
Abstract
Lesson
In neurologically intact patients with isolated tuberculosis of the posterior spinal elements, surgical intervention can be of benefit in select patients by reducing instability, deformity and late complications.
Introduction
Tuberculosis (TB) has been described as an ancient infectious disease, with evidence being discovered in centuries-old skeletal remains. 1 In recent decades, there has been a significant resurgence of TB, causing 2–3 million deaths annually worldwide. 2 According to the Health Protection Agency Enhanced TB Surveillance Report, in 2011, the incidence of active TB in the UK was 14.4 per 100,000 population. 3
Spinal TB is a relatively uncommon condition; although its true incidence is uncertain, it is thought to occur in 1.7% of the population worldwide. 4 It is a disease of young active adults with concomitant issues of deformity, and hence has an economic influence. It typically presents with back pain and/or neurological deficit and deformity. The infection begins in the vertebral body and spreads to adjacent vertebra by extending beneath the anterior longitudinal ligament. 5 Involvement of the posterior elements is considered rare, particularly in isolation, infection is usually localised to the vertebral body. In spinal TB patients, the incidence of isolated posterior elements disease is between 2 and 3%.6,7
There is great controversy as to the optimal management of spinal TB. Currently, surgical treatment is generally only indicated in cases of instability, deformity or neurological deficit. 8 As such, ambulatory chemotherapy remains the mainstay of treatment for spinal TB. 9
Despite this, we report a case of isolated TB of the posterior spinal elements in a neurologically intact patient, on whom surgery was performed.
Case report
A 34-year-old Indian woman presented to her general practitioner with a one-month history of a painful midline lump over the lumbar region of her back. She was suffering from a sore throat and headache. The patient immigrated to the UK from India in 2009. She had no medical history and was HIV-negative. On examination, the lump was firm with a central groove, and was tender. The differential diagnosis at the time was a soft tissue lump/lipoma. There was progressive growth of the lump with increasing pain over the following months. The patient was referred for an ultrasound scan in January 2011, which showed a bilobed cystic lesion. She also had a chest X-ray (CXR) and computed tomography (CT) chest scan, which revealed a lesion on the fifth left rib. In February 2011, the patient underwent magnetic resonance imaging (MRI) of the whole spine. The results confirmed a bilobed cystic lesion, extending from the spinal canal posteriorly with involvement of the L1 spinous process on either side of the midline, spanning T12/L1 to mid-L3 levels (Figure 1). The MRI scan was reported as a possible complex meningocele. The patient was referred to neurosurgery at this time.
(a) Sagittal and (b) transverse view of MRI scan showing a bilobed cystic lesion spanning T12/L1 to mid-L3, with involvement of the L1 spinous process. The lesion measured 9.6 × 3.8 × 5.6 cm.
On further questioning it was found that the patient had no history of chest symptoms such as breathlessness, cough or chest pain. On a visual analogue scale from 0 to 10, with 0 representing ‘no pain’ and 10 representing the ‘worst pain imaginable’, her average low back pain (LBP) was 8/10 and her worst LBP was 9/10. She had an Oswestry Disability Index (ODI) of 50%. On examination, she was not obese. She had a normal gait and normal overall sagittal and coronal balance of the spine. Upper and lower limb motor and sensory examinations were normal with no pathological reflexes. The patient did have an obvious swelling on the lower back, in the midline, which was firm, had a central groove and did fluctuate. Laboratory tests revealed a C-reactive protein (CRP) of 27.5 mg/L (normal range 0–10 mg/L) and an alkaline phosphatase of 78 IU/L (normal range 20–140 IU/L). The patient underwent a CT scan of her lumbar spine (Figure 2). The results of this, as well as the previous chest CT and CXR, in combination with the patient's ethnic background, suggested TB as the probable diagnosis. At this stage, the patient had no deformity of the spine or any neurological symptoms.
(a) Sagittal and (b) transverse view of CT scan showing bony involvement of the L1 spinous process.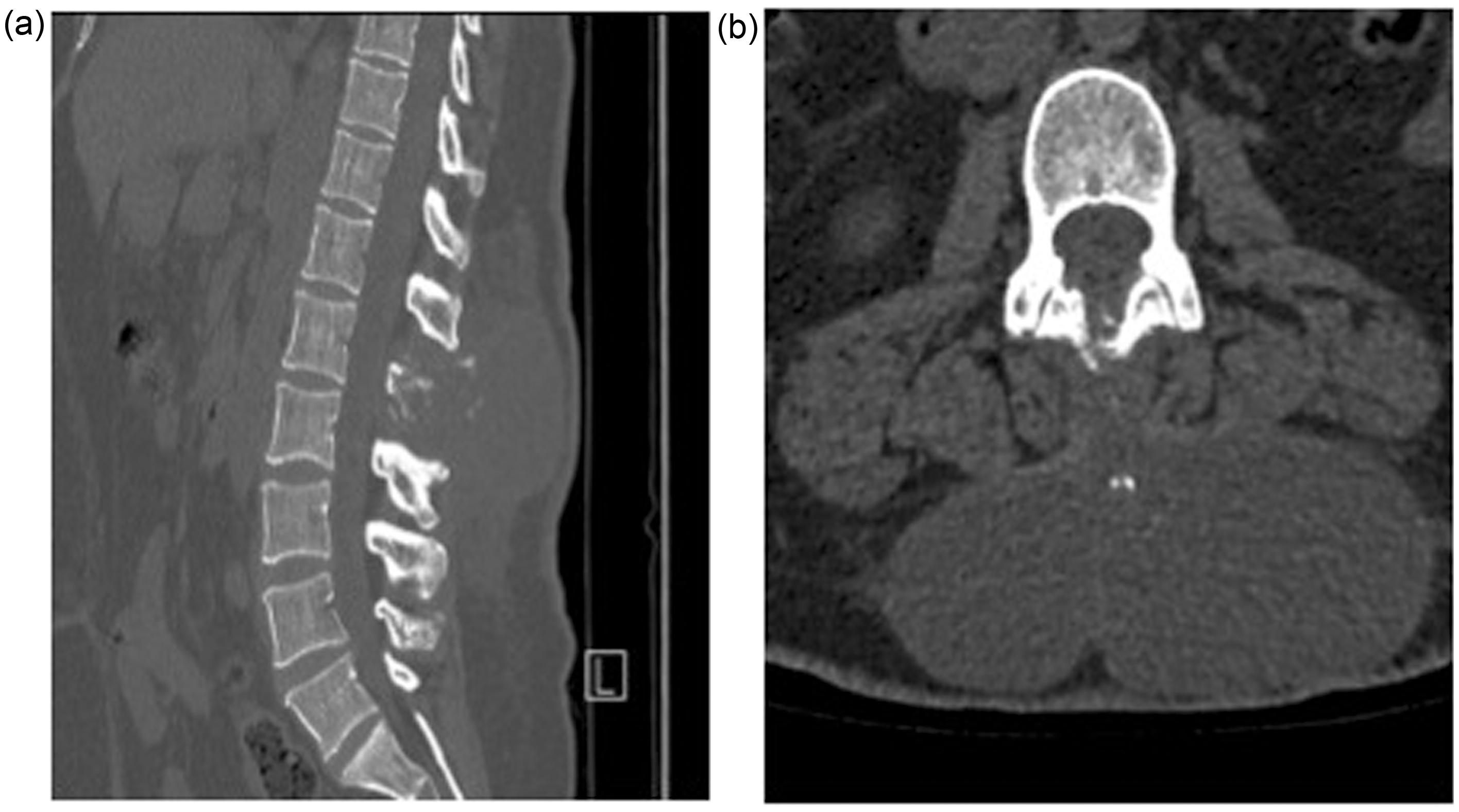
Surgery for the L1 posterior paraspinal abscess was undertaken in April 2011. This was carried out under general anaesthesia with the patient in the prone position on a Montreal mattress. The abscess was aspirated prior to opening; 120 mL of straw-coloured fluid was extracted. Upon incision, findings included pus and a granular abscess bed. The L1 spinous process was deep in the bed. A washout with 3 L of normal saline was performed. Fluid and bone were sent for biopsy. There were no surgical complications and the patient was discharged home six days later. Her cultures were found to be positive for TB, and on advice from microbiology, ambulant chemotherapy was commenced.
At six weeks' follow-up, her MRI images showed resolution of the cystic lesion (Figure 3). Her average LBP was now 1/10 and worst LBP was 1/10. Her ODI was 16%, and CRP 7.5 mg/L. There was a marked improvement in her functional ability, judged by her self-assessment in performing activities of daily living (Table 1). At latest follow-up in October 2012, the patient was found to have no deformity of the spine and no neurological deficit. By that time she had received her 12-month course of anti-TB chemotherapy. Her CRP in July 2012 was 6.3 mg/L. She did have symptoms of pain in her chest and legs. At this stage, there was no evidence of worsening of the spinal condition. The senior author thought in view of her recent vegetarian diet and her racial origin this may be due to a deficiency in vitamin D. Her blood results later showed vitamin D levels to be 8 nmol/L, she was started on vitamin D supplements. She also had a low thyroid stimulating hormone, 7.24 mLU/L, and normal free T4, 13.8 mLU/L. A referral to an endocrinologist was recommended. The patient remained under spinal review for two years following her surgical intervention.
(a) Sagittal and (b) transverse view of MRI scan showing resolution of cystic lesion, with some residual inflammation in the abscess bed. Preoperative and postoperative assessment of activities of daily living. Patient was required to indicate whether she was ‘limited a lot’, ‘limited a little’ or ‘not limited at all’ when performing the above activities of daily living.

Discussion
We presented a case of a neurologically intact patient with TB of the spine. In such patients, surgical treatment is rarely indicated, ambulant chemotherapy forms the mainstay of treatment. 9 However, due to the atypical anatomical location of her lesion, as well as her symptomatology of pain and loss of function, we decided that the best mode of management for our patient would be surgery.
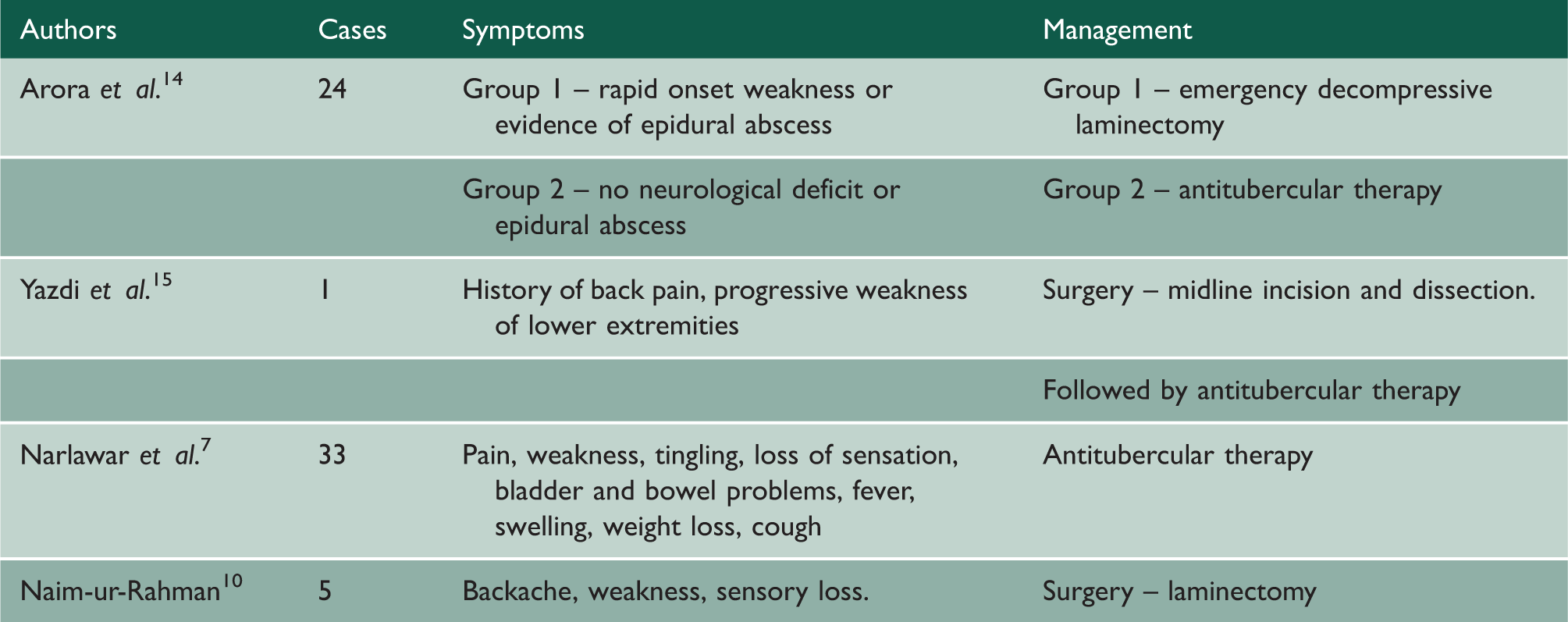
Vertebral TB is usually located in the anterior body, involvement of the posterior elements is considered rare, particularly in isolation.6,7 In this case, the infection was seemingly centred on the spinous process and lamina at one level with a soft tissue mass passing posteriorly, breaching the lumbar fascia into the abscess cavity. Two hypotheses exist explaining this atypical presentation: (1) Spread of the mycobacterium from a primary focus through the Batson venous plexus.6,7,10 This network of veins located in the epidural space contains no valves to control the flow of blood. Increased pressure in the body cavities can lead to retrograde flow of blood from the infected viscera to the vertebral venous plexi. The posterior external venous plexi anastomose freely with the other vertebral venous plexi and hence infection could pass to the posterior veins and hence to the posterior spinal structures by this mechanism. (2) Infection of immunocompromised patients. In recent decades, atypical forms of TB have been increasingly reported in HIV-positive patients.11,12 Narlawar et al. 7 tested 21 of their patients with isolated TB of the posterior elements for HIV antibodies, and found seven (33.3%) to be positive. Spread through the lymphatic system 10 and multidrug resistant TB 13 are less-widely accepted theories for atypical spinal TB.
Studies reporting cases of isolated TB of the posterior spinal elements in the last 33 years.
There remains great controversy regarding the management of a neurologically intact, non-deformed patient with spinal TB. The Medical Research Council studies recommended ambulant chemotherapy as the gold standard management for such patients. However, detailed analysis of the results later revealed that in certain patients surgery can reduce long-term kyphotic deformity and offer faster resolution. 16 Severe kyphosis can lead to neurological deficits and late complications, which can be difficult to treat. Early surgical intervention could potentially stop this progression. 17
Tuli 18 proposed the ‘middle-path’ regime for the treatment of spinal TB. Patients should initially be treated with anti-TB chemotherapy; surgery should be reserved for those who are refractory to treatment. However, he believed that lesions affecting the posterior elements of the spine are an indication for immediate surgery, due to the dangerous development of superficial abscesses or sinuses and secondary infection of the meninges. In the case of our patient, we performed relatively minor surgery, and ambulant chemotherapy was later commenced on the advice of microbiology.
The majority of patients with TB respond well to chemotherapy; however, up to 10% of patients with central nervous system disease report a paradoxical response, defined as a worsening of pre-existing TB and/or the development of new lesions, in a patient who initially responded well to therapy.19,20 This percentage can rise to 30% in HIV-positive patients, the same patients who are likely to have atypical spinal TB, further supporting our decision for early surgical intervention.
Due to its rarity and unfamiliarity, isolated TB of the posterior elements tends to be a delayed diagnosis, 15 as in this case. This delay makes simultaneous involvement of both the posterior and anterior elements via anterior spread more likely. Dual involvement leads to severe spinal instability. For pure anterior fixation to be successful, an intact posterior tension band is biomechanically advantageous, which is improbable if there is posterior involvement. 13 Therefore, hypothesised early surgical intervention can reduce the risk of deformity, instability and neurological deficit.
Our patient showed significant improvement in functional state following surgery (Table 1). Her ODI dropped from 50% to 16%, representing a significant clinical improvement. 21 This can probably be attributed to the drainage of the abscess, which relieved the pressure compressing the paraspinal muscles hence allowing more normal function and reduced pain. The paraspinal muscles are crucial for mobility and range of movement. We chose not to perform a laminectomy in this patient, to maintain natural anatomical barriers preventing the spread of infection anteriorly and into the epidural space and/or anterior column. Also, a full laminectomy causes disruption of the tension band increasing the likelihood of deformity. It is thought that since TB infection can form chronic sinuses that incision and drainage of TB abscesses can be problematic. We did not find this in our case.
Early surgical management in certain patients can reduce instability, deformity and late complications. We recommend patients with isolated TB of the posterior elements be reviewed on a case-by-case basis when determining management.