
Abstract
Introduction
Dementia care is often fragmented and un-coordinated. As the number of individuals living with dementia increases worldwide, navigation programs are a way to help counter difficulties with navigating and accessing services by better integrating care for individuals with dementia and their family caregivers. While navigation programs are increasingly being used, it is not clear how to best implement such programs in North America and abroad.
Methods
Following Arskey and O’Malley's (2006) scoping review methodology and theoretically informed by the Consolidated Framework for Implementation Research, this paper explored existing navigational programs used in dementia care to identify factors to consider when implementing these programs across different settings.
Results
Twenty-two articles were included in this review. Our findings suggest that there is a high degree of variability with how navigation programs are being delivered and no clearly established or standardized protocol to implement such programs. Barriers and facilitators to implementation were identified as they relate to (1) Complexity (Intervention Characteristics); (2) Patient and Caregiver Needs (Outer Setting); (3) External Policies (Outer Setting); (4) Available Resources (Inner Setting) (5) Communication (Inner Setting); (6) Culture (Inner Setting); (7) Leadership Engagement (Inner Setting); (8) Knowledge and Beliefs (Characteristics of Individuals); (9) Champions (Process) and (10) Evaluation (Process).
Discussion
Combined, the findings from this review provide suggestions for implementing navigation in the context of dementia care and suggest several pragmatic considerations (e.g. available resources) when implementing new navigation programs.
Introduction
Persons living with dementia (PWD) and their family caregivers (caregivers) are frequent users of the health and social care system.1,2 PWD, who often require caregivers to help them, navigate through a fragmented healthcare system where there is little guidance provided. 1 Despite a wide range of health and social care services available to PWD and caregivers at these transition points, numerous studies highlight that caregivers to PWD often underuse services due to difficulties navigating the system, and a lack of knowledge about accessing service availability. 3 A study by Stephan and colleagues on service utilization by PWD across eight countries concluded that having a single healthcare professional (HCP) coordinate care could help decrease caregiver burden and improve quality of life for PWD. 3
Patient and system navigation (here within referred to as navigation programs) have emerged as a promising approach to integrated care management for older adults with complex conditions.4,5 Definitions of navigation programs vary,6,7 but they often consist of an individual or virtual modality providing support in accessing healthcare resources. 4 For the purpose of this study, navigation programs are defined as a program wherein PWD and/or their caregivers are supported through any modality with the goal of improving the timeliness and ease of accessing health and social care services or the coordination amongst various services or HCPs.
With the growing popularity in navigation models of care, several knowledge synthesis projects have been conducted assessing their delivery model and/or efficacy. For instance, one review concluded that the role and function of navigators varies across programs and may include professional navigators, case managers or lay navigators, 8 which can make implementing such programs difficult. As well, a 2021 review of navigation programs for adults aged 26 and older with complex care needs identified some useful recommendations on how to structure and manage navigation programs. 4 However, this review focused solely on programs that used patient navigators, had a limited search strategy that did not include other synonyms of navigator programs, and thus may have inadvertently excluded articles on navigation programs in the context of dementia. 4 Recent work by Banerjee and colleagues 9 reviewed the clinical- and cost-effectiveness of patient navigation programs for PWD, as well as evidence-based guidelines on patient navigation for any medical condition. However, it did not synthesize findings related to implementation characteristics that could inform future program delivery and implementation. Thus, a comparison of various approaches to navigation in the context of dementia is merited. Moreover, there is a need to further explore the implementation facilitators and barriers to each to establish initial guidelines for increasing the use of navigators and ways to optimize their implementation across various settings.
The present scoping review aimed to address these gaps in knowledge by (a) characterizing the approaches used to deliver navigational support to PWD and their caregivers; (b) examining implementation barriers and challenges for various navigation programs; and (c) identifying strategies to ensure successful implementation of navigation programs. This assessment of the literature aims to advance our knowledge on how to successfully advance navigation programs worldwide to help better support PWD and their caregivers utilize health and social care services.
Methods
Design
A scoping review guided by Arksey & O'Malley 10 (2005) and Levac, Colquhoun and O'Brien 11 was conducted. The six-stages guiding this scoping-review process included: (i) identifying the research question, (ii) identifying relevant studies, (iii) study selection, (iv) charting the data, (v) collating, summarizing and reporting the results and (vi) consultation. 10 A protocol of this review has been published on the Open Science Framework (i.e. https://osf.io/hzd73).
Study questions
In this scoping review, the following two questions are addressed:
What has been reported in the literature regarding the implementation characteristics of existing navigation programs for PWD and caregivers in different care settings? What strategies may support the implementation of navigation programs for PWD and their caregivers?
Search strategy
A comprehensive search strategy was developed and conducted by an academic research librarian and informed, in part, by existing related reviews (i.e.4,9 and peer reviewed literature). 12 Search strategies included the use of text words and subject headings (e.g. MeSH and Emtree) related to (1) navigation, (2) dementia (see a sample of the search strategy in Supplemental File 1). The following databases were searched on 30 September 2021: Ageline, Cochrane Central Register of Controlled Trials (CENTRAL), CINAHL, Cochrane Database of Systematic Reviews, Embase, Ovid MEDLINE(R) (including Epub Ahead of Print, In-Process and Other Non-Indexed Citations), Ovid MEDLINE(R) Daily), OTSeeker, PeDRO, PsycINFO and Scopus. Reference lists were scanned to identify additional studies.
A search for the grey literature was conducted through national and international healthcare and government websites using keywords identified through the development of the academic search strategy. The authors also reached out to key stakeholders for relevant literature at regional Alzheimer's Societies in the Greater Toronto Area (Canada).
Search selection
This review included articles that focused on navigation programs for PWD and their caregivers. Studies were considered relevant for this review if they met the following inclusion criteria: (i) written in English, (ii) published from January 1990 to 30 September 2021, (iii) implemented navigation program(s) whereby the focus of the program was primarily on PWD, including individuals with mild-cognitive impairment (MCI) aged 50 or older, and delivery and implementation of the program was described, and (iv) full-text articles available. Programs that are designed for adults with cognitive deficits that may be due to a psychiatric condition or alcohol-related dementia were excluded. There were no restrictions on the geographical origin of the paper, but review articles were excluded. Grey literature had to have enough detail on the program delivery and implementation to be included.
Two reviewers were involved in study selection (KMK and ZL). Each article was reviewed in duplicate at all steps (i.e. title and abstract screening, full-text). Discrepancies were resolved through a discussion of the article with a third-reviewer (SLH). Covidence software was used to manage the review process. 13 Figure 1 details the search selection process.
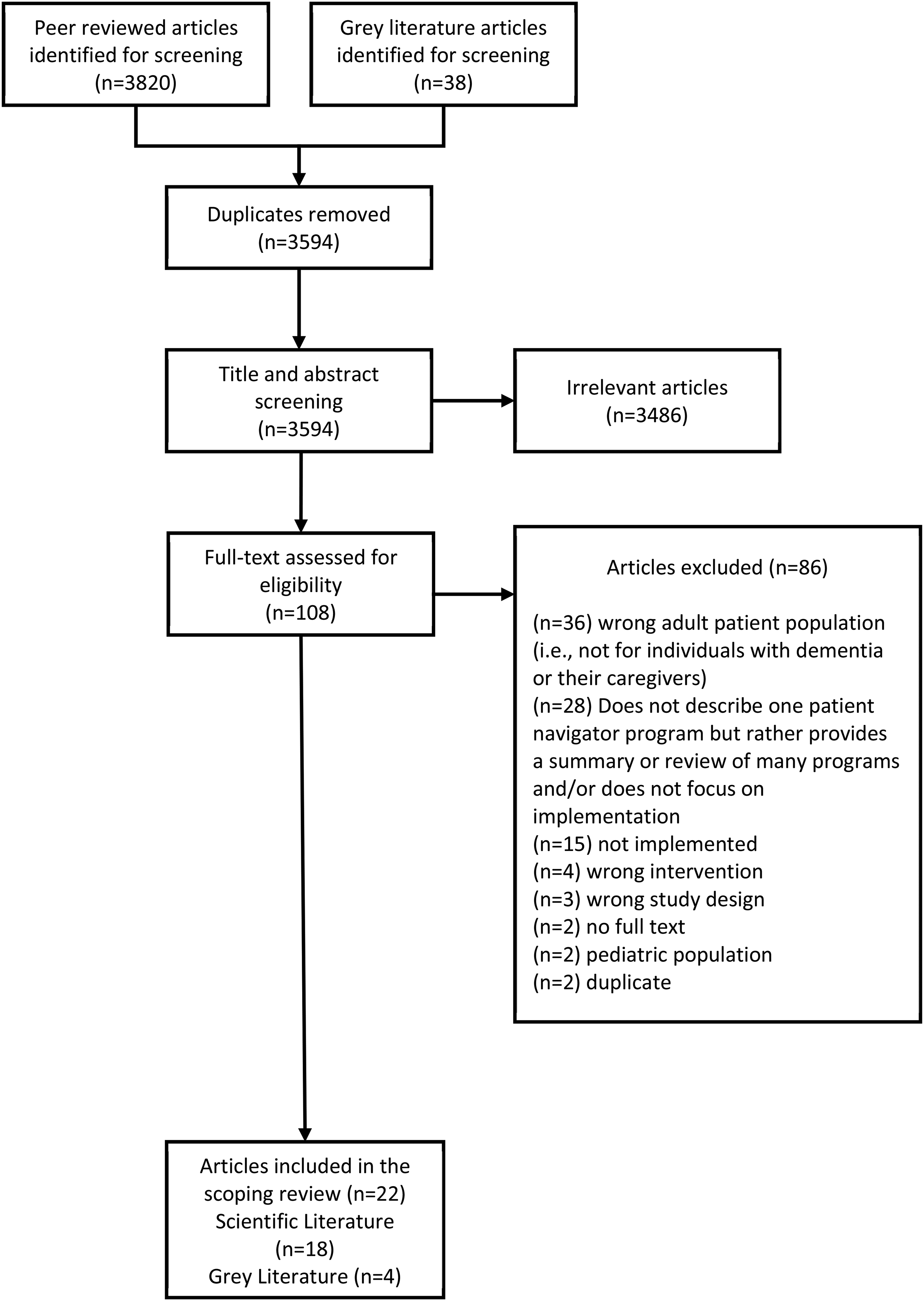
PRISMA.
Charting the data and data analysis
The study team developed a standardized data abstraction form that was piloted on a single article by all authors. After the piloting and refinement of the data abstraction form, two authors (KMK and ZL) independently read the included full-text articles and extracted data from them. Bi-weekly meetings occurred during the extraction phase to resolve ambiguities. The first author then reviewed all the extracted data and condensed the individual reviews. Following charting of the data, 10 data analysis was completed by all authors to identify themes. The authors utilized thematic analysis to appraise and categorize our included articles to report patterns (themes) within the data. 14 Analysis included a thorough review of the charted data, written ideas and a discussion about data, identification of patterns across and within each of the studies and a categorization of patterns, and giving patterns a final theme label. 14 During analysis we considered characteristics that were facilitators to implementation rather than a barrier.
Analysis was guided by the Consolidated Framework for Implementation Research (CFIR). 15 The CFIR is a comprehensive determinant framework that contains 39 constructs that influence implementation and are organized in five domains: (1) intervention characteristics (e.g. complexity), (2) outer setting (e.g. external policies), (3) inner setting (e.g. culture), (4) characteristics of individuals (e.g. knowledge about the intervention), and (5) implementation process (e.g. engaging stakeholders). 15
Engagement and consultation with stakeholders
The authors engaged via videoconferences with the staff at two local Alzheimer Societies wherein study questions were refined. The authors also engaged with a stakeholder advisory team that included a patient navigator, a community health service leader who oversees programming for individuals with dementia and an inter-professional practice hospital leader. Lastly, the authors organized a videoconference with all stakeholders to present preliminary themes prior to the manuscript being prepared for publication.
Results
The search located 3,820 peer-reviewed articles and 38 grey literature articles. Based upon the inclusion and exclusion criteria, 18 peer reviewed articles and 4 grey literature articles were included in this review (n = 22). Of the included studies, 12 had quantitative study designs, 3 had qualitative study designs, and 3 employed mixed methods. Of the qualitative studies, all employed interviews. Of the quantitative studies, six were randomized control trials. One study used a case study approach. 16 The included studies were predominantly conducted in North America. Navigation programs were implemented in the United States (n = 13), Canada (n = 3), Australia (n = 2), United Kingdom (n = 1), Netherlands (n = 1), New Zealand (n = 1) and Germany (n = 1). Only two studies focused specifically on rural populations.17,18 Five studies reported on the same program (The Care Ecosystem).19–23 The characteristics of the included articles are presented in Table 1.
Characteristics of included peer-reviewed studies and grey literature.
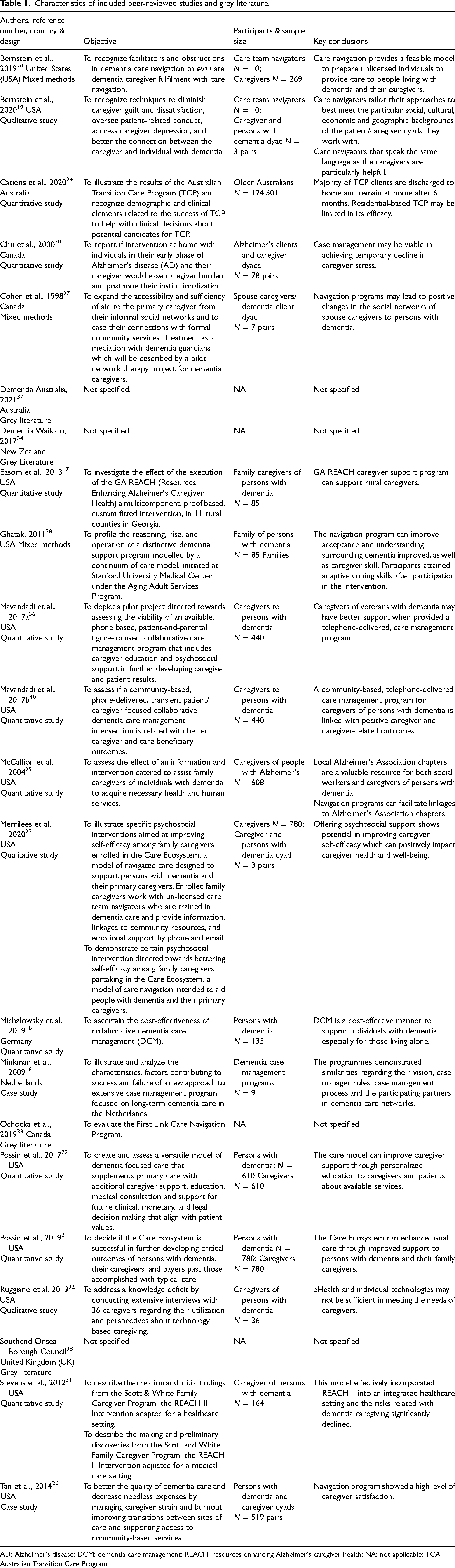
AD: Alzheimer's disease; DCM: dementia care management; REACH: resources enhancing Alzheimer's caregiver health; NA: not applicable; TCA: Australian Transition Care Program.
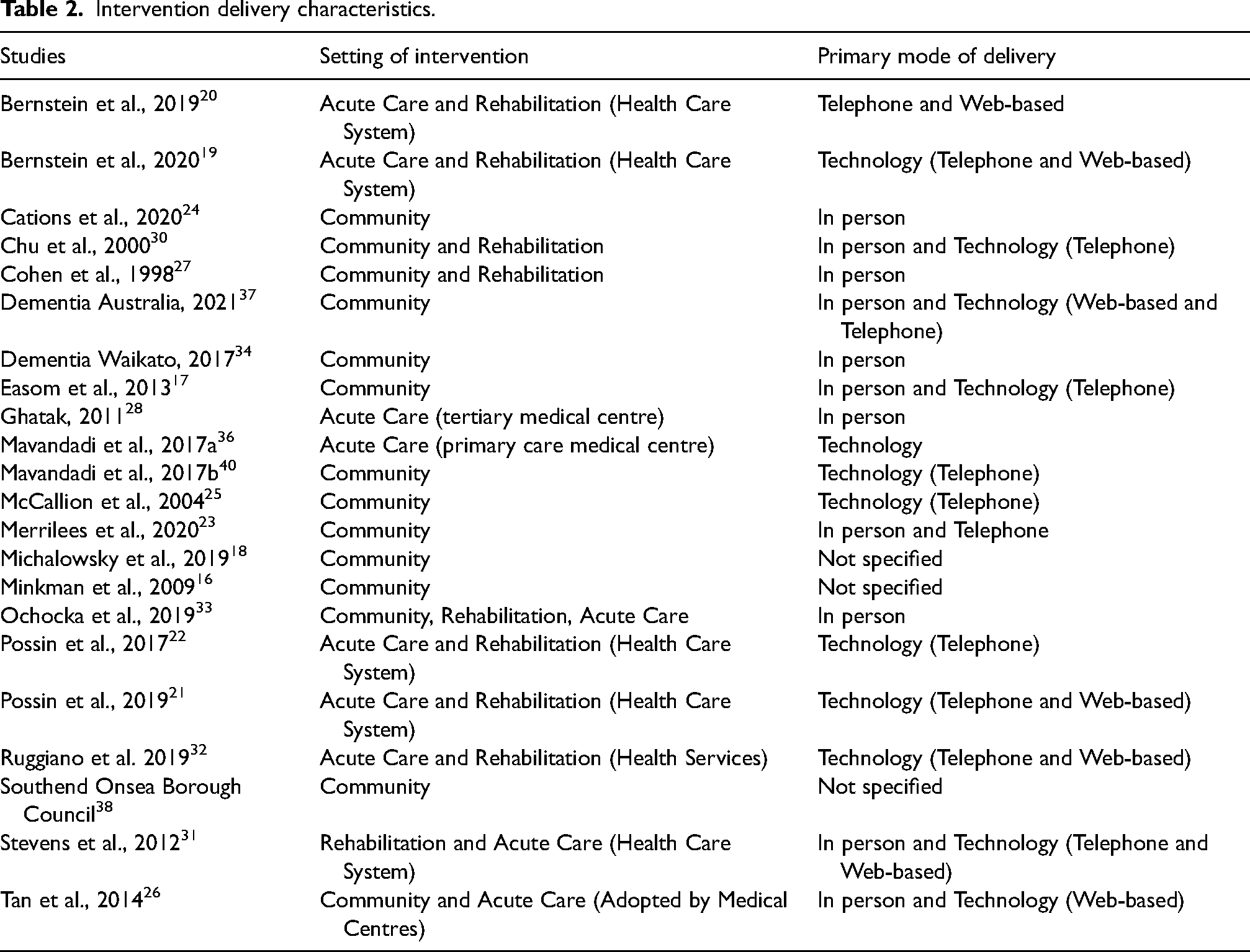
Most articles did not provide a definition of navigation, and instead operationalized navigation in the context of their study. Definitions largely involved the notion of individualized and continuing quality community-based support to help PWD and caregivers access health and social care services by addressing barriers to care.19,20,22,24–27 Programs were delivered through different modalities (Table 2).
Intervention delivery characteristics.
Study participants in the peer-reviewed articles were generally caregivers (n = 7) with six studies including both PWD and caregivers. Four studies discussed comorbidities of PWD24,28 that included cardiovascular disease, arthritis, depression, stroke and diabetes.21,22 No study included individuals with MCI.
Implementation determinants
The initiation of navigation programs were described as time-consuming and complex.16,29 The most prominent determinants influencing the complex nature of implementation (as barriers or facilitators) were identified to be: (1) Complexity (Intervention Characteristics); (2) Patient and Caregiver Needs (Outer Setting); (3) External Policies (Outer Setting); (4) Available Resources (Inner Setting) (5) Communication (Inner Setting; (6) Culture (Inner Setting; (7) Leadership Engagement (Inner Setting); (8) Knowledge and Beliefs (Characteristics of Individuals); (9) Champions (Process) and (10) Evaluation (Process). Of these characteristics, we noted the facilitators to support implementation to be multi-component programs (complexity), sufficient human and financial resources, including trained navigation staff (available resources), communication amongst all care professionals (communication), a culture of collaboration (culture), strong leadership (leadership engagement) and the presence of champions (champions).
Complexity
Navigation programs tended to be multi-component, adding to the complexity of their implementation. All programs were identified to provide a combination of informational support (i.e. education on dementia-specific behaviours),18,20,23,26,28,30–34 referrals to health and community resources (e.g. to facilitate a diagnosis 34 ),16,19,20,23,26–28,31,33,35–39 ongoing monitoring of the dementia diagnosis, supportive counselling and emotional support,16,18–20,29,31,33,34,36,38,39 family meetings 28 and caregiving skill training16,19,20,23,26,30,31 and/or coordination of care.16–18,28,29,36 One of these programs only provided linkages to government-funding to support dementia care. 37 Only two programs were identified as facilitating peer-support.33,38
Multi-component programs also included service offering such as therapies aimed at improving physical, cognitive and psychosocial functioning. 24 Programs were also differed through different modalities, with most including multiple forms of contact, including by phone,17,19,21–23,36,40 Internet,19,21–23 postal mail 23 or home visit30,34 to enable a broader geographical reach.23,40 Only one of these programs offered one component, which was connections to services. 25
Complexity of programs was also influenced by the number of individuals needing to participate in the intervention,16,20 such as programs being delivered by state-based public health services 24 or through multidisciplinary teams in the areas of case management, occupational therapy, geriatricians, physical therapy, social work, nursing, respiratory therapy, homemaking, and psychiatry.28,30 Often, these individuals work through various inter-organizational clinics to support both in and out patients, 28 given the high prevalence of comorbid conditions in amongst PWD.
Patient and caregiver needs
Navigation programs largely operated to meet PWD's needs and by extension, that of their caregivers.16,20,36 Only one study focused on the cross-cultural differences amongst caregivers and the need to potentially tailor solutions for navigation according to different cultural needs. 32 Three authors noted that part of what makes implementing appropriate dementia support so difficult is that PWD and their caregivers’ needs change as the illness progresses or depending on the systems exhibited by the PWD at a given moment.20,26,32 Programs tended to be tailored to meet individual needs,17,19,20,23,24,26–28 developed in consultation with PWD 24 and caregivers, 25 with programs being offered either in individuals’ homes,17,28,30,34 residential facilities or in hospital or community clinics.24,40 Moreover, navigation programs aimed to compensate for the lack of social supports to meet caregivers’ needs for support. 31 Thus, the importance of end-user-involvement throughout the whole process of developing and delivering navigational support programs and allowing for enough time to continuously refine programs to end-users-needs were recurrently identified as important facilitating factors. 33
In one study, considerations around the PWD's capacity for decision-making informed the delivery of support, such that it informed whether or not the program necessitated the involvement of caregivers. 26 In another study, caregivers in particular had to be interested in receiving services in order to use them; suggesting that navigation programs may facilitate referrals that do not always get taken up by those who need them. 25 In addition to needs stemming from PWD and caregivers themselves, organizations involved in navigation advocated for the needs of their clients and caregivers. 16
External policies and programs
A few programs were integrated into existing healthcare systems that were described as having multiple workings and a clear split between acute health care, long-term and chronic healthcare and social care.16,31 One program was informed by existing dementia service navigation programs. 23
Two programs were fully integrated into the Australian aged care system,24,37 suggesting that in order for the program to be system-wide it had to align with external policies in Australia and those of multiple organizations, although these were not described. Other programs described integrating their program within academic hospital systems.26,28 Moreover, those responsible for leading the integration were not mentioned. Some programs were offered in collaboration with their local Alzheimer's Society.16,25,27 In the context of hospital-based programs, existing hospitals and their outpatient clinics do not have a continuum of care model, 28 influencing the way programs could be delivered within their existing models of care.
Available resources
Navigation programs required numerous human resources, with expert knowledge16,21,22 and multispecialty group practices. 31 Individuals in the program ranged from social workers16,25 and geriatric nurse practitioners16,26 to unlicensed trained dementia specialists (e.g. Care Team Navigators19–22) who were supported through training and supervision by clinicians with dementia expertise (i.e. practice nurses, social workers, pharmacists16,19–23), staff of the local Alzheimer's Society16,25 or from Veterans Affairs.17,36,40 Training was provided to unlicensed HCPs for approximately 80 h and included communication skill-building and learning to locate information and community resources. 23 In addition to training, navigators required the opportunity to clinically debrief with their HCP colleagues.21–23
In addition to individuals assisting with navigation, there was also a reliance on community organizations to follow up, accept clients of the programs, and offer their services.17,25,31,33,40 Partnering with community agencies was a facilitator to implementation, particularly those with intervention an existing integrated healthcare system. 31 By partnering with organizations focused on dementia care, partnerships between navigation programs and not-for-profit organizations/agencies were able to assist with the support of family members who care for individuals with dementia through numerous social and health services.17,25,31,33,40
Conversely, programs that begin at the point of hospital discharge require a supportive hospital organization that is willing to implement new models of care.26,28 Other programs described the need for long-term care familiarities to have the capacity to accept new referrals. 16 For programs that aimed to facilitate primary care services, a reliance on family physicians to accept PWD and caregivers was noted.18,20 In additional to standardized referrals, standardized workflow management tools were required to care team navigators to document care plans, and other relevant information such as community service providers. 23
Financial considerations were highlighted as both a barrier and facilitator to program implementation and delivery. For instance, navigation programs discussed the need to ‘pool family resources’ to best care for PWD. 28 However, many of the clients being seen in system navigator programs had financial limitations or did not qualify for insurance benefits 20 or lived in rural areas,21,22 thus requiring programs to assist with financial support in low resource areas as well. Financial resources (i.e. funding sources) were only explicitly discussed in one study, 17 although others mentioned the supportive role of philanthropic organizations26,31,39 or government-sponsored funding.33,37,38
Embedding appropriate communication
Programs had to communicate in a manner that is meaningful to their clients. 23 System navigator professionals were often expected to use appropriate communication (e.g. person-centred language) as a means of facilitating ongoing relationships and developing an in-depth understanding of how to provide tailored support with caregivers.20,33 Regular multidisciplinary meetings aimed at improving end-user care also benefitted the implementation of these programs.16,19–23,33
To support the heterogeneity amongst PWD and their caregivers, programs aimed to connect individuals with services in their native tongue. 19 Providing support to PWD with complex family dynamics or for individuals without family support (e.g. live alone) and are resistant to care, requires more frequent and prolonged communication. 28 Web and texting based communication was also offered to caregivers19–23,26,32 and served as a means of them connecting to HCPs for navigational support. 32
Individuals with delegated roles aimed at improving service use for PWD and caregivers had to be willing to make frequent attempts to contact services, such as the Alzheimer's Societies to ensure referrals were being attended to. 25 However, research exploring the response rate of a local Alzheimer's Society found that staff at the organization had difficulty getting in touch with many of the caregivers by telephone. 25
In addition to communication amongst system navigators and their clients, a few studies commented there also needs to be discussion among various HCPs about integrating support programs and services,16,28 as well as patient-specific information.16,26 Having systematized referral and communication mechanisms put in place was seen as a facilitator to ongoing communication amongst different providers and care sectors to refer caregivers and PWD enrolled in navigation to formal services (e.g. respite care).16,26,31 Accordingly, by having automated and standardized processes for communications, referrals were believed to be better facilitated and in turn, improving access to care.31,32 Technological advances were identified as fostering a new way of working to improve healthcare locally and regionally. 32
Collaborative culture
The organizational structures and local cultures of collaboration varied amongst the programs.16,31 Some organizations formed a culture of collaboration with existing community services needed to support PWD such as adult day care, legal services and financial planning.26,31 To ensure collaboration, partnerships with these community-based organizations were formally established through memoranda of understanding. 26 The initiating community-organizations operated from a culture of supportive care and were mostly in the area of acute care, community/ home care and long-term care that could work as part of a network to execute or support the program.16,26,31 The need for more dementia-friendly culture through collaborative partnerships was also expressed in some of the articles.33,34 For instance, this included more awareness about the disease. Technology, in particular, was determined to foster networked service delivery and collaboration between different care silos and helped to foster a commitment to global improvements in healthcare. 32
Several studies were identified as having an organizational culture (i.e. training, role resourcing and access to a staff-peer network) that offers role support for individuals taking on navigation roles in the context of dementia (i.e. training, role resourcing and access to a staff-peer network).16,19–23 Facilitating factors for a collaborative culture included having a well-functioning and stable team of various providers that were specialized in dementia care and flexible organizational structures to allow these providers to work together.19–23,28,30
Leadership engagement, motives and tasks
By virtual of their role, system navigators had to take on a central and independent role in facilitating care amongst different and related sectors, providers and organizations to provide continuity of care. 16 However, other programs described that the urging of system navigators to lead continuity of care plans stemmed from leadership at the local governmental level, in cooperation with the local HCPs who were also requesting this need.16,21,22,33,38 Programs had to align with the mandates of their local health governments, such as improving health and lowering health care costs through avoiding hospitalizations.21,33,34,38 While governmental support helped to facilitate program success, changing regulations and priorities can negatively affect advocacy for particular programs which in turn, effect implementation. 33 In addition, system navigators, the presence of a research staff in implementation or the process of delivery was identified in all of the peer-reviewed articles.
Knowledge and beliefs
Knowledge and beliefs about the navigation programs were addressed in all articles. However, some of the articles also discussed the knowledge and beliefs of end-users. In the unique context of dementia, challenges with the progressive nature of the illness and unacceptance of information concerning the dementia progression (particularly at diagnosis) were found to hinder family caregivers’ use of service and thus required programs to continuously re-share information for individuals and provide ongoing training for changes in PWDs’ functional and behavioural decline.16,28,30,32 Individuals in the program with a delegated role to help connect PWD and caregivers to services had to convince clients of their need for services.25,28 Some programs focused on influencing caregivers’ beliefs around dementia by preparing caregivers for what is coming next in the dementia illness trajectory in order to address expectations related to services and help support service decision-making around service use. 19
Many of the caregivers enrolled in the current navigation programs expressed concerns of long-term care placements, 19 and thus part of the role of navigation programs were to support with the decision-making process around long-term care and helping caregivers overcome guilt.19,24
Champions
Engaging champions was implied in ten of the articles. Champions ranged from individuals who are internal to an organization, such as HCPs16,19,26,28 to those external to the organization who are able to lead to the conviction that the implemented program would be successful 16 (e.g. individuals in local public health authorities, 24 Alzheimer's Societies 25 ). In the context, of HCP, they also facilitated a dementia diagnosis that helped facilitate access into the navigation program.16,26 Champions were also required to support the translation of programs to other geographical locations.17,22 None of the studies measured the ‘champion effect’, or the mechanisms by which champions influenced their implementation processes and related outcomes.
Evaluation
Very few programs were implemented with a formal implementation evaluation approach put in place. In the pilot of one program, ongoing case studies were conducted to support the implementation of navigation programs for PWD in hospital settings. 28 Another program, aimed to conduct an ongoing evaluation to determine the feasibility of using multiple different intervention approaches and used this information to target the need for more research around a tailored approach which assessed the risk or needs of the caregiver. 17 The third article that described implementing an evaluation approach described using an existing framework to guide the evaluation of community-based caregiver interventions through five dimensions: (1) Reach into the target population; (2) Efficacy or effectiveness of the intervention; (3) Adoption by target settings/institutions; (4) Implementation through consistent delivery of the intervention; and (5) Maintenance of effects in individuals and populations over time. 31 None of these studies focused on the outcomes of the implementation.
Conversely, all of the peer-reviewed publications did involve some form of outcome evaluation following their implementation. For example, The Care Ecosystem program had been tested through a randomized control trial and through qualitative methods.19,21–23 Moreover, none of the included studies assessed factors that impact the success of their programs, 24 although one grey literature source did highlight personal characteristics (i.e. need for more navigators) that may influence future program delivery in their year two evaluation. 33
Discussion
The present scoping review characterized the various implementation characteristics being used to successfully apply dementia-specific navigation programs to help integrate care across various care settings, including the facilitators that support the implementation of navigation programs for PWD and their caregivers. The search identified 22 articles, with the majority from the United States. There were no standardized protocols for implementation approaches and implementation was described as being complex. Key factors to successful implementation identified in this review included offering multi-component programs to meet the diverse needs of PWD and caregivers through sufficient human and financial resources, trained navigation staff, a culture of collaboration, strong leadership, support of champions and communication amongst multidisciplinary HCPs, organizations, and end users. Although some of these implementation characteristics could be applied to other patient navigation programs, our review also identified barriers were often related to the complex and individualized, progressive nature of dementia. Thus, this review enriches implementation science in the context of navigation for PWD and can enhance support provided to organizations looking to implement navigation for PWD by comprehensively identifying implementation characteristics. 25
The identified influences on implementation provide a theoretical foundation to guide the implementation dementia-specific navigation in new settings. The data identified in the articles fit the predefined constructs of the CFIR. As with another review on patient navigation in the context of chronic conditions, 4 the authors also noted the need for funding, multidisciplinary engagement, appropriate mechanisms for communication, in-kind support and the need for champions. However, the authors also identified that the content of navigation programs and context of implementation should consider the phase of dementia, unique and progressive needs of PWD and caregivers and preferred methods of communication and service delivery.
System navigators must also invest in long-term support for their clients given barriers to providing dementia care (e.g. a lack of understanding of needs, a lack of understanding of the disease). Some studies specified certain characteristics of the implementing organization itself in terms of their partnership with community-agencies and reconciling community characteristics (e.g. active facilitation of the service uptake). However, barriers posed by this necessary collaboration included the need of existing community-services to accept clients of the navigation program and the need for caregivers to accept services.17,25,31,33,40 Finally, our review suggests that streamlining processes for communicating with multidisciplinary teams, particularly primary care physicians who provide diagnostic support is required. Future organizations looking to implement dementia navigation programs should take into consideration such contextual factors at multiple levels of the health and social care system including the providers needed to be involved, the organization and current support provided at system levels.15,41–43
This review did not identify a protocol for implementing navigation programs into existing dementia care. A systematic review concluded that those looking to implement new programs in the context of chronic illnesses, such as dementia, require clear implementation plans to avoid any misconceptions of the desired outcomes of the proposed program. 41 Outcomes of the implementation of the different programs were not discussed. As such, implementing these multifarious navigation programs is difficult. Existing research on program implementation complexity posits that if implementing organizations believe delivering the program to be simple, then the program is more easily implemented into existing healthcare service delivery.41–43 High degrees of complexity in any implementation effort has been found to lead to conflict amongst stakeholders, such that complexity acts as a barrier to implementation. 44 However, programs identified in this review all aimed to meet individual PWD and caregiver needs. Thus to overcome the complexity of interventions, future navigation programs are encouraged to facilitate implementation by fostering belief amongst service providers that their intervention is being implemented for the purpose of helping PWD, rather than just change for the sake of change. 41
Many of the programs did not consider an evaluation of their implementation approach. Therefore, there is an evident lack of research around the factors that could best lead to successful and sustainable implementation. While the results from this review builds upon the existing body of literature, combining the findings of this review with future evaluation research can be used to help create a standardized framework to support the evaluation of the implementation of dementia navigational support programs. Such a framework could assist in the standardized evaluation of the implementation of a large-scale dementia navigation program by being used to determine what constructs identified in this review are most important to consider while implementing navigation programs into dementia care.
Limitations
Our study relied on a singular definition of navigation and thus may have excluded other articles of navigational support that may involve different types of implementation considerations. Another concern is regarding the lack of consistency in the operationalization of the definition of navigation in the included articles. As such, this was up to the authors’ interpretation. Lastly, this review included articles in the English language only.
Conclusion
The current scoping review demonstrated that the implementation of navigation programs for PWD required the concentrated effort of the implementing organizations, the current healthcare system, philanthropic donors and the required HCPs. Thus, implementation of such programs in new settings requires attention to many complex and interrelated factors. Our results indicate that while some factors could influence any navigation program, the unique and progressive nature of dementia also influences implementation. Specialized dementia training amongst the implementation and delivery program team is of great importance. Future studies are encouraged to consider the influence of barriers and facilitators to implementation in a variety of contexts (e.g. low-income areas) to determine what factors can be easily manipulated to enhance future implementation outcomes Moreover, the long-term effects of these barriers and facilitators on program success and sustainability should be considered. Overall, this scoping review provides an initial set of key considerations on implementing navigation programs to augment existing dementia care.
Supplemental Material
sj-docx-1-icp-10.1177_20534345231151208 - Supplemental material for Understanding implementation characteristics in navigation programs for persons living with dementia and their caregivers: A scoping review
Supplemental material, sj-docx-1-icp-10.1177_20534345231151208 for Understanding implementation characteristics in navigation programs for persons living with dementia and their caregivers: A scoping review by Kristina M Kokorelias, Zoe Li and Sander L Hitzig in International Journal of Care Coordination
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Slaight Family Foundation, Alzheimer Society of Canada.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.