
Abstract
Introduction
Care coordination has been part of social work for some time. It has been recognized as contributing to care coordination for long-term care for the elderly and mental health but less is known about their contribution in primary care with patients with complex health and social needs. As social workers are increasingly present in primary healthcare, this scoping review aims to provide a synthesis of social workers’ coordination activities for patients with complex needs in primary healthcare.
Methods
CINAHL, Medline, Scopus, SocioIndex, Social Work Abstracts, and ProQuest databases were searched, from 2004 to 2020 for peer-reviewed literature. A thematic analysis using deductive and inductive approaches was used to conduct this scoping review.
Results
Eighteen studies on 11 different care coordination interventions were included. The care coordination activities have been classified into four categories: 1) activities that target the patient, family, and caregivers; 2) activities that target health and social care professionals and services; 3) activities that link the patient and family with health and social professionals and services; and 4) cross-cutting activities that support and enhance other activity.
Discussion
A variety of care coordination interventions conducted by social workers were identified, all of which included related but different activities. Still, the common aim is to reduce fragmentation of care. Social workers, because of their disciplinary skills characterized by linkages to nonmedical services, can make a significant contribution to the coordination of care in primary health care, in collaboration with nurses.
Keywords
Introduction
Governments and healthcare authorities have a growing interest in the integration of care, 1 and numerous countries have recognized the need to change the fragmented healthcare system for a more coordinated one. 2 Significant cost growth related to health, aging populations, more sensitivity to the patient's point of view, and the quick increase of comorbid chronic diseases3,4 seem to find some answers in a more coordinated care system. It has been noted that an integrated care system could improve population health and reduces or stabilizes per capita costs. 5 Furthermore, through a systematic review, Baxter et al. showed evidence that integrated care increases patient satisfaction, improves the perceived quality of care and enables access to services. 6
Case management is the most widely used professional coordination mechanism in Organisation for Economic Co-operation and Development countries and social workers occupy the majority of these positions around the world. 7 Historically, case management has long been a component of the social work profession. 8
Social workers play a significant role in care coordination centered on the needs and preferences of patients and their families. 9 Their contribution is well known for patients with complex and chronic conditions who have traditionally been institutionalized in long-term care as the preferred option such as elderly people facing diminishing autonomy and people with mental health problems. 10 However, less is known about the social workers’ specific contribution to the care coordination for people with complex health and social care needs in primary healthcare settings.
In the current study, complex needs are defined as: “Complex health and social care need result from multiple concurrent chronic conditions, functional and cognitive impairments, mental health challenges and social vulnerability, the individual's characteristics, and a major change in his life or care trajectory.” 11 As complexity increases, 12 the coordination of care requires more than the management of a single condition or disease, 13 and must be more than simply coordinated through relational willingness. This is particularly important for people who require support with functional autonomy and chronic conditions impacted by social determinants of health. 14 It becomes very relevant when patients with complex needs transition from one care context to another. 15 Care coordination by social workers is also useful when the needs of the person with a chronic disease require services outside the broader health field (school, work, housing, etc.).
This significant contribution should be brought to light and appropriately acknowledged, especially given the relatively recent developments in social work. Several current developments require social workers to broaden their practices in the health sector.16,17 The emerging profession of medical social workers 18 or social prescribing strategies 19 is still little-known in the social work field. But this expansion of social work has been shown to have positive effects on patients,20,21 because it allows a broader consideration of the patient's needs. 22 Two of the many driving forces behind these transformations of social work are the need for a more integrated organization of health and social services 23 ; and the development of coordination practices often assigned to social workers. 24 Other motives include 1) the dissemination of interprofessional conceptual models such as the chronic care model 25 ; 2) more open conceptions of health that include social determinants and well-being (e.g., the definition of the World Health Organisation where health includes well-being); 3) the priority given by public policy to biopsychosocial complex clinical situations 26 ; 4) community, population and primary care approaches that raise the need for a more home-based, community-based, ambulatory, or transitional intervention 27 ; 5) more integrated organization of health and social services 22 ; and 6) the development of coordination practices often assigned to social workers. 24 Some even believe that these developments are part of a renewed recognition for social workers, who are increasingly called upon to play a central role in the modernization of social and health care systems. 28 To fulfill these functions and meet the expectations of this new organization of services, social workers must be closer or present in medical clinics, which is not always the case. Their contribution to health must be more considered, which is also not always the case, even by social workers themselves. 10
Care coordination programs or interventions are highly dependent on the trajectories of care considered by the policymakers. They are also highly dependent on the nature of the target population and the national and regional history of the service organization. 29 Nevertheless, the National Association of social workers (NASW), 9 a US-based organization, advocates that the contributions of social workers working as case managers “shall participate in ongoing, formal evaluation of her or his practice to advance client well-being, assess the appropriateness and effectiveness of services and supports, ensure competence, and improve practice.”
The Agency For Healthcare Research and Quality identified several terms that are sometimes used interchangeably to name coordination of care, for instance, collaborative care, disease management, case management, care management, chronic care model, and care or patient navigation. 30 This abundant literature regarding all those appellations reflected there is some ambiguity and little consensus around a conceptual model and in the definitions of care coordination. 31 This heterogeneity raises a challenge in synthesizing the knowledge about care coordination.
In primary healthcare, care coordination activities are carried out by different categories of professionals. 11 Although care coordination is part of the social workers’ activities, primary healthcare is still an underrepresented sector in the social work literature for primary care. Due to the limited number of studies on this theme in the field of social work, a lack of knowledge persists about care coordination activities provided by social workers for patients with complex health and social care needs in primary healthcare. As social workers are increasingly present in primary healthcare, this scoping review focuses on charting specific disciplinary aspects of care coordination activities of these professionals for these organizations. A comprehensive understanding of the social workers’ activities and their contribution to care coordination in this context could help align their work with that of other professionals when patients with complex needs are involved.
This scoping review aims to provide a synthesis of the existent literature on social workers’ coordination activities for patients with complex needs in primary healthcare. If we aim at developing a comprehensive social work coordination intervention for a complex need population, which activities should be included? This synthesis attempts to answer this question by answering these specific questions: 1) Who are the targeted complex patient populations? 2) In which organizational context do the care coordination interventions take place? 3) What activities do they involve? and 4) What care coordination interventions are currently enacted by social workers in primary healthcare?
Methods
This scoping review followed standard five steps which are: 1) formulating a research question, 2) identifying and 3) selecting relevant studies, 4) charting the data of the selected studies, and 5) analyzing, collating, summarizing, and interpreting the data. 32 The questions for this review have been presented previously. The search strategy was carried out across multiple databases: CINAHL, Medline, Scopus, SocioIndex, Social Work Abstracts, and ProQuest (dissertation and thesis). The terms used for the search strategy and criteria are presented in Table 1.
Terms for the search strategy and inclusion and exclusion criteria.
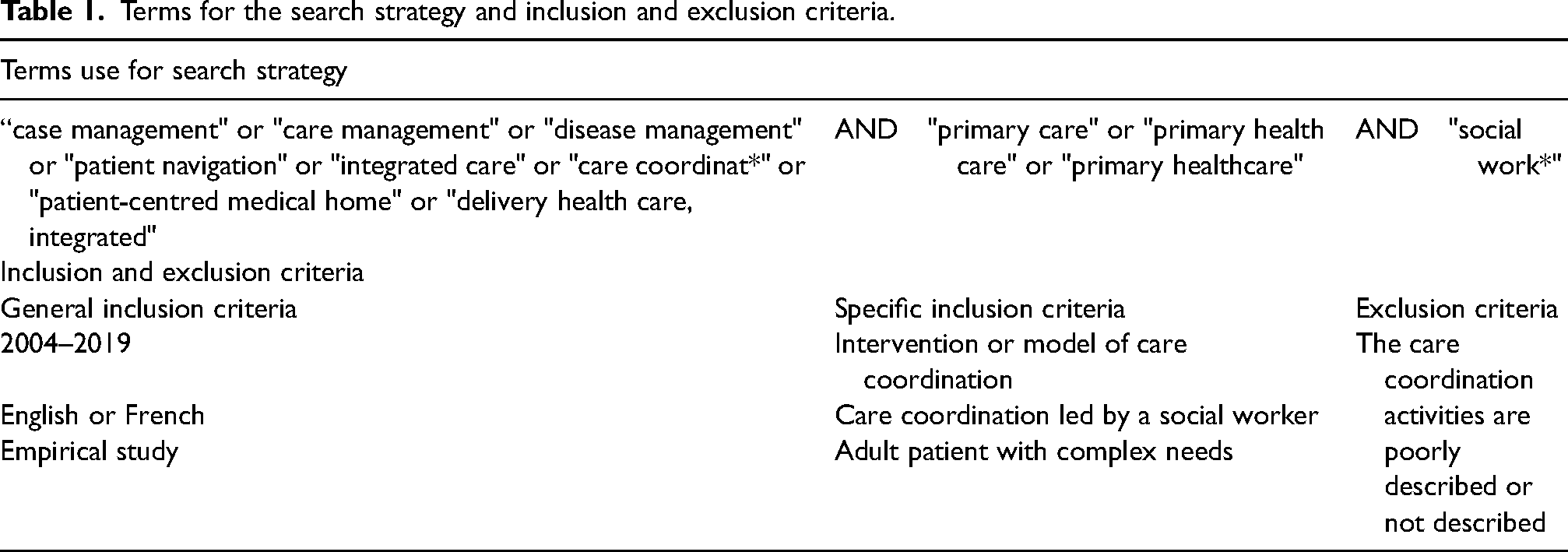
The search strategy was conducted to cover articles from 2004 to 2020, written in English or French. Included articles present an empirical study describing the coordination of care among adult patients with complex needs in the primary care setting. The reported intervention was to be led by a social worker. Later in the search, articles reporting on an intervention led by a team including a social worker and a nurse with equal responsibilities were also kept for review. Articles that did not describe, or described poorly, the care coordination activities were excluded since their content could not meet this scoping review purpose.
Study selection and validation of the selected studies were conducted by two independent researchers through consensus-based discussion (SL & MG). The selected studies were then presented to the research team for further validation. The selection process is presented in Figure 1.
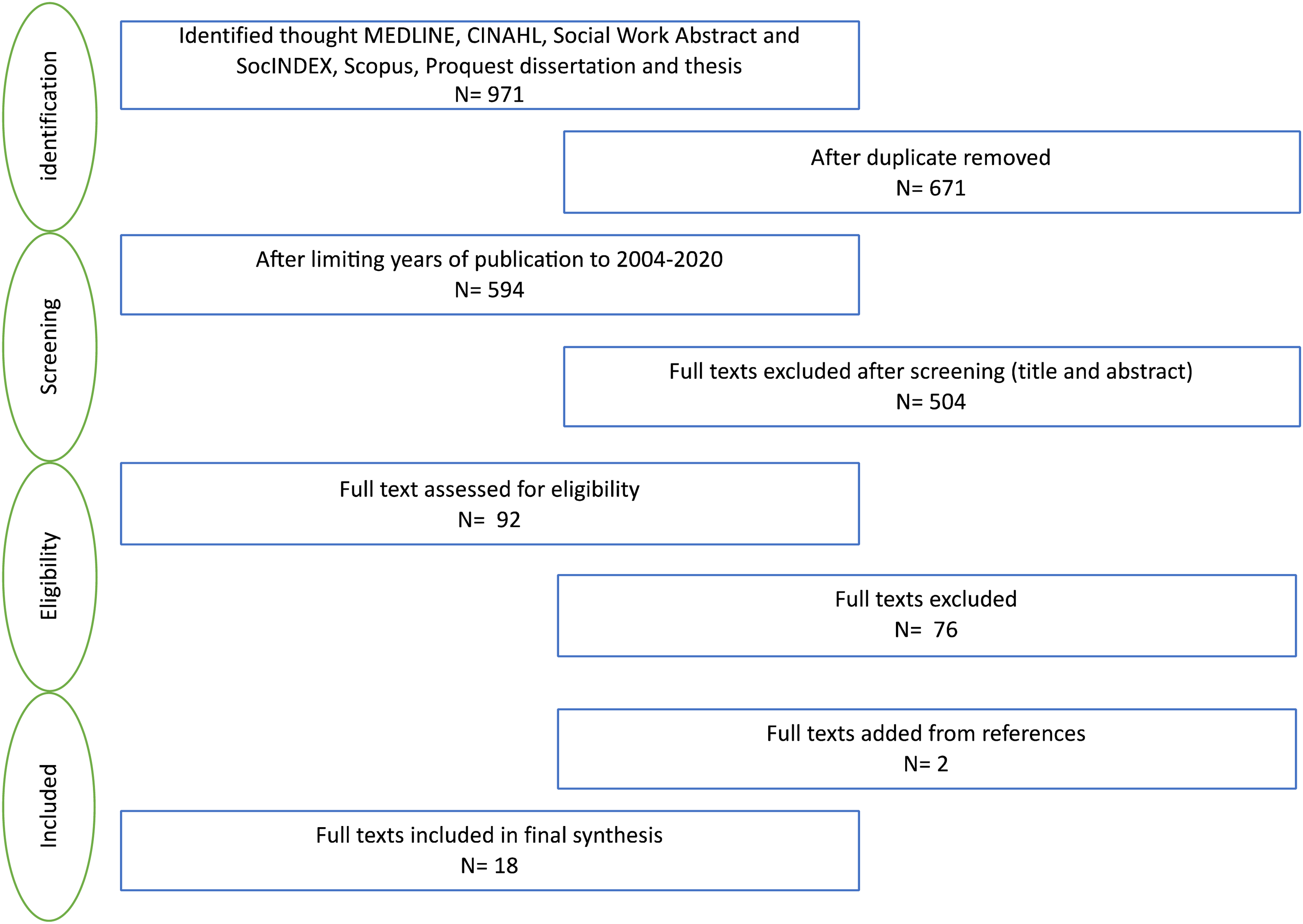
Flow diagram detailing search and studies selection process.
Once the studies were selected, data extraction was accomplished by completing detailed analysis grids that reported the main characteristics of each study and the data required to answer the research questions. This process identified two supplemental studies that had not been identified by the initial literature search. These studies were added to the scoping review. The grids included specific data to describe each study: the study design, objectives, care coordination intervention, target population, and context. The grids also listed all care coordination activities reported in the articles (appellations and definitions). These grids were completed by one of the reviewers (SL) and further validated by a second reviewer (MG). Discrepancies were resolved by discussion between the two reviewers and the main researcher. As the purpose of this scoping review was to describe care coordination interventions and activities, a methodological quality appraisal was not performed.
The descriptive data were compiled to provide a portrait of the context and the population targeted by the care coordination interventions. Then a thematic analysis, using deductive and inductive approaches, was performed with the care coordination activities. First, using a deductive approach, this analysis considered the previous categorization of activity types made by Karam et al. 11 for nursing care coordination activities which were based on the American Nurses Association 33 framework and adapted for primary care and complex patient populations. Even though this categorization was developed for a different domain, the general activity categorization of primary care coordination seems similar to social work activities. Then, using an inductive approach, the analysis considers space to identify emergent subcategories for specific social work activities.
Results
As shown in Figure 1, 92 full-text articles were assessed for eligibility. Eighteen articles met all the criteria and were included in the final synthesis. The 18 studies included reported on 11 different care coordination interventions. For the analyses of care coordination activities, precautions were taken not to duplicate information. The content of each article was used to complete the information on the intervention. Table 2 describes all included studies.
Included studies that address social worker care coordination for patients with complex needs.
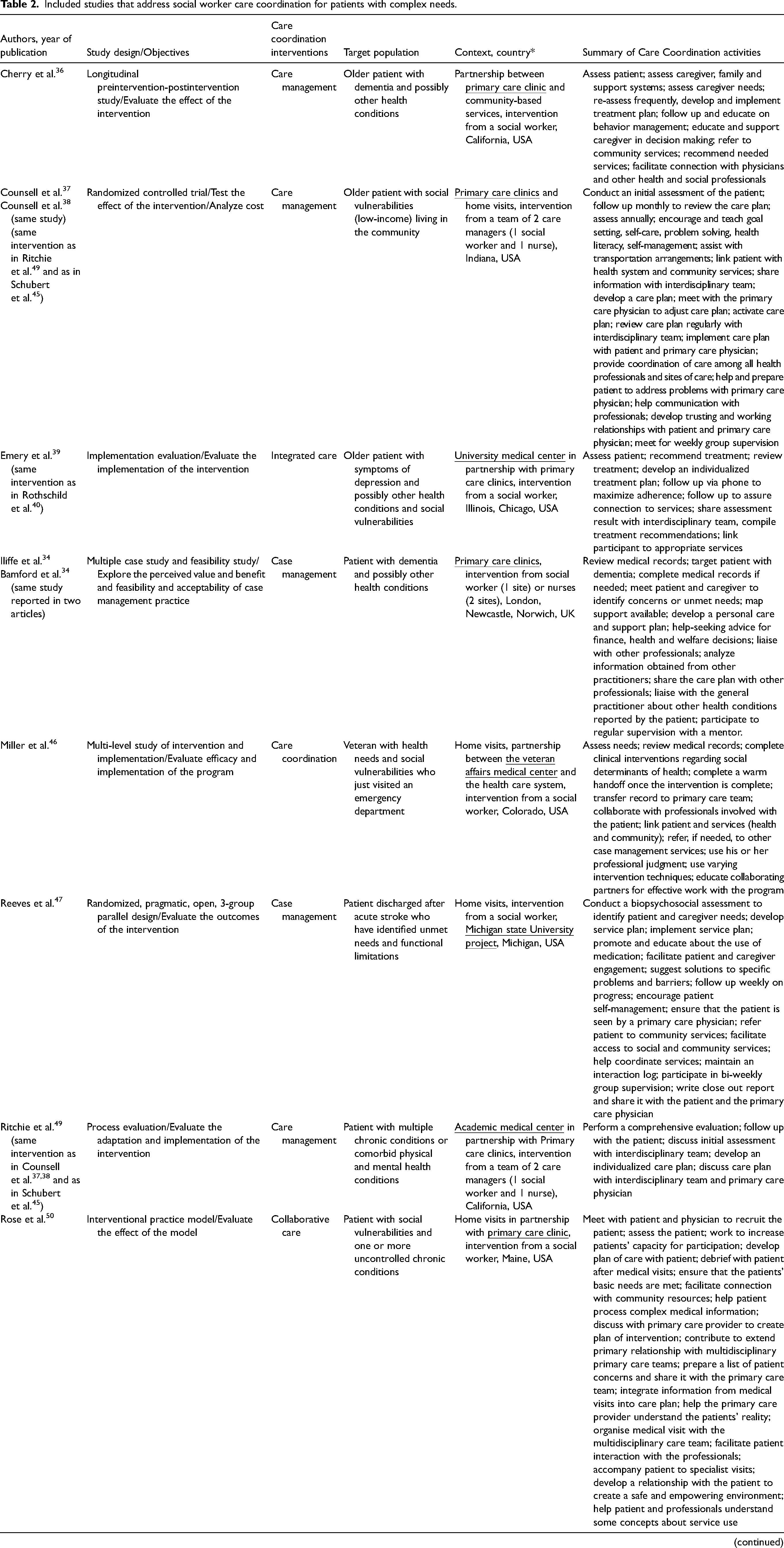
Underlined organizations indicate where the care coordinators are located.
Complex target patient populations
Diverse populations were targeted by the interventions described in the 18 studies. These patient populations are mostly characterized by social vulnerabilities (e.g., low income, uninsured, living alone, housing or employment insecurity, etc.) combined with multiple health needs (e.g., multiple chronic diseases, depression, dementia, stroke, etc.). The majority of interventions (12/18 articles) targeted older patient34–45 with different health conditions. The population's age is not specified in three of the articles46–48 and other care coordination interventions are not age specific.49–51
Organizational context of the care coordination
The care coordination interventions presented in the articles were carried out through different organizations. The majority of interventions involve primary care clinics,34–46,49,50 however, as shown in Table 2 (underline organizations), these clinics are not always the care coordinator's home organization. Other organizations involved in the interventions are academic or university medical clinics,39–43,47,49,51 the department of Veteran Affairs (USA),45,46 hospitals, 48 community-based organization, 36 and one intervention seem to be provided by an independent organization. 51 Several articles (12/18 articles) report on an intervention that involved a partnership between two different organizations.
The majority of articles reported intervention led exclusively by a social worker (10/18 articles).36,39–43,46,47,50,51 In addition, articles reported on two different interventions where care coordination was led interchangeably by a social worker or nurse, regardless of the role or activities of these professionals.34,34,44 It is to be noted that those two interventions are the only ones from outside of the United States. Lastly, since we expanded the criteria to include studies reporting on interventions involving a team of care coordinators, five articles report on two different interventions where a team of one nurse and one social worker work together to coordinate care.37,38,45,48,49 Even though parts of the assessment of the patient are reported as specific to the social worker or the nurse, all other activities are not specific to one professional.
Care coordination activities
Considering in this analysis that some interventions are reported in more than one study, the care coordination activities were synthesized into four categories as presented by Karam et al. 11 In the following, we briefly present the four categories and related activities. A more detailed description and content specifications are provided in Appendix A.
Activities that target the patient, family, and caregivers
Target and recruit patients who will benefit most from the intervention. The care coordinator identifies patients with complex needs by reviewing records or with the help of referring general practitioners and partners.34,35,46 The care coordinator introduces the intervention and makes sure he or she is interested in participating.41–43,45,50
Assess patient, family and caregivers. The care coordinator conducts a comprehensive biopsychosocial assessment of the patient36,38–43,45–50 and an assessment of the patient, family and caregivers’ needs,34,35,42,43,48 readiness to engage in the treatment plan, 48 and decision-making process. 36 The care coordinator conducts an initial comprehensive and transdisciplinary assessment of needs and formal or informal follow-up assessment throughout the intervention duration. This initial assessment is supported by disciplinary assessments, including those of the physician or nurse, and provides additional information for patient care coordination.
Develop, present, discuss, and assist in implementing a tailored care plan. The care coordinator develops the care plan in collaboration with the patient34,34,39–43,47,48,50 and shares and discusses the care plan with the patient.36,39,40,44 The care coordinator also assists in implementing the care plan.
Monitor and follow up on the patient and the care plan implementation. The care coordinator maintains contact with the patient to monitor implementation of the plan, progress, adherence, service use, etc.36,37,39–45,47–49
Offers support and psychosocial intervention to the patient, family, and caregivers. The care coordinator, when relevant, offers support and specific psychosocial intervention to help the patient, family, and caregivers meet their needs. Support and psychosocial intervention mainly aim to answer needs related to the social determinants of health,46–48,50,51 to ensure empowerment of the patient, family, and caregivers,36,41–43,46–48,50 and help in understanding and managing behavioral problems. 36
Activities that target health and social care professionals and services
Share and receive information about the patient, the assessment, or the treatment recommendations. The care coordinator is active in various exchanges of information with other professionals involved with the patient. Information sharing aims to support assessment,37,39,40,49,50 to coordinate recommendations of treatment plan provided by an interdisciplinary or multidisciplinary team,34,35,39,45,46,50,51 or to communicate or discuss patient's needs to service providers.34,35,42,47,50 The care coordinator also sometimes provides logistic support to team meetings,44,50 promote the care coordination intervention,46,50 help provider's understanding of concepts of care coordination, 50 and link professionals together. 40
Develop the patient's care plan or share the patient's care plan with the professionals involved. The care coordinator often develops the care plan with the patient (see category above), but often he or she develops the care plan with a team of professionals38,45,49 or both the patient and a team.34,35,50 This team is also responsible to follow up on implementation and adapt the care plan to answer emerging or changing patient's needs.
Activities that link the patient and family with health and social care professionals and services
Link the patient or provide referrals to health and social services. The care coordinator assists in identifying or recommending relevant resources and services34–36,48 and refer, link, facilitate access, or assure connection to services.39–43,46–48,50 These referrals can be within health services, specific to social services, and across multiple public or community-based sectors such as school, work, and housing.
Coordinate services and support interactions between patient, caregiver, family, and providers. The care coordination sometimes directly assists in coordinating services (scheduling, brokering, engagement of resources, follow-up with providers).34,35,41–43,45,47,48,51 In some interventions, the care coordinator also coordinates actions between professionals to provide services or implement the care plan.37,47,48 They also in some cases assist during medical visits and appointments during which, if needed, they facilitate interactions with the professional and advocate for the patient.36,48,50,51
Cross-cutting activities that support and enhance other activity
Build a relationship with the patient, caregiver, and professionals. The care coordination uses different strategies to ensure he or she develops a relational connection with every person involved which contributes to the efficacy of the intervention.37,41–43,45,48,50
Participate in professional supervision and continuous education. The care coordinator takes part in activities to support the quality of care coordination, the implementation of the intervention of care, professional disciplinary development, and interdisciplinary team development.34,35,37,40,47
Discussion
Our results showed a variety of interventions, led by social workers, in primary healthcare settings and used to coordinate care around patients with complex needs. This heterogeneity confirms that coordination of care means different things to different people in different healthcare systems, depending on locations, targeted populations, and the intervention's objectives. 52 This variety also depends on the diversity of the characteristics of the clients with whom they work and on the quality of their integration into primary health care organizations.
The terms and concepts used to identify the care coordination intervention (care management, case management, care coordination, integrated care, collaborative care) do not appear to define the content of the intervention or the activities of the care coordinator. They seem to vary within the same kind of intervention type as well as multiple similarities can be noted between different appellations of care coordination intervention. For example, studies that identify with care coordination all have activities related to the systematic linkage of the patient with community resources, but only one study 46 presents activities regarding the medical record of the patient (reviewing, completing, and transferring), which are also activities reported in studies using the term “case management”.34,35 Moreover, three studies reporting on the same intervention41–43 do not use the same terms to identify the care coordination intervention. Two of them use care coordination41,42 and one uses care management. 43 As reflected previously in the introduction, terms used to designate care coordination intervention vary and these different terms might need further clarifications. Yet the term case (as in case work) has a historical audience in this discipline. This probably shows how the idea of coordination came back into the world of social work via the world of health.
Single care coordination activities do not seem associated with the target populations. Interventions targeting the same kind of population have similar activities as well as activities that are different. For example, in articles reporting on interventions targeting older patients, not all interventions conduct an assessment (articles that do not report conducting an assessment in the care coordination activities),34,35,44 but all have activities related to the development and implementation of a care plan. In addition, when comparing different population types, it is also noted that activities are sometimes similar, sometimes different. For example, the same intervention is studied in four articles, three targeting older patient37,38,45 and one targeting none age-specific patients (Ritchie et al., 2016). 49 Therefore, care coordination activities do not seem to depend on the target population but are more related to the intervention itself.
Observations are similar when considering the organizational context in which the care coordination activities take place. No specific activities seem related to the localization of the care coordinator. The involvement of a partnership in the project versus the initiative of a single organization also does not appear to determine the nature of the care coordinator's activities. It also seems that there are no significant differences in the care coordination whether it is led by a social worker, a nurse, or a bidisciplinary team.
The interventions are what seem to influence the most the care coordination activities. Unfortunately, the articles included in this review rarely specify or specify with too few details, the rationales behind the choice of the included care coordination activities. Therefore, it is harder to discuss the specific similarities and differences between interventions. Still, similarities between interventions are frequent. Some activities appear less often than others, but no activity is associated with only one intervention. For example, Assess patient, family and caregivers appears in 15 of the 18 articles while participate in professional supervision and continuous education appears in five of the 18 articles.
Many of the reported activities may be perceived by social workers and researchers as disciplinary. However, they are often shared with colleagues from other disciplines, such as nurses, forming a common core of transdisciplinary coordination activities. Moreover, as shown in the introduction, the definition of the contribution of social work to coordination in primary health care is young and still being defined. Case management seems characteristic of social work and most times is undifferentiated from standard social work practice, which can be illustrated by the frequent use of the term “case work” to define their practice. It is a professional function mainly dedicated to the multidimensional evaluation of the needs of people with complex problems, to the planning of all the multidisciplinary interventions that result from it, and then to their coordination over a long period, regardless of the territory under the responsibility of the organizations involved in the overall response to the user's needs. 53 Therefore, care coordination also concerns patients with complex needs that go beyond the medical response. It is the professional component of service integration at the core of reforms in the organization of health and social services for clients with complex clinical situations. 54
This scoping review proposes many essential components of care coordination that should be found in interventions for patients with complex needs. Assess patient, family, and caregivers seem inevitable in healthcare interventions and even though it is an important activity that guides the entire intervention, it is not specific to care coordination. More specific to care coordination is activities related to share and receive information about the patient, the assessment, or the treatment recommendations. Collaboration based on interprofessional and sharable records with the general practitioner seems to be the foundation of every activity involving social workers working with patients with complex needs. The exchange of information between the people involved in the different components of care is recognized as an effective strategy for the organization of care.55,56 Collaboration is encouraged by the World Health Organization 57 and has become a priority for healthcare systems over the past decade. Other studies have stressed the importance of communication based on good working relationships between professionals to respond to the complex needs of patients.52,58–62
The care coordinator's action must therefore deal with an interprofessional function focused on the organization and coordination of services 63 and a disciplinary professional function focused entirely on the relationship with the patient. 64 At the junction of those two functions lies a specifically well-known action of case management: advocacy 65 which is the action of supporting the patient in an always more complex system. In this way, care coordinators manage to establish a relationship of trust with their patients, advocate on their behalf and make themselves available which are two other essential categories of activities (Coordinate services and support interactions between patient, caregiver, family, and providers and Build a therapeutic relationship with the patient, caregiver, and professionals).
Also, Link the patient or provide referrals to health and social services is of great value in care coordination. Various coordination models share some common goals, including facilitating access to social resources, 66 and increasing interorganization services coordination, 67 one of the traditional functions of social work. 68 Home visits, as well as the involvement of community resources, seem of particular importance when coordinating the care of patients with complex needs. This is largely in response to the vulnerability and some cases functional decline of the target patient populations. 69 Creating a relational continuity of care with the patient and family, and relevant members of the community emerge as central to the coordination of care with complex needs populations. For these patients, integrated care means a single point of entry and privileged contact with a dedicated care coordinator. 62
This scoping review has several implications for future research, policy, education, and practice. We have shown that the success or failure of integrated care interventions, including care coordination,70,71 depends on the context and the quality of their implementation. 6 It is generally recognized that complex interventions frequently encounter obstacles in their implementation. 44 However, the studies included in our review present little, or no information related to the quality or fidelity of interventions. There is also no clear indicator of the frequency of social workers’ activities, nor of their need to develop skills or competencies for certain activities that are atypical to their field. It would be interesting to explore these factors further to explain, at least in part, the limited effectiveness of some interventions.
The extent and purpose of coordination depend in part on the coordinator's area of practice. The scope of social work is characterized by linkages with nonmedical services, including life skills support, community resources, and nonhealth intervention areas (school, work, housing, etc.). Social workers share a care coordination contribution with families and caregivers with nurse care coordinators. Interprofessional coordination between these two disciplines remains to be better understood.
From a policy perspective, our results highlight the following challenge for health care systems: to identify employment and remuneration models for primary health care that would facilitate multidisciplinary teamwork and promote collaborative rather than hierarchical practice. This involves facilitating the transfer of information between providers through effective communication technologies, and the integration of social work in the information tools used by physicians, otherwise, the two parallel modes will continue, on a disciplinary level, but also in care coordination activities.
At the organizational level, our review highlights the need for coordinating social workers to have a clear role and to “meta-coordinate” with all professionals in and around primary health care involved in the patient's care. In addition, they must be supported by the health care system through funding, clinical and communication tools, and other means. Especially in certain contexts where social workers intervene on two levels, the one belonging to their discipline and the one involving their coordination activities. This is particularly difficult when their place in primary care organizations is uncertain.
Finally, some interventions in our review necessitated preimplementation training for social workers. Though we cannot confirm that it is the case in other countries, in Québec, care coordination, and primary care, are not present in social work education even though activities of coordination seem to be a crucial part of social work history. This synthesis provides a foundation for the development of specific professional competencies that would target the skills needed for effective coordination and improve care coordination interventions. It also supports the need to develop systematic documentation of care coordination activities of social workers to secure appropriate financial and societal recognition of their contribution to high-quality integrated care.
Research that describes the intensity of care coordination services for different populations is still needed. 52 In medical clinics, there are three coordinators, the doctor who coordinates with specialists, the nurses who coordinate some nursing interventions, and the social workers for services to support functional capacity, family mobilization, intersectoral coordination, etc. From pair to pair (doctor–nurse, nurse–social worker), the coordination overlaps. The articulation of these coordinations and their effects are still to be understood.
This scoping review has several strengths and limitations. To our knowledge, there are currently no other reviews to synthesize social worker care coordination activities for patients with complex needs in primary health care settings. Findings could contribute to the development of a framework for care coordination and opens the door to several future research projects.
The review used only parts describing the processes of care coordination and the specific activities of care coordinators as provided in the included studies. Therefore, aspects such as system-level mechanisms, structural aspects that support care coordination and the organization of primary care in each country were not addressed. For example, this article does not consider the diversity of primary care between countries and their influence on the practice of social workers. More studies should be conducted on this topic.
Also, descriptions were sometimes poor or lacking details, so we may have missed specific features of some activities. To minimize missing information, we reviewed the available theoretical articles presenting the interventions studied in the included empirical articles.
In conclusion, despite the heterogeneity of care coordination interventions, one common thread remains: they aim to reduce the fragmentation of care by bridging the gaps between the patient needs and the system capacity. Social workers, because of their disciplinary skills, can make a significant contribution to care coordination in primary health care, in collaboration with nurses. This interprofessional collaboration is common in practice but is rarely supported by training that meets the need of professionals. The practical and conceptual heterogeneity shows that further attention needs to be given to the education and training of social workers to enable them to act effectively in care coordination and team-based care delivery. The integration of essential and transversal skills into the training program for social workers would optimize the coordination of care.
This same heterogeneity illustrates the diversity of needs that care coordination aim to meet. Behind this observation lies the narrow information provided about the implementation of a care coordination intervention, insufficient by itself to foster strongly integrated care and meet the needs of targeted patients. Challenges remain and care coordination interventions should be linked to a continuum of strategies at all levels to achieve effective and efficient care. 72 Finally, the intersectoral part of coordination of care, around the primary health care setting, closely concerns social workers.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Care Coordination activities and their description. Target patients with complex health and social needs Introduce the program to the patient and ensure the patient's understanding of the program and the need for care coordination Make sure the patient is interested in participating Reviewing medical records or GP lists (assess for program eligibility) Referral from the GP or other program's partners (hospital, primary care clinic, etc.) Conduct a comprehensive biopsychosocial assessment of the patient
○ Conduct by phone, in a clinic setting or home visit ○ Conduct follow-up assessments as needed or depending on the program's procedures ○ Use validated and standardized tools and protocols ○ Use various counseling strategies ○ Discuss the assessment's outcomes with the patient Patient's history (medical history, personal history, social history) Physical health (general health, vital signs, cardiovascular risk, gait and balance, vision et audition etc.) Mental health (mental and cognitive status, depression, psychotic symptoms, dementia, behavioral problems, etc.) Social determinants of health (social support, home safety, living arrangements and conditions, family interactions, available resources, financial situation, etc.) Functional status (medication management, daily function, feeding, dressing, mobility, etc.) Readiness to engage in the program (motivation, values, readiness for change, barriers, goals, decision-making process, strengths, etc.) Family and caregiver needs Share and review care recommendations with the patient Develop (collaboratively) and review the care plan Assist the patient in implementing the care plan—coordinate the care plan activities Is patient-centered Is individualized Is mutually agreed (with patient and caregivers) Is based on priorities and mutually agreed goals Is evolving Is revised as needed Maintain contact with the patient
○ By phone, home visits or clinic appointments ○ Weekly, monthly, twice per year or as needed (depending on the program) Re-assess the patient (progression or decline) (see Assess patient, family, and caregivers) Assess ongoing implementation (relevance and achievability) of the care plan Assess goal attainment Review or modify the care plan Facilitate adherence to care plan Ensure support is available Ensure services are obtained—address barriers to the use of services Provide further information and resources (if needed) Clinical intervention regarding SDOH to improve health outcomes Practical education on housing, finances, parenting, employment, etc. Identification and removal of barriers (e.g., transportation issues, financial burdens, complexities of multiple providers, etc.) Collaborate to ensure basic needs (e.g., safe and affordable housing, food security, clothing, etc.) Encourage and educate in self-care and self-management Encourage and reinforce goals setting, goal implementation and goal achievement Facilitate decision-making
○ Encourage decision making ○ Educate, give information, and discuss available choices and resources ○ Give relevant information about disease and treatment options Educate and assist in learning problem-solving skills Use behavioral counseling and psychoeducation to reinforce self-efficacy, personal strength, self-focus, and a sense of control Present the assessment results to an interdisciplinary or multidisciplinary team (virtually or in a meeting) Provide information about the patient to the professionals involved Receive information about the patient from the professionals involved Make sure the medical record or the patient's file are up to date, write a close-out report (so that the information is shared with the professionals involved) Discuss the patient's case with the interdisciplinary team and the primary care provider Prepare a list of the patient's concerns and needs to present them to the professionals involved to prepare for the patient's visit Compile recommendations Coordinate recommendations of multiple care providers Integrate suggestions into the care plan Analyze and synthesize information (from assessment, medical records, providers, etc.) Complete medical records if needed Plan and organize the interdisciplinary or multidisciplinary team meeting Promote the program or provide education about care coordination and the program to professionals and service providers Help providers’ understanding of concepts Link professionals (health services and community-based services) together to help coordinate services between other providers and the patient primary care provider (physician) Develop an individualized care plan for the patient
○ Based on assessment results, interdisciplinary team suggestions, and protocols Review care plan with the interdisciplinary team (regular team meetings) Adapt the care plan with the primary care provider (present, review, modify, prioritize) Identify resources (indexing, organizing, mapping) that may provide services to the patient and caregiver Recommend resources to the patient and caregiver Refer the patient and caregiver to services Link the patient and caregiver to services Facilitate connection and access Assure connection to wanted services (if needed and agreed upon) Health services (physical and mental health) Community-based services Neighbourhood resources (formal and informal) Ensure the patient is informed of available services to help achieve care plan goals Assist the patient in seeking needed services Help create a system of support (natural helping network) Directly assist in coordinating services between the patient and providers
○ Support scheduling (set up appointments and visits) ○ Assist with transportation ○ Assist in brokering services, obtaining services ○ Ensure resources are in place and engaged (ongoing care) ○ Ensure follow-up with providers Coordinate actions of all professionals involved in implementing the patient's care plan Help to navigate the health system Assist during medical visits (clinic or home visits) and appointments with other providers
○ Facilitate interaction and communication ○ Support patient in presenting concerns and needs ○ Provide emotional support ○ Advocate for patient ○ Assist with paperwork ○ Model appropriate behaviors Develop a relational connection based on:
○ Trust ○ Collaborative working ○ Creating a safe and empowering environment ○ Empathy ○ Positive interpersonal interactions ○ Active listening Participate in a supervision meeting
○ In group or individually ○ Regularly (weekly or bi-weekly) Undertake training and continuous education
○ Specific training, co-development, professional updating (as needed) Support professional development Support quality of care coordination (improvement of care) Help and support implementation of the program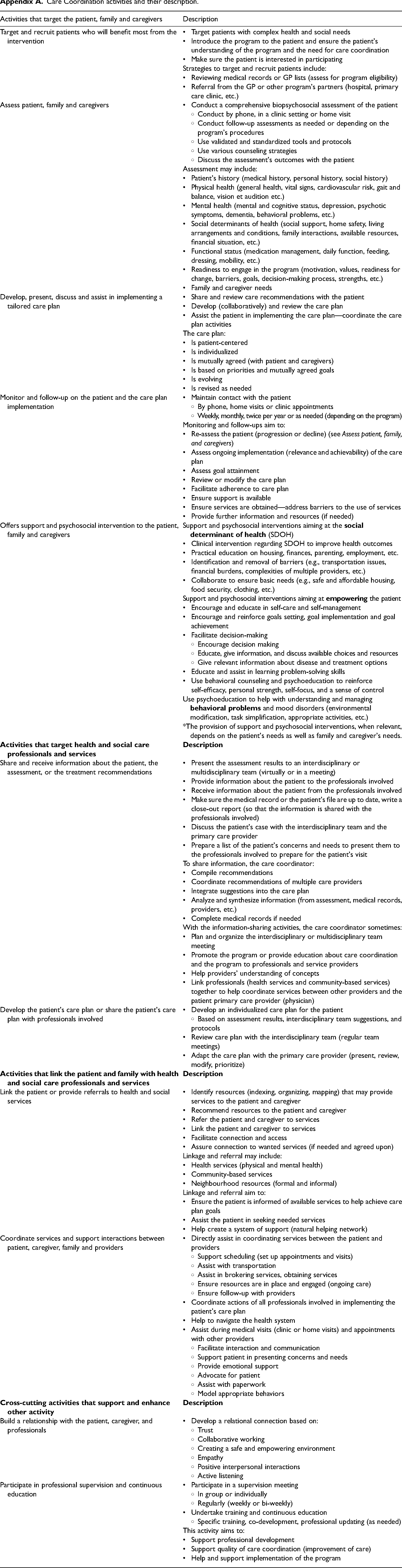
Activities that target the patient, family and caregivers
Description
Target and recruit patients who will benefit most from the intervention
Strategies to target and recruit patients include:
Assess patient, family and caregivers
Assessment may include:
Develop, present, discuss and assist in implementing a tailored care plan
The care plan:
Monitor and follow-up on the patient and the care plan implementation
Monitoring and follow-ups aim to:
Offers support and psychosocial intervention to the patient, family and caregivers
Support and psychosocial interventions aiming at the
Support and psychosocial interventions aiming at
Use psychoeducation to help with understanding and managing
*The provision of support and psychosocial interventions, when relevant, depends on the patient's needs as well as family and caregiver's needs.
Share and receive information about the patient, the assessment, or the treatment recommendations
To share information, the care coordinator:
With the information-sharing activities, the care coordinator sometimes:
Develop the patient's care plan or share the patient's care plan with professionals involved
Link the patient or provide referrals to health and social services
Linkage and referral may include:
Linkage and referral aim to:
Coordinate services and support interactions between patient, caregiver, family and providers
Build a relationship with the patient, caregiver, and professionals
Participate in professional supervision and continuous education
This activity aims to: