
Abstract
Summary
Objectives
The fetal origins of adult disease hypothesis describes associations found for fetal or early-life exposures with cardiovascular risk and disease in adulthood. The extension or not of these associations into old age has received less attention. We investigated if maternal health and family circumstances were associated with cardiovascular risk factors and cardiovascular disease (CVD) in late life and discuss results in light of possible selection effects and measurement error.
Design
A retrospective cohort study based on community survey. We examined 224 possible associations between anthropometric measures, maternal health information and family socioeconomic status at birth versus CVD and CVD-related risk factors 72–74 years later.
Participants
Of 3341 participants in a community survey of people aged 72–74 years, we were able to trace birth records from a historical archive in a broadly representative subsample of 480.
Setting
Bergen, Norway
Main outcome measures
Established cardiovascular risk factors and indicators of CVD.
Results
Only 11 (4.9%) of these associations were found to be statistically significant, and no strong or consistent patterns in the associations between exposures and outcomes were found.
Conclusions
There was little evidence in this relatively elderly sample for an association between early life factors and CVD outcomes of clinical or public health relevance. Further research is required to confirm the extent to which a diminution of early life influences into old age, if genuine, can be accounted for by selective mortality, systematic bias or by dilution of effects due to competing risk factors.
Keywords
Introduction
The fetal origins of adult disease (FOAD) hypothesis1,2 suggests that early influences, especially intrauterine environmental exposures, affect individuals irreversibly during particular periods, and consequently increase the risk of specific diseases in adult life. Early studies in this field investigated if weight and head circumference at birth could predict cardiovascular disease (CVD)-related outcomes in adult life, 1 such as increased blood pressure and increased mortality from CVD and stroke.1,2 Lower birthweight3,4 and paternal social class 5 have been found to be associated with incident CVD in adulthood. Inverse relationships have also been found between birthweight and adult serum cholesterol concentrations, risk for type-II diabetes and hyperlipidaemia. 2
It has, however, been more challenging to extend this paradigm and examine the same factors as risks for disease in old age. For one, there has been a lack of reliable data combining exposure status at birth and health outcomes in late life. The few studies that have investigated the hypothesis in relation to old age (≥65 years of age)6–14 have often had limitations such as self-reported birth information6,8 or restriction by gender.6,8,11,14 To the best of our knowledge, no previous studies have investigated the FOAD hypothesis in a population above 70 years of age specifically.
Taking advantage of a birth record archive in an area covered by a community survey of older people, we constructed a retrospective cohort study by linking information from the survey of people aged 72–74 years with participants’ birth records. Based on this linkage, our aim was to investigate the extent to which birth measures, maternal health and family circumstances were associated with cardiovascular risk factors and CVD in old age. Given the long temporal gap between exposure and outcome, and the paucity of any intervening information, a secondary aim was to consider the methodological challenges involved in this type of study design and use the present results to highlight and discuss these.
Methods
Study population
The sampling frame for this study comprised all 3341 participants in the old age cohort of the population-based Hordaland Health Study (HUSK) which has been previously described. 15 In summary, all residents of Bergen city or neighbouring areas born between 1925 and 1927 were invited to participate in a general physical examination and to complete questionnaires on sociodemographic status, general health and health-related behaviour. HUSK was conducted from 1997 to 1999 as a collaboration between the National Health Screening Service, the University of Bergen and the local health services.
In the Norwegian Population Registry, all inhabitants of Norway are registered with a personal identification number. Using this individual identifier, the names (and maiden name for females), date of birth, place of birth and parents’ names (if available) of HUSK-participants were retrieved. This information was used to retrospectively trace the participants born in Bergen to their birth records located at the Regional State Archives of Bergen. These records contain detailed information about the pregnancy, the birth and the mother’s health recorded contemporaneously by midwives and obstetricians. As these records were used in the educational training of midwives, they are considered to be of a high quality. 16 Of the 3341 participants from the old age cohort, we were able to trace 480 (14.4%), which constituted the final study sample aged 72–74 years (mean 72.3). More details about the establishment of the retrospective cohort has been previously described. 17
During the late 19th century and early 20th century, Bergen city expanded geographically and went from a semi-rural city to a city with more modern characteristics, and the secondary and tertiary industry expanded. 18 This industrial change was mostly due to growing manufacturing but also related to an increase in commerce, shipping, transport and service industry. 18 As a consequence, three social classes began to dominate in Bergen during the same period, upper, middle and lower, with large differences in income, housing standard and diet. The upper class was characterised by industry proprietors, importers, wholesale dealers and financers. The middle class consisted primarily of merchants, craftsmen and officials, while the lower class comprised regular workers or artisans. 18
During the summer of 1918, the Influenza pandemic reached Bergen, and it is estimated that 45.3% of the population became infected between July 1918 and March 1919. 19 For Norway as a whole, the excess mortality was 5.7 deaths per 1000 inhabitants, 20 and 65% of those who died were between 15 and 40 years of age. 21 For births in 1925–1927, life expectancy in Norway has been estimated as approximately 67 years for males and 74 years for females. 21
Early life factors – information obtained at birth, 1925–1927
The available birth records in the Regional State Archives of Bergen were viewed and coded blind to all HUSK measures. The following information was abstracted from the records: gestational age (weeks), birthweight (kg), birth length (cm), head circumference (cm) at birth, ponderal index (PI; calculated from weight and length) and mother’s mean pelvic size (cm). The following binary variables were derived from individual free text fields: any recorded disease in the mother (yes/no), family history of coronary heart disease (yes/no) and tuberculosis (yes/no), the state of mother’s teeth (poor/good), mother’s condition after birth (poor/good), complications during birth (yes/no), mother’s general somatic state at discharge (poor/good), marital status (married/unmarried), socioeconomic status (SES, based on father’s occupation; lower/middle) and type of payment for the hospital stay (health insurance/other). Date of birth was also available for all of the participants, and this information was used to differentiate between being born during the summer (March–August) and winter (September–February) season.
Demographic information – follow-up from HUSK at age 72–74
As a crude assessment of potential demographic differences between the participants we were able to trace and the rest of the HUSK-participants, self-reported level of educational attainment and general health was obtained from HUSK. Level of educational attainment was divided into ‘compulsory only’ and ‘post-compulsory’, while general health was divided into ‘poor’ and ‘good’.
CVD and risk factors for CVD – follow-up from HUSK at age 72–74
The following outcomes from HUSK were analysed: measures of body mass index; hip and waist circumference; systolic and diastolic blood pressure; non-fasting serum levels of triglycerides, total cholesterol, high-density lipoprotein (HDL) cholesterol and glucose; self-reported diabetes, previous CVD incidents (including stroke, infarction, embolus and any CVD-related surgery) and use of nitroglycerin or antihypertensive medication. Based on the measured information available, we defined a metabolic score according to a modified version of the US National Cholesterol Education Program (NCEP) criteria for metabolic syndrome. 22 As information about fasting glucose was unavailable, this criterion was excluded. The participants were given a score from 0 to 4 for each fulfilled criterion according to NCEP, with ≥3 indicating a ‘high metabolic score’. 22
Statistical analyses
A post hoc power analysis indicated that we would be able to detect a small to medium effect size for continuous (a correlation of 0.13), binary associations (Cohen’s w of 0.16) and the combination of the two (Cohen’s d of 0.35), given a power of 80%. 17 The sample was described and HUSK participants with traceable birth records were compared to the remainder of that sample. Age- and gender-adjusted associations were then investigated between exposures and outcomes employing linear regression models. In addition to the age- and gender-adjusted associations, crude associations and gestation-adjusted associations were computed, yielding similar results (data not shown). Because of criticisms of publication bias concerning previous FOAD findings, 2 our approach was to investigate and report all associations between exposures and outcomes, taking into account the number of significant associations that would be expected through chance alone but also investigating any consistency across a given exposure or outcome.
Results
Comparison between the analysed sample and the remainder of the HUSK sample
Differences on outcomes between HUSK participants with birth journal information and participants without.

Significant associations in bold.
NCEP: The US National Cholesterol Education Program Adult Treatment Panel III.
*mg/dL.
†Non-fasting glucose, mg/dL.
Sample characteristics
Sample characteristics at birth obtained from medical records.

*The mean of the interspinous distance, the intercristal distance and the external conjugate in centimeters.
†Including, but not limited to, prolonged labour, abnormal presentation, manual extraction and episiotomy, uterine rupture, discoloured amniotic fluid, abnormal fetal souffle and placenta praevia.
‡Date of birth was available for all of the participants in the old age cohort of HUSK.
Association between early life factors and CVD-related outcomes at age 72–74
Age- and gender-adjusted associations between continuous risk factors at birth and CVD-related outcomes at age 72–74, unstandardised coefficients.
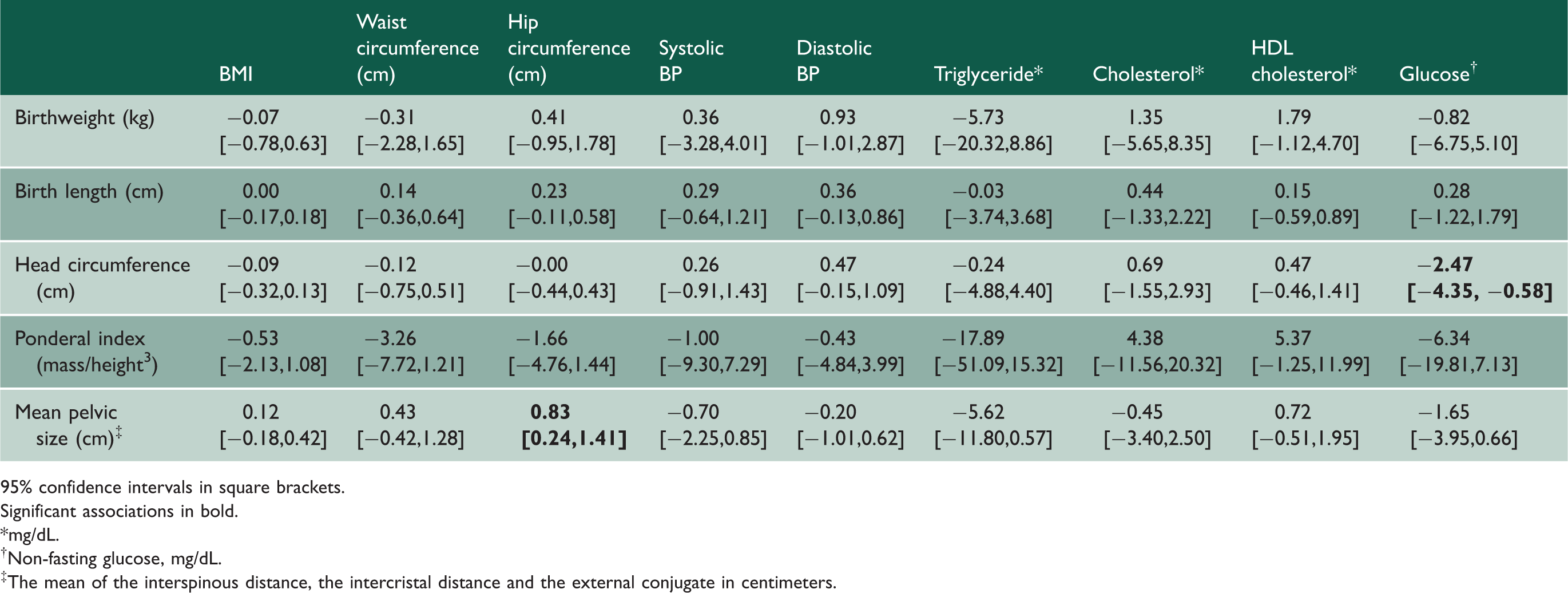
95% confidence intervals in square brackets.
Significant associations in bold.
*mg/dL.
†Non-fasting glucose, mg/dL.
‡The mean of the interspinous distance, the intercristal distance and the external conjugate in centimeters.
Age- and gender-adjusted association between binary risk factors at birth and CVD-related outcomes at age 72–74, unstandardised coefficients.

95% confidence intervals in square brackets.
Significant associations in bold.
*mg/dL.
†Non-fasting glucose, mg/dL.
‡Including, but not limited to, prolonged labour, abnormal presentation, manual extraction and episiotomy, uterine rupture, discoloured amniotic fluid, abnormal fetal souffle and placenta praevia.
Age- and gender-adjusted associations between risk factors at birth and binary CVD outcomes at age 72–74, unstandardised coefficients.

95% confidence intervals in square brackets.
Significant associations in bold.
NCEP: The US National Cholesterol Education Program Adult Treatment Panel III.
*The mean of the interspinous distance, the intercristal distance and the external conjugate in centimeters.
†Including, but not limited to, prolonged labour, abnormal presentation, manual extraction and episiotomy, uterine rupture, discoloured amniotic fluid, abnormal fetal souffle and placenta praevia.
Considering outcomes where more than one age- and gender-adjusted association was found, increased glucose blood levels were associated with mother’s condition after birth being reported as bad (p = 0.042), in addition to the association with head circumference. Also, increased hip circumference in old age was associated with increased mother’s pelvic (p = 0.006) size and reports of tuberculosis in mother’s family (p = 0.045).
In addition, a higher paternal SES was associated with decreased BMI in old age (p = 0.029), and mother’s condition at discharge being rated as bad was associated with decreased systolic blood pressure. The point estimates of the crude associations did not differ substantially from the age- and gender-adjusted associations presented in Table 3 to 5.
Discussion
In this study, we examined 224 possible associations for anthropometric measures, maternal health information and family socioeconomic status at birth with established CVD and related risk factors 72–74 years later. A mere 4.9% of these associations (n = 11) were statistically significant (p<.05) in age- and gender-adjusted analyses, and no strong or consistent pattern of associations was found with respect to exposures or outcomes. As with any empirical study, chance, bias and confounding should be considered as potential explanations. The significant associations were in summary no more than would be expected by chance, applying an alpha level of 0.05. Our analysis had sufficient statistical power to detect small to medium effects sizes, but by testing 224 associations, we increased the risk of type I error. The data, taken as a whole, suggest no substantial association between early life factors and cardiovascular health in late life in our sample. Employing Bonferroni adjustments for multiple testing would render even more of the significant associations non-significant and further strengthen the likelihood that there are few substantial associations between early life factors and late life CVD health. There are, however, a range of design challenges and selection effects that may have influenced our results, and these will be discussed in depth later.
Strengths of the present study
Having access to birth records from the 1920s and the possibility to link this information to a population-based health survey in the late 1990s enabled a follow-up in the range of 72–74 years which, as mentioned, was longer than has been available in any previous cohort. Both the exposure and the outcome sources contained detailed information and the gathering of information was unlikely to have been biased in any particular direction. The birth records were used in the education of midwives under the supervision of the head physician and included detailed anthropometric measures, as well as information about maternal health and circumstances, the birth process and the early postnatal period. The HUSK study included many physiological measures in addition to self-reported diagnoses and medication. Furthermore, in contrast to several previous studies with follow-up into old age,6,8,11,14 both genders were represented.
Traceability
A key limitation was that, despite considerable effort, we were only able to trace 14.4% of the HUSK participants to their birth records. There are several reasons for this: in particular, not everyone who participated in HUSK was born in the Bergen area, and others were born at home or at other hospitals. Two issues of generalisability can be considered here – the first is whether the analysed sample represented people present in the birth register; the second is whether the analysed sample represented people of their age group in the source population.
Considering the second issue, the 480 participants were broadly representative of the HUSK sample, the only substantial differences from the remainder being that they had higher educational attainment, higher values for waist and hip circumference, were more likely to be taking antihypertensive agents and more likely to have a higher metabolic score. The anthropometric and physiological differences suggest a higher vascular risk status in the analysed sample; however, other important indices such as resting blood pressure, total cholesterol levels, previous CVD and diabetes prevalence did not differ significantly or substantially between the groups, and HDL cholesterol was higher rather than lower. Furthermore, the HUSK sample itself has been shown to be representative of its sampled population. It is therefore unlikely that the presence or not of birth record information will have accounted for the observed findings.
Selection effects
It is important to bear in mind that most survival influences will have affected comparison groups equally in the analysed sample, because all people in the analysed sample were participants in the old age cohort of HUSK and all had there survived to those ages. However, selection effects need some consideration. Intrauterine and early influences which potentially increase the likelihood of adult diseases are likely to have influenced mortality in the time between exposure and outcome ascertainment. 23 Therefore, the same exposures that possibly increase risk of late-life outcomes may also have exerted some selection on the sample through increased mortality. In general, this would lead to positive selection of healthier survivors. 23 In order to detect any effects of early influences on the CVD health in old age, the negative effects of the early influences would have to be ‘sufficiently strong among the survivors to overwhelm the positive effect of selection’.23(p.165) As the temporal distance between exposure and outcome increases, these survival effects are likely to lead to progressively weaker associations of interest due to increasing positive selection, thus diluting potential exposure-outcome associations towards the null-hypothesis. This dilution could explain our null-findings, without necessarily invalidating the FOAD hypothesis for shorter follow-up periods. Of note, Koupilová et al. 11 found stronger associations between lower birthweight and hypertension at age 50 than at age 70, lending some support to this assertion. These potential dilution effects would have been interesting to explore in more detail, but this was not possible within the restriction of the present study (only two time points and a relatively small sample size). Selection effects may therefore have biased the findings through a healthy survivor effect previously described in occupational epidemiology. 24 Therefore, as well as the sample overall being healthier in earlier adult life than the general population, those with (for instance) a lower birthweight and increased risk for CVD may be less likely to have survived than those without these factors in combination.
Also, our analysis is based on participants in a population-based health survey. As health survey participants generally are more healthy than non-participants, 25 this might also have contributed to a selected healthier population than other studies investigating the FOAD hypothesis. It is, however, unlikely that such selection effects would obliterate all of the exposure-outcome associations, especially since CVD and diabetes was present in 12.8% and 6.6% (compared to 10.5% and 6.8% among the rest of the HUSK participants) of the sample, respectively.
Bias due to measurement error
Bias due to measurement error might have obscured the associations investigated. While a differential measurement bias is unlikely, as reporting in HUSK was unlikely to be influenced by birth circumstances, a non-differential bias might have biased the findings towards the null-hypothesis.26–28 However, we feel that measurement error is unlikely to be so substantial as to invalidate our findings entirely. Some of the outcomes are especially vulnerable to measurement bias, such as measurement of non-fasting glucose, and reliance on self-reported diabetes, CVD and medication. Also, information on maternal health and family circumstances were relatively crude in the birth records, and therefore more prone to error.
In conclusion, despite potential methodological challenges, the findings presented here suggest that the hypothesised associations between early life factors and later CVD outcomes do not appear to be substantial in later life. Specifically, the fact that we were not able to detect many associations in a relatively well-characterised sample suggests that the underlying effects are small and, in this elderly population at least, unlikely to be of major clinical or public health importance.29,30 The most likely explanation we feel is that associations between early life factors and later CVD outcomes in adulthood diminish in older age groups due to differential survival or dilution of effects through the emergence of competing risk factors. Our findings require confirmation in larger samples with higher tracing rates, and future research may benefit from focusing on other measures of early life factors, and where possible, also adopting a life-course perspective, rather than merely investigating gestation and birth.