third of the households. 11 In total 8835 residents (4311 women and 4524 men) aged 35 or older were eligible for blood glucose measurement in those households, and 7565 took part, yielding a response rate of 86% (89% of women and 83% of men). Of those participants, 879 had DM (fasting plasma glucose values of ≥7.0 mmol/L or currently taking medication to lower blood glucose). The 2011 BDHS used the HemoCue 201 + blood glucose analyzer in capillary whole blood obtained from the middle or ring finger from adults after an overnight fast for measuring fasting plasma glucose levels. 11
Among the DM participants 340 had hypertension (blood pressure levels ≥140 mmHg SBP or ≥90 mmHg DBP, or currently taking medication to lower their blood pressure). The 2011 BDHS used the LIFE SOURCE® UA-767 Plus Blood Pressure Monitor model to measure hypertension recommended by the World Health Organization (WHO).
12
The survey recorded blood pressure in the right arm of seated participants. Three measurements of both systolic and diastolic blood pressure were taken during the survey at approximately 10-min intervals between measurements. The average of the second and third measurements was used to report respondent’s blood pressure values. After dropping any with missing data related to treatment status (n = 1), a total of 339 DM hypertensive individuals were selected for our analysis (Figure 1).
From the original 8,835 eligible men and women aged 35 years and older, we obtained a final sample of 339 for diagnosis and treatment outcomes and 239 for control outcome for this study: 2011 Bangladesh Demographic Health Survey.
Measures
We analysed three outcome variables: diagnosis, treatment and control of hypertension among DM hypertensive individuals. We regarded participants as having been diagnosed with hypertension if they answered ‘yes’ when asked whether a doctor or any other health professional had told them they had hypertension. We considered DM hypertensive patients to be receiving treatment for hypertension if they reported currently using an antihypertensive medication. For respondents reporting diagnosis, or diagnosis and receiving treatment, we examined whether their hypertension was controlled, defined as blood pressure levels SBP <140 mmHg or <90 mmHg DBP. Binary variables were created to define each of the three outcome variables.
This study created a variable to define SES in the following manner. First, a binary variable was created to assess the level of the respondent’s education according to the formal education system in Bangladesh, as either lower educated (below secondary education; 0–5 years of schooling) or higher educated (secondary or higher education; ≥6 years of schooling). Second, a binary variable was created to assess the wealth status of the respondents, as either poor or non-poor. The BDHS wealth index was constructed from data on household assets, including ownership of durable goods and dwelling characteristics. Principal components analyses were used to assign individual household wealth scores. Each household was assigned a score and the sample was then divided into population tertiles: poor, middle, rich. 11 In this study, individuals who live in households that belong to any other wealth tertile except the poor are designated as ‘non-poor’. Finally, a composite variable of SES was created by combining wealth and education as follows: (1) low SES (poor and lower educated); (2) middle SES (either poor or lower educated); and (3) high SES (non-poor and higher educated).
This study also included several theoretically pertinent sociodemographic risk factors of control and management of DM and hypertension.
Statistical analyses
We estimated the age-adjusted prevalence of hypertension in individuals with DM by a direct standardisation method. Age-adjusted prevalence of diagnosis, treatment and control of hypertension among DM individuals were also calculated. We derived a reference population for the age-adjusted prevalence data by using the gender-specific subpopulation of persons who had DM.
We used absolute percent difference and relative percent difference to measure disparity between low and high SES groups. The Slope Index of Inequality (SII) and the Relative Index of Inequality (RII) were used to quantify socioeconomic inequalities of our measured outcomes. The SII was calculated as described by Mackenbach and Kunst. 13 The gradient was determined with linear regression whereby the relative rank of the socioeconomic measurement factor was taken as predictor variable and the respective age-adjusted prevalence as outcome variable. For the estimation of the RII, the SII was divided by the overall prevalence of each of the outcome variables. Analyses were conducted using Stata version 12.0 (StataCorp. LP, College Station, USA) to adjust for sampling weights based on the complex survey design of BDHS.
To adjust for clustering of observations at multiple levels, data were analysed by using logistic multilevel modeling procedures. 14 We specified a three-level model for binary response of each of the three outcome variables for individual i living in household j in cluster k of the form, π ijk : yijk ∼ Bernoulli (1, π ijk ). All models were created by using penalised quasi-likelihood approximation with second-order Taylor linearisation as implemented in MLwiN 2.30 software. Data of this study are reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology guidelines. 15
Ethical considerations
The data collection procedures for the BDHS were carried out with the approval of the ORC Macro-institutional review board. The survey protocol was reviewed and approved by the National Ethics Review Committee of the Bangladesh Ministry of Health and Family Welfare of Bangladesh. Before starting the interview, informed consent was obtained from individual respondents followed by an oral explanation by interviewers according to the guidelines of the BDHS. Participants were informed and instructed about the importance of fasting status prior to the investigations. Trained data collectors and biomarker staff performed face-to-face interviews in each of the selected households to obtain demographic and biomarker information about the household and family members. This study was considered to be exempt from a full review as it was based on an anonymous public use of a secondary data set with no identifiable information regarding the survey participants.
Results
Descriptive statistics
Descriptive statistics according to age-adjusted prevalence of diagnosis, treatment and control of hypertension and sociodemographic characteristics among diabetes hypertensive individuals aged 35 or older: 2011, Bangladesh Demographic and Health Survey.

aNumber of family members 7 or over
≥25 kg/m2. Numbers are unweighted and percentage are weighted
Summary measures of SES inequality and diagnosis, treatment and control of hypertension among diabetes hypertensive individuals aged 35 or over: 2011, Bangladesh Demographic and Health Survey.
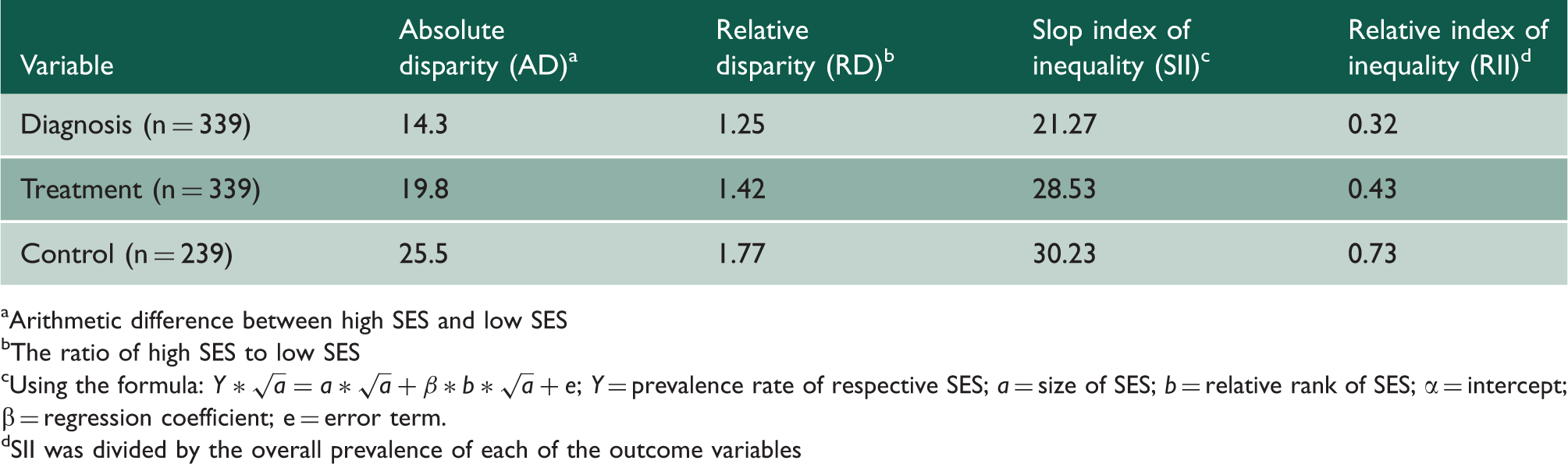
Arithmetic difference between high SES and low SES
The ratio of high SES to low SES
Using the formula:
SII was divided by the overall prevalence of each of the outcome variables
Multivariate analysis
Association between SES and diagnosis, treatment and control of hypertension
Adjusted odds ratios for associations between SES and diagnosis, treatment and control of hypertension among diabetes hypertensive individuals aged 35 or older: 2011, Bangladesh Demographic and Health Survey.

CI: Confidence interval; AOR: Adjusted odds ratio.
Number of family member s 7 or over; b≥25 kg/m2. Bold numerals indicate significant association.
Association between other covariates and diagnosis, treatment and control of hypertension
Participant’s age (60–64 or 65+ years) was independently associated with higher odds of diagnosis and treatment (Table 3). Among the DM hypertensive individuals those who had a large family were significantly more likely to be diagnosed and under antihypertensive medication. Being overweight/obese was associated with higher odds of diagnosis and being under antihypertensive medication and lower odds of controlling hypertension. Employed respondents were less likely to report of being under antihypertensive medication. In addition, DM hypertensive individuals aged 40–44 years were less likely to report of controlling hypertension (Table 3).
Discussion
Main finding of this study
The results from a nationally representative large survey in Bangladesh showed that hypertension is extremely common among Bangladeshi men and women with DM, with this disease occurring in more than one in three DM (38.4%) individuals. The study indicated that SES plays an important role in diagnosis and treatment of hypertension in DM hypertensive individuals in Bangladesh; it also appears to influence the likelihood of a DM hypertensive patient achieving normal blood pressure levels while being under antihypertensive medication.
Strengths and limitations of this study
The main strength of this study is that the data were collected from a large and randomly selected representative population. The data contained information on potential confounding factors, with a low proportion of missing information. Moreover, the BDHS ensures that interviewers were trained extensively and standardised measurement tools and techniques were used. The results of the current study should be considered in light of some limitations. First, due to the cross-sectional nature of this analysis, temporal order cannot be determined. Second, because our selection of variables was constrained by the preexisting BDHS data, we were unable to include additional, potentially important variables related to DM and hypertension, such as quantity and quality of diet, smoking status of the patients and physical activity. Third, the study can be criticised for using an indirect measure of household wealth. However, due to unavailability of reliable and comparable income or consumption data across households of all social classes, an asset-based index is generally considered as a good proxy for household economic status.
Finally, the estimated prevalence of hypertension might be underestimated because only persons who had measured high blood pressure during the examination and those who reported taking pharmacologic treatment to achieve control of hypertension were included in the analysis. Certain participants who might have received a diagnosis of hypertension previously but who had normal blood pressure measurements during the examination, perhaps as a result of lifestyle habits (e.g. diet and exercise), were not included as having hypertension in the analysis.
Comparison with other studies
The obtained high age-adjusted prevalence of hypertension among DM patients indicates an impending pandemic of diabetic cardiovascular diseases in Bangladesh with its potential economic consequences. The present study revealed that 42% of DM hypertensive patients who were receiving antihypertensive medication could control their hypertension. Because we used a representative community sample, our results are not directly comparable to the prevalence of other small scale and local studies. However, this figure is much lower than the previous small scale studies (52.9–80.1%)16–18 conducted in several developing and developed countries. By considering these situations, population-based awareness raising about hypertension and effective education among DM patients are necessary in Bangladesh.
This study indicated that DM hypertensive individuals belonging to the low SES group were less likely to diagnosis and also less likely to be under antihypertensive medication. These findings are in accordance with some of the previous studies conducted in both developed9,19 and developing nations. 20 There might be some barriers to the effective treatment and diagnosis of hypertension among DM hypertensive individuals belonging to the lower SES group in Bangladesh. These include failure to understand the importance of adhering to the treatment of hypertension, lack of family support, inadequate health facilities for diagnosis, insufficient specialist services for the management of DM, the absence of health educators, a costly and complex transportation system from village to city and a lack of health information. 21 Another potential barrier may be due to the discrimination by health-care providers and office staff. Clinicians may be busy only with managing diabetes for people with lower SES and consequently would not be willing or able to increase the antihypertensive medications. A study in Europe revealed that as the treatment of diabetes became more sophisticated, individuals with higher SES tended to respond to new treatment practices and benefited more than individuals with lower SES. 22
Another important finding is that the low SES group showed a lower probability of having normal blood pressure levels under treatment. Low literacy, lack of structured education and insecure economic status of DM hypertensive patients belonging to the low SES group lead to the dominance of incorrect beliefs about hypertension and its care. 23 These beliefs may have serious consequences, amounting to stopping the treatment or refusing the diagnosis of hypertension and thereby increasing the chance of uncontrolled hypertension. The relationship between SES and control of hypertension should be explored further and the reasons for the particularly low rates of control in individuals of low SES should be determined.
In the multivariate analysis, we found that old age (60 years or over) was independently associated with higher hypertension diagnosis and treatment, which is consistent with other reports.24,25 In contrast, the higher diagnosis and treatment levels among the older age group did not correspond to better hypertension control. In fact, the older adults, on the contrary, were less likely to have their hypertension adequately controlled compared with younger adults despite their higher awareness and treatment rates. A possible explanation might be that the older people may pay more attention to their health but lack financial means to afford costly antihypertensive drugs. 26 The higher control rates among traders may reflect their ability to access medical care, and ability to afford antihypertensive medications.
Another interesting finding is that living in a large family was significantly related to higher hypertension diagnosis and treatment. There may be a number of reasons for this. DM hypertensive individuals from a large family may receive more familial support compared with those from a small family. They may have more contact with family members and receive encouragement to seek care. Our findings also show that obesity was associated with higher levels of diagnosis and treatment but lower levels of hypertension control. These findings are consistent with other reports,27,28 It has been suggested that obesity positively influences blood pressure checking and prescription of medication for intervention, and hence, higher awareness and treatment levels. This study shows that employed persons were less likely to receive treatment. The possible reason may be due to the fact that employed persons in our sample data were less likely to suffer from hypertension compared with the unemployed individual. Moreover, an additional analysis was performed in our study to support this hypothesis, and DM hypertensive patients with jobs were found to have a low prevalence of hypertension compared with those who had no jobs.
Implications for practice and further research
The present findings highlight the need for strategies, programmes and policies that aim to combat hypertension among DM hypertensive individuals. Special attention should be given to low SES groups most affected. Such programmes can include interventions to improve the knowledge, attitude and behaviors of all sectors of the community including patients and health professionals in the context of prevention, early diagnosis, adherence to treatment and control of hypertension. Further longitudinal research is needed to fully tease apart this complex relationship and understand the underlying mechanisms.
Conclusions
This study indicated that hypertension is more prevalent among DM patients. Furthermore, DM hypertensive patients from the low SES group are also less likely to diagnose and also less likely to receive treatment for hypertension. In addition, DM hypertensive patients from the low SES group were less likely to control hypertension compared with the individuals belonging to the high SES group. This reduced likelihood of receiving proper treatment will lead to a rapid increase in the prevalence of macrovascular and microvascular diseases among DM hypertensive patients.