
Abstract
Current theoretical models intended to guide health services research and evaluation lack care coordination-its features and impacts. These aspects are critical for understanding the role of care coordination in healthcare use, quality, and outcomes. In this Focus article, we briefly review the well-known Andersen individual behavioral model (IBM) of healthcare use and the Donabedian health system and quality model (HSQM) together with recent practice-based evidence. We propose a new integrated theoretical model of healthcare and care coordination. The model can serve as a guide for future research to better understand the variation in care coordination services and delivery and its added value to improving mental health in different real-world settings.
Introduction
The pandemic has brought stark attention to rising mental distress and the challenges that many people face accessing and navigating healthcare. Care models employed to support people with mental health conditions have proven valuable in addressing a wide range of needs among adults and children, including access to combined therapies, issues with employment and housing, and management of co-occurrence of addiction and other conditions.1,2 Yet while care models have evolved to measure aspects of care coordination, our current theoretical models have not changed. The lack of a theoretical model that incorporates evidence from practice makes it challenging to design new studies of care coordination in a variety of settings. A new theoretical model is needed that will guide future evaluation and research about the role of care coordination and its influences on healthcare utilization, quality, and mental health outcomes.
We need to rethink how we conceptualize individual behavior, access to care, and quality of care. The focus on patient-engaged, patient-centered research of the past several years draws attention to the processes that patients experience in their health service use. The longstanding Andersen individual behavioral model of healthcare use (IBM) describes how the individual and their predisposing, enabling, and need context impact access, use, and health outcomes. 3 The well-known Donabedian health system and quality model (HSQM) depicts how structure and process lead to outcomes that reflect the quality of care provided by health systems. 4 Both models have served as cornerstones of mental health services research. Nevertheless, while both models have been revised extensively, the role of care coordination has been ignored. Without integration of care coordination into health care utilization and quality models, it is challenging to assess its value and impact on mental health outcomes.
We propose a new theoretical model that integrates care coordination explicitly. To accomplish this, we review and combine the current theoretical models. We suggest features, influences, and impacts to guide future evaluation of care coordination.
Evolution of the individual behavioral model
IBM has always included individual predisposing, enabling, and need characteristics and their interaction with the healthcare system.5–7 Early versions had components of access (the outcome of interest) and structure, defined as characteristics of the system that determine what happens to the patient following entry.5,6 For example, having a regular source of care has been associated with improved health outcomes for homeless adults. 8 Structure was distinct from processes, paralleling Donabedian's concurrent work. 9 In 1974, the goal of the model was expanded to inform health policy, service use, and satisfaction with those services. 7 Quality was included as an outcome as well as quantity. The socio-organizational aspects of access were described as system resources that facilitate or hinder the efforts of a client to obtain care, drawing from Donabedian. 10 For example, the measurement of receipt of the preferred type of mental health service (psychotherapy or pharmacotherapy) is important to assess patient-centered care. 11 Subsequent iterations of the IBM explored further dimensions of access including continuity of care, delay in help-seeking, and adherence to a prescribed regimen of treatment.12,13
Reviewing how the model had been used over time, Andersen noted that revisions emphasized the dynamic and recursive nature of the model. 3 For example, there is evidence that experience of healthcare discrimination exacerbates barriers to depression treatment such as forming trusting relationships with providers. 14 These themes emphasize the interaction of an individual with the healthcare system to perceive the need, explore options, learn from the experience of use, and coordinate a plan of care.
Evolution of the health system quality model
Donabedian's model depicts a healthcare system or provider comprising three components: (a) structure, and (b) process, which in turn lead to (c) aggregate health outcomes. 4 Structure refers to the resources required, such as personnel and equipment. The best process measures are those for which there is research evidence that better processes lead to better outcomes. For example, performing routine screening for depression identifies those at risk early so that treatment options can be considered; prescribing counseling or anti-depressants reduces the likelihood and severity of depression symptoms; integrating a social worker in primary care reduces emergency department use. 15 Similarly, the best outcome measures are those over which the health care system has influence. For example, food insecurity may not be an appropriate outcome measure because health systems lack the means to adequately identify those at risk. By contrast, symptom improvement in patients with severe mental illness is a reasonable outcome measure.16–18 Both structure and process dimensions can provide valuable information for measuring quality.
Later adaptions of the Donabedian model distinguished technical care from interpersonal care, as well as expansion to include other outcomes including: safety, effectiveness, patient-centeredness, timeliness, efficiency, and equity. 19 More recent models added patient experience, 20 and provider experience. 21
Building theory from practice-based evidence
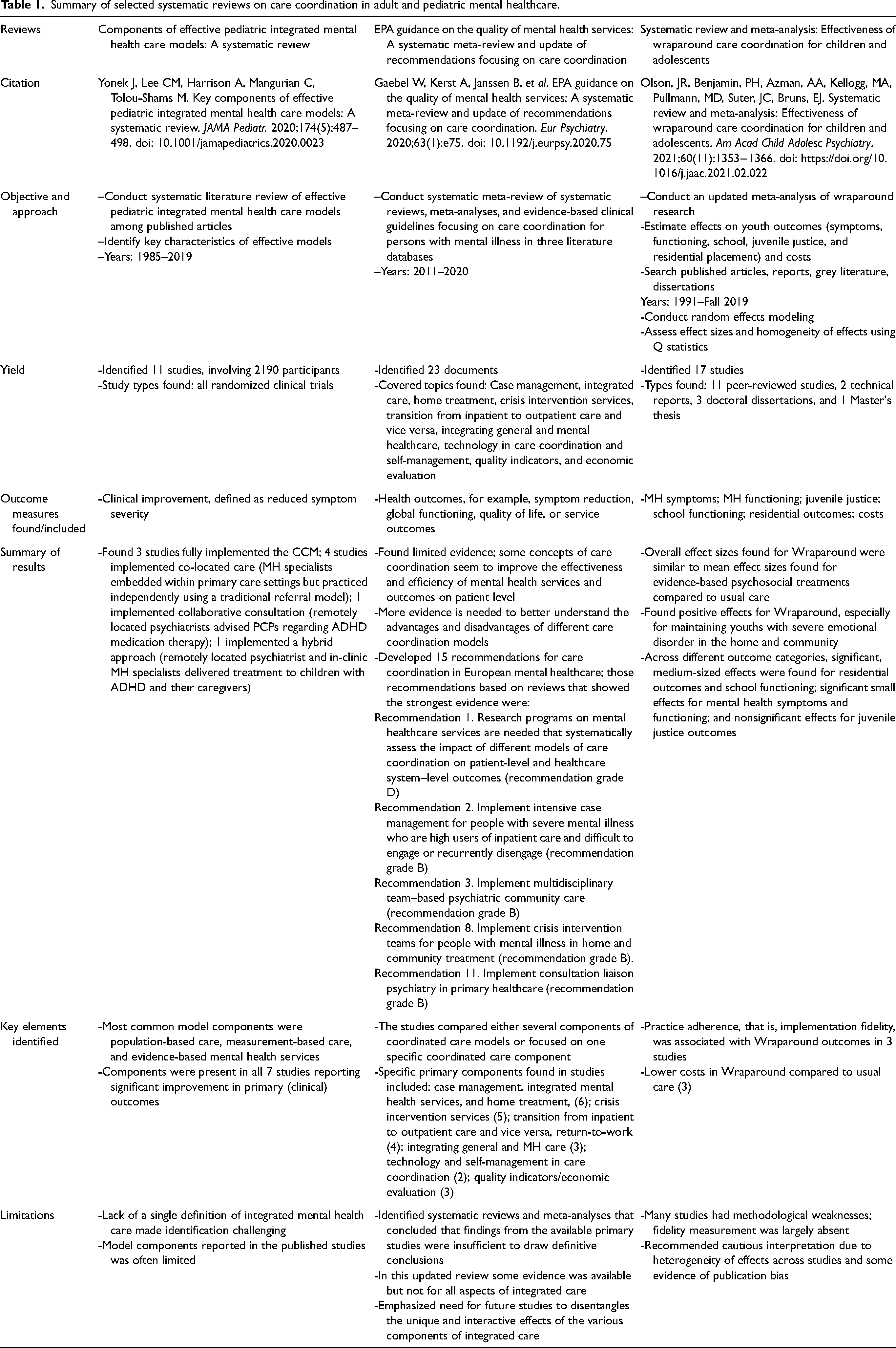
The term “integrated-care” reflects strategies designed to improve the mental health outcomes of people with complex needs, including those with mental health needs. Notable examples include the Collaborative Care Model, 22 First Episode Psychosis Care, 23 and Assertive Community Treatment. 24 In each case, care coordination is an integral feature. Table 1 highlights three systematic reviews of prior research in adult and pediatric populations.25–27 These studies provide evidence that care coordination supports health behaviors and health outcomes for adults and children with mental health conditions.
Summary of selected systematic reviews on care coordination in adult and pediatric mental healthcare.
Care coordination embodies aspects of both structure and process ranging from informational support to advanced knowledge and direct services
Care coordination can also implement processes such as screening for depression or sharing patient data between primary and specialty care. 31 For families of children with mental health needs, important processes include family engagement and co-selection of treatment strategies. 30 Care coordination processes can be key to getting to the right health system or provider at the right time for mental and physical health care needs to be fully met.
In the U.S., in contrast to other countries with national programs for the delivery of integrated-care services, most people with mental health needs receive a variety of care coordination services from different settings and with differing intensity. Few practices have the staffing to implement integrated care, waiting lists are long and satisfaction with services is highly variable.32,33 As a result, evidence on the value of care coordination in real-world settings is mixed. Care coordination has proven successful for improving adult psychiatric patients’ access to care, clinical outcomes, and patients’ experiences.34,35 Yet the unique and interactive effects of the various components of care coordination for mental healthcare are not well understood. 25 Care coordination for children with psychiatric conditions or developmental delay has improved healthcare experiences and outcomes leading to more planning, reduced unmet need, more family-centered care, and greater satisfaction with care.26,36,37 But evidence on key elements of care coordination and their impacts on health outcomes is lacking. 26
An integrated theoretical model of healthcare and care coordination
The overlapping content and shortcomings of the IBM and HSQM together with practice-based evidence point to a need for a new theoretical model that explicitly includes care coordination to generate evidence from real-world settings. An integrated theoretical model of healthcare and care coordination is presented in Figure 1.
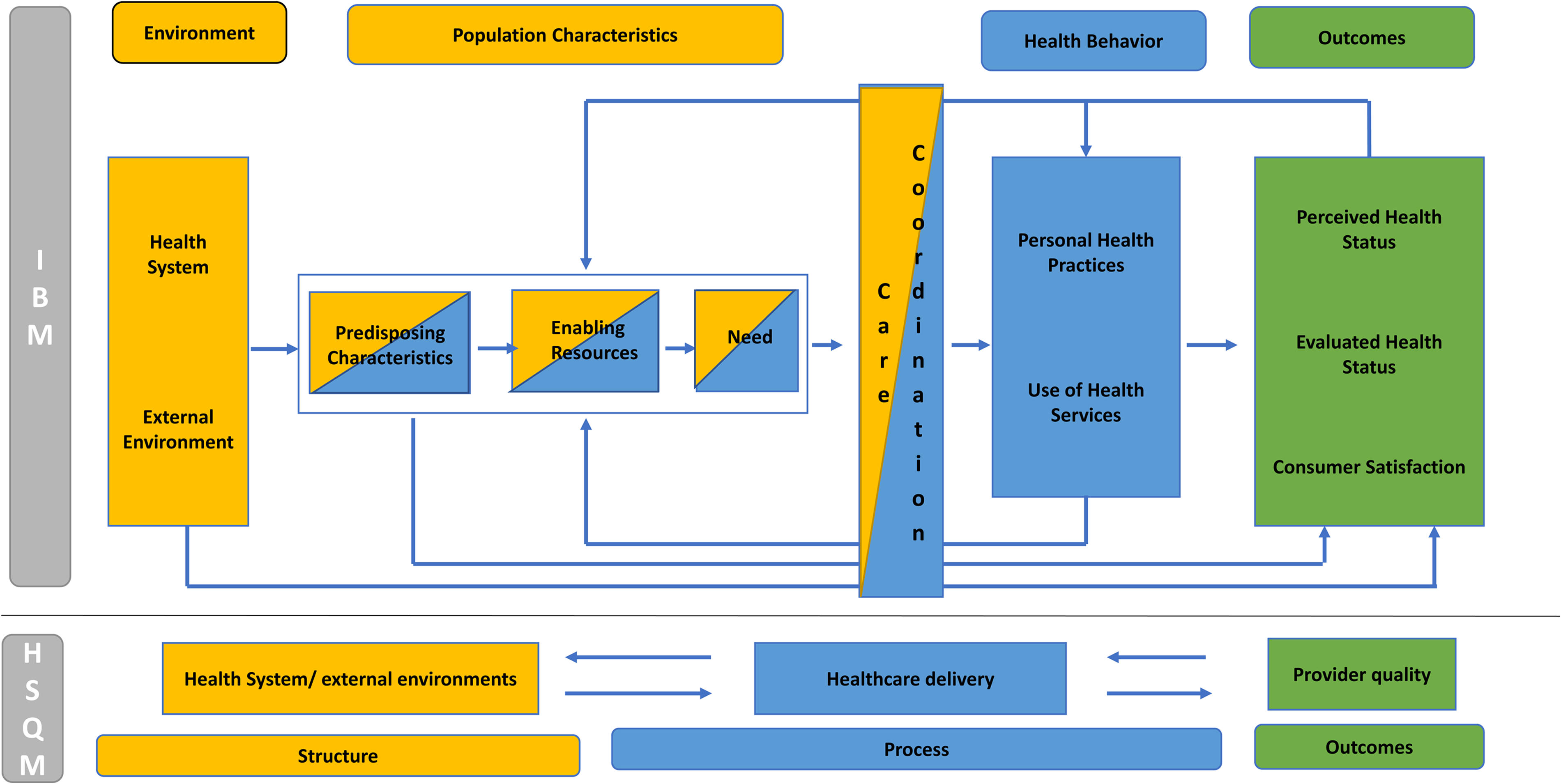
The integrated theoretical model of healthcare and care coordination includes all of the elements of the IBM and HSQM models. Overlap in the individual and system level domains is indicated by placement and color: structure (yellow), process (blue), and outcome (green) at individual and health system levels. The environment domain of the IBM is aligned with the structure domain of the HSQM. The health behavior domain of the IBM is aligned with the process domain of the HSQM. The outcome domain of the IBM is aligned with HSQM outcomes. The population characteristics domain of the IBM is heterogeneous with respect to HSQM domains, sharing structure and process features. For example, the enabling charactistic of individual health insurance includes the structure of plan benefits (premium, copayments, coverage limits, and scope) and the process of its use (poor understanding of mental health benefits, the choice of in- or out-of-network providers, and the experience of surprise out-of-pocket payments).
Care coordination is explicitly integrated with structure and process features. 38 Key practice principles of care coordination include processes (reliable and valid patient assessment, effective communication between patient, caregiver, and provider) and structure (supported linkages between healthcare resources and community, integration across domains of care). 39 Ideally, coordination of care ensures that accountable structures and processes are in place for a comprehensive plan of care across providers and settings in alignment with patient and family needs, preferences, and goals. 40
The need to measure and assess the impacts of care coordination motivates the integrated theoretical model of healthcare and care coordination. The new integrated theoretical model includes feedback loops from outcomes through care coordination and back to the population or individual thereby informing predisposing, enabling, and need factors. In the figure, arrows indicate the direction and relationships with steps in the process. The integrated theoretical model provides a way of understanding and explaining how care coordination works in the context of individual behavior and health systems in practice, and emphasizes accountability features that can be applied in a broad range of real-world practice settings.
Implications for future research
The integrated theoretical model of healthcare and care coordination provides a map for exploring how to improve care coordination and its impacts for mental healthcare. For example, there is evidence of structural racism in the receipt and impacts of care coordination for adults and children with psychiatric conditions. National data provide evidence of racial disparities in parent-reported receipt of care coordination by children with special healthcare needs.41,42 Program-level data show structural racism in the implementation of effective care coordination for adults with psychiatric conditions measured by enrollment, phone outreach, referrals, and patient choice.43,44 Nonetheless, study of the impact of care coordination for people with psychiatric conditions, especially accounting for racial disparities in experience of care coordination, is limited. Multivariate modeling using program data indicates variation in the impact of care coordination by race for children and adults, but these early models do not adjust for selection bias.45,46 Secondary analysis of a randomized controlled trial of care coordination for people with first-episode psychosis found that racial disparities in service experiences were associated with reduced program impact. 47 Future research should identify the contextual factors associated with variation in implementation of care coordination and the individual factors associated with variation in receipt of care coordination. This detail is necessary to document the impacts of care coordination adjusting for selection bias arising from factors such as structural racism or patient preferences. These steps provide a foundation to craft and evaluate care coordination programs that work across a heterogeneous population with psychiatric conditions.
Conclusion
We propose an integrated theoretical model of healthcare and care coordination to guide future research on the value and impact of care coordination on healthcare use and quality and health outcomes. The model builds on established services research models and aligns with recent practice-based evidence to integrate care coordination. The model can serve as a guide for future research to better understand the variation in care coordination services and delivery and its added value to improving mental health in different real-world settings.
Footnotes
Author's note
Denise M Hynes, School of Nursing, Oregon Health and Science University, Portland, OR, USA.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclaimers
The views expressed in this paper are the authors’ and do not necessarily reflect the view of the US Department of Veterans Affairs, the US government, the Oregon State University, or the University of North Carolina at Chapel Hill.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Hynes was supported in part by awards from the US Department of Veterans Affairs Health Services Research and Development Service (SDR 18-321; IIR 20-165; & RCS 21-136) and Oregon State University start-up funding. Dr. Thomas was supported by the University of North Carolina Chapel Hill Eshelman School of Pharmacy.