
Abstract
Current challenges to sustaining public support for health data research have directed attention to the governance of data-intensive health research networks. Accountability is hailed as an important element of trustworthy governance frameworks for data-intensive health research networks. Yet the extent to which adequate accountability regimes in data-intensive health research networks are currently realized is questionable. Current governance of data-intensive health research networks is dominated by the limitations of a drawing board approach. As a way forward, we propose a stronger focus on accountability as learning to achieve accountable governance. As an important step in that direction, we provide two pathways: (1) developing an integrated structure for decision-making and (2) establishing a dialogue in ongoing deliberative processes. Suitable places for learning accountability to thrive are dedicated governing bodies as well as specialized committees, panels or boards which bear and guide the development of governance in data-intensive health research networks. A continuous accountability process which comprises learning and interaction accommodates the diversity of expectations, responsibilities and tasks in data-intensive health research networks to achieve responsible and effective governance.
Introduction
Contemporary health research is increasingly carried out on a large scale and in international networks. This is especially evident in the context of data-intensive health research. To unlock the potential of Big Data analytics, partnerships and networks comprising scientific communities, patient organizations and professionals across different disciplines are built (Anker et al., 2017). For instance, the BigData@Heart project, part of the Innovative Medicines Initiative's (IMI) Big Data for Better Outcomes (BD4BO) programme, seeks access to most of the relevant large-scale European databases to develop Big Data-driven, translational research platforms (Hemingway et al., 2018). We refer to such sets of autonomous yet interdependent actors which collaborate in health data research as data-intensive health research networks (DHRNs).
Along with the establishment of DHRNs, organizing sustainable and trustworthy practices to collect, share, link and use data has proven challenging (Kaye and Hawkins, 2014; Muller et al., 2022). As a result, the governance of DHRNs has become a salient topic of interest (Floridi et al., 2019; Sethi and Laurie, 2013). Governance concerns the organization of interaction and decision-making processes as well as responsibilities and tasks to facilitate appropriate conduct, oversight and collaboration in DHRNs (Ballantyne and Stewart, 2019; Deverka et al., 2017; Xafis et al., 2019). Moreover, governance is important to ensure public support and cooperation, building the trustworthiness required to maintain the social licence of data-intensive health research (Carter et al., 2015; Muller et al., 2021).
Demands have been raised recognizing that accountability is a crucial element for the ability of DHRN governance to function in a transparent way and merit trust in health data research (Blasimme et al., 2018; O’Doherty et al., 2011; Teare et al., 2018; Vayena and Gasser, 2016). However, developing suitable regimes for effective accountability has proven challenging. Current accountability practices are too incomprehensive and have insufficient capacity to impose measures to properly address urgent issues such as data misuse, rule violation and mismanagement (Blasimme et al., 2018; Kaye, 2011; McGuire et al., 2019). Moreover, accountability incorporates public interests, broader social priorities and justifications for the division of risks and benefits to only a limited extent (O’Doherty et al., 2011).
Whereas these are important accountability problems in DHRNs, more fundamental difficulties for developing effective accountability regimes need to be considered. If actors are to achieve coherence and agreement on accountability, shared norms, responsibilities and expectations are far from self-evident. Yet guiding frameworks are just beginning to emerge. Several principles and norms for governing health data research have been fostered. However, a lack of harmonization and widespread confusion about their meaning prevails (Kalkman, et al., 2019a; Phillips and Knoppers, 2016). This can be witnessed in the many open-ended and ambiguous conditions guiding local research sites and databases that participate in DHRNs informing governance (Kaye et al., 2018). Additional guidance by international data-sharing policies is warranted concerning such ‘white spots’ (Kalkman et al., 2019b). However, the uptake of existing guidelines and frameworks to guide long-term storage and future data use is scant (Knoppers, 2014; Mascalzoni et al., 2015). Lastly, patient and public values are barely incorporated to articulate principles and norms guiding governance (Deverka et al., 2017; Kalkman et al., 2019c; McGuire et al., 2019; Muller et al., 2022).
The challenges observed highlight a lacuna regarding the purpose and potential of accountability, which prevails in the literature addressing the governance of DHRNs as well as in policy-making and governance. We provide a critical analysis of the current state of affairs regarding governance and accountability in DHRNs and outline an approach which can help further develop accountability and effective governance in the context of DHRNs.
Current DHRN governance
Governing complexity
We can understand governance broadly as ‘the processes and structures of public policy decision-making and management that engage people constructively across the boundaries of public agencies, levels of government and/or the public, private and civic spheres in order to carry out a public purpose that could not otherwise be accomplished’ (Emerson et al., 2012: 2). With this definition as a starting point, we reviewed the literature to shed light onto how governance in DHRNs is shaped.
The governance of data-intensive health research concerns the organization of conduct, oversight and collaboration in data-intensive health research. DHRNs cover a broad array of health data, ranging from electronic health records to aggregated clinical trial data (Erikainen et al., 2021; Mostert et al., 2016). Governance structures are built around sharing and linking data, resulting in new collaborations and combinations of data for the purpose of particular research endeavours, such as cardiovascular disease in the BigData@Heart consortium. Thereby, governance compiles and aggregates pre-existing approaches to governing health data research of collaborating parties, such as those employed by pharmaceutical companies, hospitals and professional organizations (Kalkman et al., 2019b). Moreover, new organizational forms are created to link and access data, such as multi-layered platforms and federated systems, which arise from the practical need to facilitate a variety of data-driven research types (Floridi et al., 2019; Mandl et al., 2020; Murtagh et al., 2012).
Current DHRN governance interweaves vested ethics oversight and review mechanisms with an approach driven by regulatory and policy requirements for research conduct, data handling and cooperation (Morrison et al., 2020). This ethico-legal approach balances the protection of patients from the possible harms of participating in research with the public benefits of health research (Laurie, 2017; Sethi and Laurie, 2013). This approach operates by streamlining the handling of conditions for informed consent, addressing the return of results and processes for ethics and data-sharing clearance by research ethics committees (RECs) and data access committees (DACs). Moreover, the ethico-legal approach entails formulating soft law and normative guidance concerning research conduct and procedures for data handling (Kaye et al., 2018; Kaye and Hawkins, 2014).
Regulation has a prominent role in enforcing governance mechanisms by formally demanding legal bases for processing data and requiring safeguards for responsible data handling. Regulation architectures (Evans, 2016; Mostert et al., 2016; Rothstein, 2013), technical requirements (Scheibner et al., 2020) and data protection rules are explicated in legislation such as the European Union's General Data Protection Regulation (GDPR) of 2016 and the Health Insurance Portability and Accountability Act (HIPAA, last amended in 2013) in the United States (Rothstein, 2013). Moreover, soft law and guidelines can be found at the international level (Knoppers et al., 2011; Sethi and Laurie, 2013). Examples are the World Medical Association's Declaration of Taipei (2016), guideline 12 of the Council for International Organizations of Medical Sciences’ International Ethical Guidelines for Health-related Research Involving Humans (2016), and the Global Alliance for Genomics and Health's Framework for Responsible Sharing of Genomic and Health-Related Data (2014) (Ballantyne, 2019; Scheibner et al., 2020). Still more dedicated sets of stipulations and rules are produced in response to ongoing debates about large-scale data research (Carter et al., 2015; Kalkman et al., 2019a; Scheibner et al., 2020).
Adding to the above, self-regulation such as via codes of conduct has become an accepted means for DHRNs to establish best practices fit for the purpose of governance (Floridi et al., 2019; Knoppers et al., 2011). Finally, DHRNs often comprise an array of arrangements and entities that delineate and govern the functioning of ethical review and oversight of data processes in practice, going beyond strict formal requirements (Kaye et al., 2015, 2018; Laurie et al., 2015; Sethi and Laurie, 2013). Examples are governance advisory committees as well as specialized advisory boards or panels. These are mostly issue-specific, tasked with addressing topics such as confidentiality, public benefit, involvement and engagement that arise in governing collaborative health data research (McHale, 2011; O’Doherty et al., 2021).
Problems of current DHRN governance
The governance of DHRNs crystallizes in the form of various norms, institutions and practices. As a result, governance infrastructures are subject to many normative outlooks as well as different interests and perspectives. Across distinct DHRNs, these specific ‘constellations’ impact how governance is articulated. Therefore, specific articulations of governance may vary to a great extent, depending on contextual circumstances. What is more, the resulting complex variety puts a burden on existing capacities to effectively address pertinent overarching governance challenges. At the same time, the success of addressing these challenges depends on the ability to engage in concerted governance efforts, whereas collaboration in governance cannot be simply presumed: it needs to be facilitated. The complexity of factors affecting DHRN governance may obscure that attempts to further coherent and tailor-made governance are complicated (Kaye et al., 2018; Muller et al., 2021).
Attempts to further the development of DHRN governance focus on anticipating and pre-empting complexities that are induced by the variety of norms, institutions and practices described. Yet due to these complexities, the capacities to further DHRN governance in such a quick and dirty manner are insufficient. Therefore, DHRN governance all too often degenerates into a top-down approach to governance (Dove et al., 2016; Dove and Özdemir, 2015). Top-down governance upholds a preoccupation with advance harmonization, focusing on solving practicalities that arise from conducting data sharing, linking and research piecemeal (Kalkman et al., 2019a). As a result, governance practices only fulfil regulatory requirements and criteria for appropriate ethical oversight and review of data access in a limited, minimalist way (Dove et al., 2016; Shabani et al., 2017). However, the structural challenges of developing governance to shape responsible collaborative data research institutions and practices remain under-addressed (Kaye et al., 2015, 2018).
Top-down governance is initiated for the main purpose of constructing the entity of the consortium, rather than enabling the collaborative network structure that underlies it (Dove et al., 2016; Dove and Özdemir, 2015). This comes down to drawing board governance, which can be clearly recognized when looking at the focus on facilitative activities. Principal purpose is to gather, inventory and categorize conditions for data sharing, contained in ethico-legal documents specified beforehand for individual participating datasets and databases (Kalkman et al., 2019b). This often results in mere aggregation of conditions, principles and norms. However, subsequent effort to facilitate convergence, such as by harmonizing agreements and policies, is lacking (Kalkman et al., 2019a; Phillips and Knoppers, 2016). Similarly, in-context operationalization of conditions to guide collaborative practice requires further and far-going effort.
As stated, the governance of large-scale health data research usually materializes within specific research projects organized in the form of consortia. Drawing board governance is therefore often undertaken in new research endeavours. Yet when these evolve into DHRNs of their own, governance which goes beyond their formative consortia is required. Therefore, governance able to sustain collaborative health data research in networks becomes necessary (Kaye and Hawkins, 2014; Mayrhofer and Prainsack, 2009; McGuire et al., 2019). Thus, DHRN governance concerns an enterprise which should go beyond the minimum requirements of a consortium.
For the greater part, parties participating in DHRNs have thus far been reluctant to devote significant amounts of time, attention and resources to establish frameworks that could guide the governance of collaborative health data research. For DHRNs to flourish, existing principles and norms require translation to clear structures and tangible policies that establish a distinct governance system (Blasimme et al., 2018; Global Alliance for Genomics and Health (GA4GH), 2014; Kalkman et al., 2019a). For now, it remains unclear how expectations, responsibilities and tasks can be comprehensively addressed (Blasimme et al., 2018; Kaye, 2011; McGuire et al., 2019). Moreover, to steer DHRNs and make sure that they deliver on their promises, effective accountability needs to be developed as a part of governance (Aitken et al., 2016a; Dove et al., 2016; Laurie and Sethi, 2013; Morrison et al., 2020).
Accountable network governance
In the literature on DHRN governance, accountability is often classified as a norm or principle which is part of the pursuit of public trust and engagement in the governance of DHRNs (Aitken et al., 2016a; Carter et al., 2015; Dove and Özdemir, 2015). As such, accountability has a strong connection with the norms of transparency, integrity, responsibility and solidarity (Blasimme et al., 2018; Kalkman et al., 2019a; Kaye, 2011). However, this interrelatedness makes accountability hard to discern as a stand-alone element of governance.
For realizing accountable governance, we are required to approach accountability not solely as an abstract norm or principle inherent to DHRN governance. Rather, public administration theory has conceptualized accountability as a process of account-giving and account-holding: ‘a relationship between an actor and a forum, in which the actor has an obligation to explain and to justify his or her conduct, the forum can pose questions and pass judgement, and the actor may face consequences’ (Bovens, 2007: 450). The process of accountability is characterized by information provision, debate and the possibility of facing and imposing consequences (Bovens, 2007; Bovens et al., 2008). For that reason, accountability mechanisms are central for ensuring democratic control and safeguarding the legitimacy of governance. In addition, accountability maintains abilities to steer and adapt the functioning of governance (Bovens, 2007; Dubnick and Frederickson, 2011; Skelcher, 2005). To fulfil these functions, parties collaborating in DHRNs need a regime within which accountability can operate. An accountability regime consists of tangible relationships and mechanisms, establishes expectations to explain and justify conduct, and enables parties to raise questions, pass judgement and ultimately face consequences (Bovens, 2007; Bovens et al., 2008; Scott, 2000).
Considering processes, let alone regimes of accountability has thus far played a minor role in health data research governance. Valid reasons can be given for this underappreciation: the conceptualization of the accountability process primarily applies in hierarchical state-oriented governance, in which public organizations interact in principal–agent relationships (Bovens et al., 2008; Strøm, 2000; Willems and Van Dooren, 2012). Consequently, accountability is approached as formal answerability and mainly performs external and retrospective scrutiny (Acar et al., 2008; Willems and Van Dooren, 2012). It functions by virtue of relative certainty and a degree of mutuality between principal and agent, which rests on the assumption that both sides of the relationship are embedded in an encompassing governance system (Bovens et al., 2008). In sum, accountability presupposes straightforward and stable relationships between parties carrying out tasks (the actor or agent) and the groups to whom they should be responsive (the forum or principal) (Bovens et al., 2008; Willems and Van Dooren, 2012).
These conditions ensure that a shared structure of norms, responsibilities and expectations exists, enabling accountability to fulfil its functions (Acar et al., 2008; Bovens, 2007; Philp, 2009). The governance context of networks such as DHRNs limits the extent to which these conditions can be fulfilled. More fundamentally, governance of networks disputes how accountability's purpose, purview, terrains of inquiry and processes should take shape.
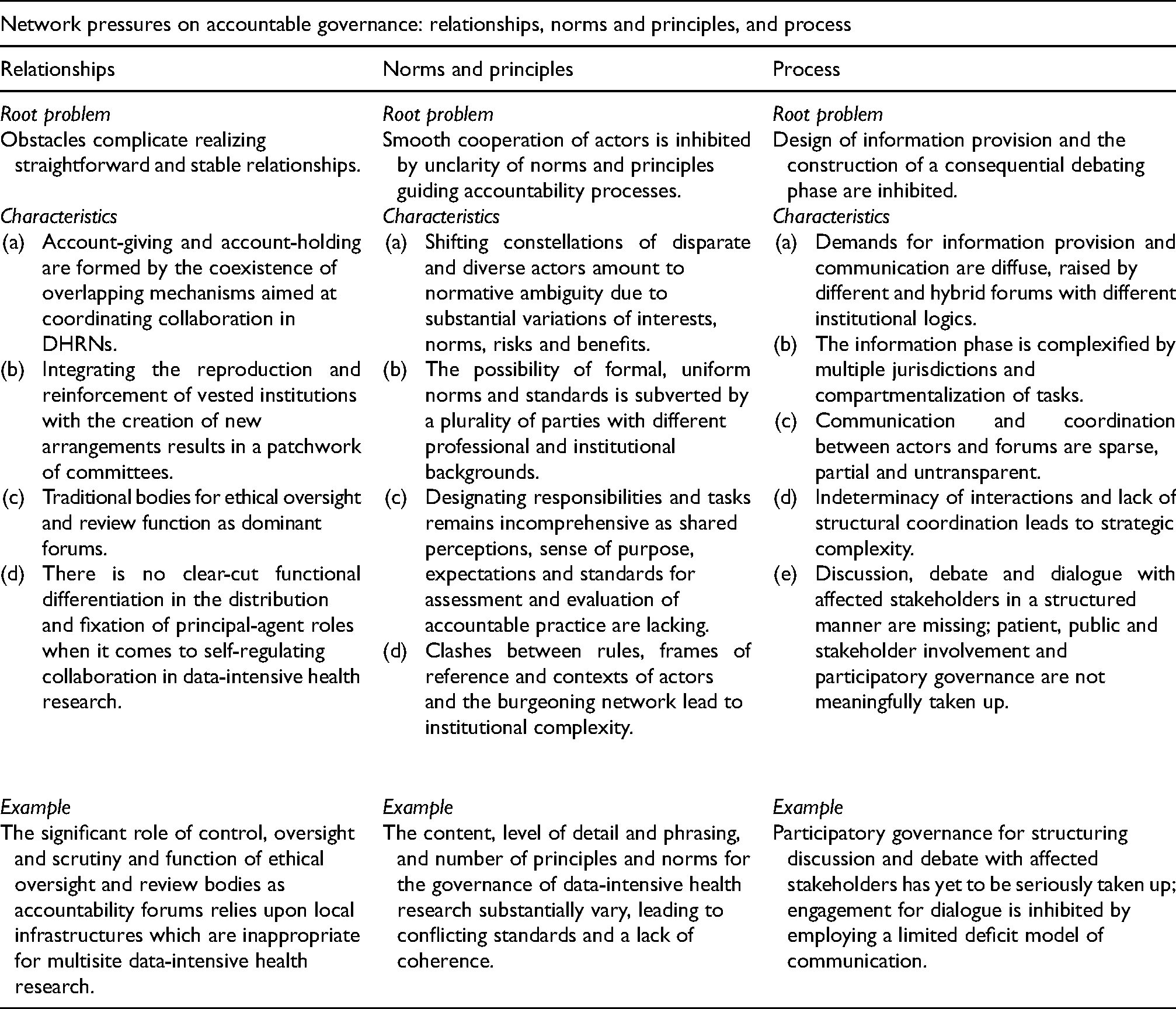
Network pressures on accountable governance
Governing DHRNs is marked by interdependent partnership and horizontal collaboration. This development has displaced and fragmented traditional hierarchical governance (Frederickson, 1999; Skelcher, 2005). As a consequence, it seems dubious to assume the same level of coherence among parties which could result in an overlapping consensus about an accountability regime (Bovens et al., 2008; Willems and Van Dooren, 2012). This lack of convergence creates ambiguity in collaborating parties’ perceptions of their governance relationships. Interpretations are more likely to differ and generic standards for accountability processes cannot be presumed. On the whole, this impedes effective accountability in governance (Acar et al., 2008; Bovens et al., 2008; Willems and Van Dooren, 2012). We subdivide and characterize this accountability problem further according to three pressures arising in DHRN governance.
First, realizing straightforward and stable relationships in accountable governance is complicated (Bovens et al., 2008). Multiple mechanisms for coordinating collaborative health data research coexist and overlap in DHRNs (Kaye, 2011). The accountability relationships that result form a rather heterogeneous ensemble. DHRN accountability relationships incorporate firmly established ethical oversight and review legacies, while concern exists for novel topics particular to the large-scale and collaborative nature of data collection, sharing, linkage and research (Kaye, 2011). This dynamic leads to pressures to integrate traditional and innovative checks and balances on health data usage. As a result, existing oversight and review bodies are reproduced and amended while new advisory committees, boards and panels are formed (Dove et al., 2016; Laurie and Sethi, 2013; Shabani et al., 2017). This makes identifying and establishing clear-cut accountability relationships challenging. Accountability in the form of ethical oversight and review has become the task of a patchwork of committees. At present, they play a significant role as principal in the accountability relationship. However, their capacities are tied to research ethics infrastructures that are mostly situated at the level of local research sites. This makes it difficult to take the specific characteristics and issues of multisite health data usage into account and consider its impact at the appropriate level (Cheah and Piasecki, 2020; Kaye, 2011; Shabani et al., 2017). Additionally, while formally independent, RECs and DACs are either subsidiaries of participating research institutions or bound to specific projects (Erlich et al., 2014; McHale, 2011; Shabani et al., 2017). Their coexistence creates overlap in scrutiny, oversight, review and control tasks, fostering replicate review problems overburdening RECs (Dove et al., 2016). Employing DACs for downstream data use has introduced redundancies in scope between the two (Cheah and Piasecki, 2020; Kaye and Hawkins, 2014). To clarify the current disorientation in this system, determining a desirable and appropriate division of tasks is warranted. Moreover, it requires enhancing communication channels to align review practices between RECs and DACs (Dove et al., 2016; Erikainen et al., 2021; Shabani et al., 2017). Another example highlights that the roles of principal and agent are only to a limited extent fixed to specific sets of parties in DHRNs. Data protection law such as the GDPR creates a fundamental distinction between data controllers who determine the aim, scope and means of data use, and data processors who have to abide by binding data transfer agreements (Kalkman et al., 2019b; Mostert et al., 2016). Yet for large-scale health data research, this distinction's legitimacy and suitability are contested, since the ensuing rules, responsibilities and requirements among both sides remain uncertain (Forgó et al., 2021; Hallinan, 2021; Marelli et al., 2021). In addition, horizontal forms of collaboration mean that only minor difference exists between principal and agent roles. Such role obfuscation can be seen in the exercise of self-regulation and the establishment of best practices to review public value and uphold scientific integrity (Mayrhofer and Prainsack, 2009). When asserting many health data usage topics, fixed distinctions are surpassed, which muddles parties’ principal-agent responsibilities and tasks relating to governance (Mayrhofer and Prainsack, 2009; Sethi and Laurie, 2013).
Second, unclarity about guiding norms and principles for the accountability regime and the use of different sets of guidance inhibits smooth cooperation between parties (Acar et al., 2008; Bovens, 2007; Philp, 2009). DHRNs are premised on diverse and shifting constellations of actors (Cole et al., 2016; Hemingway et al., 2018), which makes accommodating ambiguity in sensemaking and interpretation difficult. Accommodation is pivotal to achieve overlapping consensus on perceptions and expectations about goal setting and priority-setting for data usage as well as about standards for evaluating accountability (Laurie and Sethi, 2013). In consequence, comprehensively designating corresponding responsibilities and tasks becomes an increasing challenge when collaboratively sharing and using health data (Blasimme et al., 2018; Kaye, 2011; McGuire et al., 2019). Ambiguity also stems from the involvement of private parties in DHRNs as well as the rise of the international context of data usage (Ballantyne and Stewart, 2019; Kaye, 2011; Kaye et al., 2018; Vaudano, 2013). Substantial variations remain in interests, risks and benefits that parties on either side of the ‘public-private divide’ are willing to accept (Ballantyne and Stewart, 2019; Sethi and Laurie, 2013; Xafis et al., 2019). Similarly, concerns about public trust in private-sector cooperation endure (Aitken et al., 2016b; Marelli et al., 2021). Therefore, unclarities in interpreting regulatory conditions and requirements for health data sharing require reconciliation (Floridi et al., 2019; Winter and Davidson, 2018). In sum, the consortia formative of DHRNs consist of a plurality of parties with different professional and institutional backgrounds, which disturbs establishing uniform norms and standards for an accountability regime (Kaye et al., 2018). If successful, DHRNs face institutional complexity, since internal behaviour-regulating rules and procedures of parties clash with those governing the network (Blasimme et al., 2018; Klijn and Koppenjan, 2014). Systematic review of the content, level of detail and phrasing as well as number of principles and norms for the governance of data-intensive health research revealed substantial variation, conflicting standards and a lack of cohesion (Kalkman et al., 2019a).
Third, obstacles arise in arranging an accountable governance process, specifically finding suitable means of two-way communication and organizing meaningful debate (Strøm, 2000). The compartmentalization of tasks and interaction of multiple jurisdictions in DHRN complexifies providing appropriate information, a crucial part of the accountability process. Demands for information are coming from more parties and have become diffuse as a result (Floridi, 2013). Information provision forms a challenging task for DHRNs facing accountability in an ecosystem of actors (Vayena and Gasser, 2016). Sparse coordination and untransparent communication between collaborating parties and stakeholders aggravate this problem (Kaye et al., 2015; Kaye and Hawkins, 2014; O’Doherty et al., 2021). Moreover, greater structural coordination is needed to enable an effective collaborative response to anticipate regulatory and policy requirements and streamline communication practices (Kaye et al., 2015; Sethi and Laurie, 2013). Interactions between parties are too indeterminate to facilitate structural uptake, creating ‘strategic complexity’ (Klijn and Koppenjan, 2014). To channel external accountability demands, adjustment between DHRNs, regulatory bodies and funders is required (Kaye, 2011; Laurie, 2011; Morrison et al., 2020; Wahlberg et al., 2013). However, accountability demands from stakeholders, publics and society at large remain underarticulated in DHRN governance (Aitken et al., 2016a; Kaye et al., 2018; Vayena and Gasser, 2016). Participation in DACs and governance advisory bodies by patients and members of patient organizations is possible to a limited extent, whereas it provides opportunities for meaningful involvement on patients’ own terms (Blasimme et al., 2018; Cheah and Piasecki, 2020; O’Doherty et al., 2011; Winickoff et al., 2016). To entrench discussion and debate with affected stakeholder groups, greater consideration of structural co-production or participatory governance is required (Buyx et al., 2017; McGuire et al., 2019; O’Doherty et al., 2011, 2012). See Table 1 for an overview of the three network pressures on accountable governance in DHRNs.
Three network pressures on accountable governance in DHRNs.
Learning accountability
In DHRNs, realizing effective regimes for accountable governance forms a complex challenge which is difficult to address within the drawing board governance approach. We, therefore, draw further inspiration from public administration theory on accountability, where the design of accountability under complex governance circumstances has gained attention.
The pressures on establishing accountable governance that we identified in DHRNs have been recognized as characteristic of contemporary network governance beyond this case as well (Bovens, 2007; Skelcher, 2005). The recognizability of these pressures emphasizes that realizing regimes for accountability to function warrants far greater attention in the context of network governance. Therefore, developing an appropriate framework is required to guide the shaping of a comprehensive system for accountable governance. However, developing an appropriate framework necessitates revisiting the conceptualization of accountability.
Difficulties in realizing clear and coherent relationships, norms and principles, and processes of accountability in DHRNs indicate that we need to address how accountable governance can be accomplished. Accordingly, prior focus on meticulous explication of the appropriate what of accountability in health data research needs complementation. Given the pressures encountered in DHRN governance, preoccupation with solving substantive practicalities of health data usage as prime task of governance (Blasimme et al., 2018; Kaye, 2011) provides little guidance on how accountable health data usage can be realized. Asking how accountable governance can be facilitated allows reflection on the purpose and potential of accountability processes (Acar et al., 2008; Strøm, 2000; Willems and Van Dooren, 2012). Still, this too occurs against the backdrop of similar network complexities (Klijn and Koppenjan, 2014).
At the heart of addressing how accountable governance can be achieved lies the practical necessity to find ways forward serving the purpose to which regimes of accountability should be geared. Finding ways forward requires acting structurally upon tentative proposals to determine the most pertinent account-giving actors (or agents) and account-holding forums (or principals) in accountable governance processes. Moreover, specific terrains (Mulgan, 2003: 22) as well as topics of large-scale, collaborative health data usage need to be prioritized to sensitize accountability as a part of governance.
Public administration theory has formulated approaches which revisit the purpose of accountability and reconsider how to put this purpose to practice (Acar et al., 2008; Bovens, 2007; Willems and Van Dooren, 2012). The ideal of accountability goes beyond the processes and institutions that facilitate designated mechanisms and arrange relationships to give and hold to account (Bovens et al., 2008). This conception is in line with the normative connotation of being accountable as part of the pursuit of public trust and engagement (Aitken et al., 2016a; Carter et al., 2015; Dove and Özdemir, 2015). For that reason, accountability first and foremost consists of finding appropriate ways to exercise introspection and self-control. Such self-regulation is based upon norms, responsibilities and expectations that emanate from overlapping consensus achieved in collaborative organizational networks like DHRNs (Acar et al., 2008; Aucoin and Heintzman, 2000; Romzek and Dubnick, 1987; Willems and Van Dooren, 2012). Accountability mechanisms seek to invoke processes which stimulate organizations and actors to reflect upon practices, as a mode of learning how appropriate governance can be achieved. Consequently, accountability functions as an integral element of organizational and governance practices to facilitate continuous, integrated learning. This learning accountability supplements current approaches guiding DHRN governance by translating and applying abstract guidance in the form of principles and norms to situations in concrete governance contexts.
Accountability which revolves around stimulating learning provides a way of addressing the broader how question raised in the context of establishing accountable governance (Ebrahim, 2005). Enabling accountable governance forms a tool to induce those engaged in practices of implementing guidance, strategies and policies into conduct to learn from performance feedback (Aucoin and Heintzman, 2000; Bovens, 2007; Bovens et al., 2008). Being accountable thrives by institutionalizing capacities for recurrent learning about novel topics of concern arising along the governance process, which instigates actors to engage with each other in a constructive way (Argyris and Schön, 1978). This dynamic outlook relies on opening up rigid and closed organizational networks (Sabel and Zeitlin, 2012). Moreover, to enhance actors’ willingness to learn and proact on acquired insights, feedback-based inducements should be part of recommendations for practice (Acar et al., 2008; Romzek and Dubnick, 1987).
Clear-cut communication and reflective debate with account-holding forums and outside actors lie at the heart of learning by being accountable (Bovens et al., 2008). To embed learning, strategies for managing, adjudicating between and incorporating diverse expectations of governance parties and stakeholders are necessary (Acar et al., 2008; Willems and Van Dooren, 2012). To forestall the challenges of indeterminacy and complexity in governance, seeking overlapping consensus is required to provide guidance rooted in motives and expectations of collaborating parties. In sync exchange of information enables parties to enhance capabilities for retrospection on past practices. The accuracy, timeliness and clarity of information must be ensured to guarantee an effective discussion phase (Bovens et al., 2008). Flexible information systems allow actors to provide diagnoses about relevant dimensions of practices that are better attuned to the needs of accountability forums (Ebrahim, 2005). Flexibility and relevance facilitate interchanging information suited to specifically situated accountability demands, which contributes to the focus and timeliness of learning (Bovens et al., 2008).
Decision-making and priority-setting practices require ongoing, critical reflexive examination welcoming dialogue among parties (Argyris and Schön, 1978; Aucoin and Heintzman, 2000). Therefore, interaction routines should be designed to induce recurring dialogue among parties about feedback on practices as they develop (Acar et al., 2008; Bovens et al., 2008; Klijn and Koppenjan, 2014). Dialogue is needed to ‘determine responsibilities, authorize discretion, establish reporting procedures and create review processes for the relationship’ (Whitaker et al., 2004: 115). Moreover, dialogue needs to be consequential to yield effective, meaningful uptake and eventual change of conduct and governance practices. A strong yet constructive forum in which the most relevant and pertinent stakeholders and affected publics can participate could control this need.
Approaching accountability as learning contributes valuable theoretical insights to help provide guidance on how accountable governance can be realized. Governance parties should be enabled to learn together about how relationships, norms and principles, and processes of accountability can be shaped and improved in an ongoing fashion. Overlapping consensus about norms, responsibilities and expectations should be relied on to foster collaborative self-regulation and self-control. Stimulating the learning potential in accountability regimes furthers realizing responsible practices of collaborative health data usage.
Perspectives for accountable DHRN governance
We recommend two pathways to enable learning accountable governance in DHRNs and depict how these can be pursued in entities geared towards bearing or guiding governance in DHRNs. Committees, boards or panels involved in governance are appropriate places for bundling learning processes. Many such entities are already part and parcel of DHRN governance structures. We refer to them simply as governing bodies. Additionally, learning processes can be integrated into substantive committees and panels dedicated to specific topics. Citizens’ or community advisory panels or boards serve as good examples (Deverka et al., 2019; McGuire et al., 2019; O’Doherty et al., 2021), but boards advising on topics such as ethics, data access, oversight, confidentiality as well as panels representing interests and perspectives of affected groups, or established RECs and DACs may fulfil a similar role. By strengthening their learning potential, governing bodies can be utilized to shape accountable governance, guiding and bearing governance processes in DHRNs. Embedding learning relies on framework rule-making as well as continuous revision, which is enabled by recursively reviewing experiences with implementing governance processes in specific contexts. This approach has been referred to as ‘experimentalist governance’ (Sabel and Zeitlin, 2012).
Implementing accountability requires adapting learning processes and mechanisms to accommodate contextual circumstances and specific conditions, such as the (inter)national setting, cross-sectoral nature and mix of public/private organizations that impact the makeup of wider governance structures (Kaye et al., 2015; O’Doherty et al., 2011; Sethi and Laurie, 2013). Realizing accountable governance by learning depends on an eclectic mix of characteristics and factors for which no uniform blueprint can be provided. Instead, we propose two pathways to develop learning accountability processes in governing bodies.
The first pathway addresses the structural side of implementing learning accountability. This dimension focuses on developing an integrated structure (Sabel and Zeitlin, 2012), or rather a ‘backbone’ for learning to occur. An integrated structure embeds insights from learning activities and realizes its impacts on how collaborative health data usage in DHRNs ought to be governed. To that end, governing bodies require greater integration with operational management and steering of the governance activities they are devoted to. As a first step, governance bodies should be given a greater role in providing independent advice and recommendations. Moreover, authority must be handed over to enable governing bodies to raise requirements for meaningful response and preferably uptake. Response or uptake can be either changes in practice, policy or follow-up discussion about the issues raised by the governance body. Practical ramifications of this change, such as devoting resources, required time commitment, appropriate recompense and minimum expertise demand consideration, especially regarding the participation of ‘lay’ committee members. This raises questions about the desired levels of professionalizing governing bodies and their membership. Considering these issues is crucial for enabling and empowering effective governing bodies and should be an integral part of their design.
An integrated structure systematically intertwines parties and involves and engages with affected stakeholders, communities and publics of health data research as partners. Fostering interaction between widely different partners of health data ecosystems (Vayena and Gasser, 2016) is pertinent to enable collaborative learning activities across the network. At this level of abstraction, only broad guidance can be provided for determining which actors are pertinent to participation. Participation should in principle be open to allow data providers, patients, publics, communities and stakeholders at large which are affected most to be included. Depending on context, scope and scale, representation such as by patient organizations should be considered as a viable option.
To provide more specific input on who to involve regarding which questions, governing bodies should actively build on and translate international efforts that develop guidance and consensus on responsible governance (e.g., Global Alliance for Genomics and Health (GA4GH), 2014, 2016, 2021; Knoppers, 2014; Knoppers et al., 2011; Rehm et al., 2021). Drawing on contextual considerations for incorporating and applying international guidance on involvement raises the potential of triggering reflexive learning processes. As a starting point, international guidance provides an initial architecture for conveying experiences and perspectives instrumental to acquiring meaningful insights. At the same time, governing bodies should retain their abilities to develop actionable initiatives at their own discretion (cf. Emerson et al., 2012).
To facilitate the evaluation of conduct and governance practices, provisional long-term goals need to be articulated. Establishing such goals according to overlapping consensus is crucial to develop mutual understanding, shared motivation and common commitment (Ebrahim, 2005; Sabel and Zeitlin, 2012). Aspiring to reach overlapping consensus requires due regard for the underlying assumption that parties are reasonably willing to weigh each other's considered convictions regarding the collaboration and its goals (Taebi, 2017). Governing bodies should therefore consider it their prime task to establish continuous development and revision of a framework of coherent principles and norms (Sabel and Zeitlin, 2012). Ongoing application and reconsideration of principles and norms that can guide both practices of large-scale collaborative data collection, sharing, linkage and research, as well as their governance, lies at the heart of governing DHRNs. For example, this concerns negotiating how health data usage across sectoral and private/public boundaries can be streamlined (Kaye and Hawkins, 2014; Mascalzoni et al., 2015; Morrison et al., 2020). To this end, international guidance needs to be incorporated and translated in situated DHRNs as well, to ensure the continuity of governance according to acclaimed best practices. Interconnection can prove helpful in providing foundational principles and core elements and topics to build upon, especially when coherence between parties is lacking and diversity of norms and principles is significant (Global Alliance for Genomics and Health (GA4GH), 2014; Knoppers, 2014). Contextual factors, situated lived experiences and reflexive interpretations should steer how abstract guidance is dealt with and translated to meaningful governance practice.
Learning relies on engaging in network management of the relationships between partners (Klijn and Koppenjan, 2014). Relationship building can facilitate elaborating on interaction and collaboration processes between partners by cultivating informal working relationships based on mutual trust (Emerson et al., 2012). By this, we mean both cross-sectoral interactions between professionals and researchers, but also more dynamic interactions with data providers, patients, publics, communities and stakeholders at large (Ballantyne and Stewart, 2019; McGuire et al., 2019; Xafis et al., 2019). Relationships and characteristics like trust and respect between parties involved need to be mapped. Existing interaction processes need to be built upon, developed and refined for network management to succeed. This stresses the importance of aligning the plurality of motivations prevalent in multi-partnerships. Joint goal setting by regularly consulting with pertinent stakeholders forms a recursive process which is crucial to control learning processes in governing bodies (Emerson et al., 2012). Therefore, joint goal setting should enable reviewing and reflecting on the transparency of day-to-day governance mechanisms. Joint goal setting strengthens subsequent capabilities for collaborative action (Teare et al., 2018). Principled collaborative engagement (Emerson et al., 2012) enhances partners’ abilities to understand each other's positions and interests in developing and refining topics requiring consideration for accountable governance. Mutual recognition of efforts and contributions that embolden collaboration forms an indispensable part of constructive engagement. Strengthening the partnership of collaborating parties encourages building capacity for joint action (Emerson et al., 2012). Additionally, constructive engagement draws on an open vocabulary to promote an accessible discourse for addressing topics and issues which arise in the accountability process. Accessible discourse fosters a greater esprit de corps, which is helpful to instil a greater sense of co-ownership of the network.
Governing bodies need to settle upon mutually agreeable decision-making and policy-making practices. Procedural requirements should entrench lay participation as well as formally embed public consultation and feedback on decision-making and policy-making (Ebrahim, 2005). Participation ensures that stakeholders pertinent to acquiring valuable insights into issues under examination are enabled to interact and express their lived experiences (Sabel and Zeitlin, 2012). Thus, they are given greater power to influence how decisions regarding health data usage, governance practices as well as guiding principles, codes of conduct and working arrangements are made. Therefore, overcoming existing hierarchies of power embedded in DHRNs remains necessary. This requires bold, but granular and realistic measures. Safeguarding that decision-making and policy-making procedures remain transparent and inclusive is a first step in thwarting hierarchies to enhance the impact of learning on accountable governance.
The second pathway establishes reflexive dialogue by stimulating ongoing deliberative processes and specifying how collaborative communicative practices can be realized (Emerson et al., 2012). One-way explanation and information provision requires replacement to overcome the opaque nature of interaction regarding collaborative health data usage and governance. Multiple opportunities should be pursued to open up communication practices and integrate meaningful interaction with partners. Engaging in diverse types of two-way information provision explicitly raises accessibility and lowers the threshold for participation. Communication needs to be catered to a plurality of partners: patients, publics, communities and stakeholders at large. Open and understandable communication is crucial to receive experience-driven feedback and attain insights from partners’ perspectives that can stimulate learning about the appropriateness of governance (Lerner and Tetlock, 1999). Accessibility for parties that are distant to day-to-day governance practices is especially important. Staying attuned and open to bottom-up demands significantly depends on explicit consideration of information demands from marginalized communities. Moreover, two-way communication means increasing flexibility to tailor information to those aspects of conduct and governance practices that are considered integral to independent scrutiny and evaluation by ‘lay’ account-holding forums (Ebrahim, 2005). To benefit from concrete lived experiences and insights of ‘lay’ experience experts, their abilities to express their perspectives on topics as and how they see fit must be empowered (Sabel and Zeitlin, 2012).
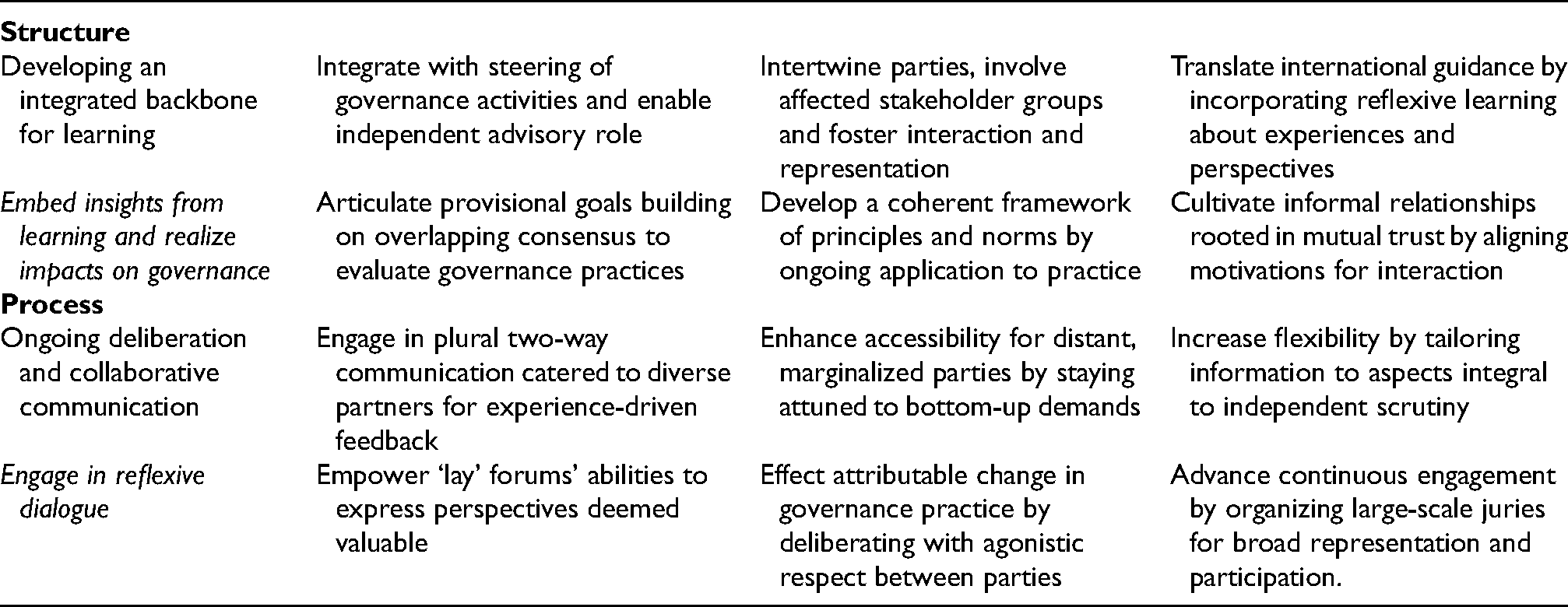
Reflexive dialogue and broadening the utility of communicative practices should have tangible consequences. Communication and collaborative interaction should lead to an attributable change in governance practices. In order to become more meaningful and effective, reflexive dialogue can take the form of reflective discussion or more active debate. Yet as opposed to antagonistic or adversarial interaction, deliberation should be characterized by agonistic respect between parties (Davies, 2007; Sørensen and Torfing, 2005). Moreover, continuous efforts to engage relevant partners are self-evidently required for actual co-creation to take hold (Emerson et al., 2012). To advance continuous engagement, affected groups of publics, communities and stakeholders at large should be organized and established collectively as an account-holding forum. Various forms are permissible, such as user, data provider and patient panels. However, organizing large-scale citizens’ juries is preferable due to their larger size and greater ability to include relatively diverse perspectives, interests and experiences. Embedding affected groups within governance bodies allows seeing them as genuine, extended accountability forums, which organize broad representation and participation. Realizing collective organization within governing bodies fosters a more open, (self-)critical atmosphere in the DHRNs as a whole. Moreover, strengthening the ability to raise accountability demands from the bottom up is conducive to examining, evaluating and learning from the feedback regarding governance practices among different parties. See Table 2 for an overview of the key points for learning accountability in DHRN governing bodies for each pathway.
Key points for learning accountability in DHRN governing bodies.
Conclusion
Accountable governance of conduct, oversight and collaboration in DHRNs forms an important means of ensuring public support and cooperation with data-intensive health research. Difficulties in realizing accountability present a profound conundrum both in the literature and in the policy-making and governance of DHRNs. Having reviewed and analysed the complex networks that have become commonplace in the field of data-intensive health research, developing learning accountable governance serves to complement and further achieving more adequate, comprehensive and inclusive accountability. Whereas learning accountable governance cannot be established overnight, following the pathways of developing an integrated structure for learning to occur and establishing a reflexive dialogue in the form of an ongoing deliberative process in dedicated governing bodies provide important steps towards the accountable governance of large-scale and collaborative data collection, sharing, linkage and research in DHRNs.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was part of Work Package 7 of the BigData@Heart consortium, which received funding from the Innovative Medicines Initiative 2 Joint Undertaking (IMI2) under Grant Agreement No. [116074]. This Joint Undertaking receives support from the European Horizon 2020 research and innovation programme and the European Federation of Pharmaceutical Industries and Associations (EFPIA). IMI did not have any role in the formulation of the research aims, decision to publish or preparation of the manuscript.