
Abstract
Introduction
Continuity of care by family physicians in primary care settings may play a role in reducing health resource utilization and improving clinical outcomes and satisfaction of patients with chronic obstructive pulmonary disease. Clear evidence on the impact of continuity of care will support clinical programing and integration of services across health settings.
Methods
The association between continuity of care and unplanned health service utilization in persons with a diagnosis of chronic obstructive pulmonary disease in a rural region in Ontario, Canada was evaluated. A retrospective cohort study was conducted using population-level health administrative data. The main exposure variable was continuity of care.
Results
A continuity of care index was calculated for patients with at least five visits to a healthcare provider during the 5-year follow-up period (n = 40,033). Higher continuity of care (n = 20,008) and lower continuity of care (n = 20,025), based on the median continuity of care score were calculated. Patients with lower continuity of care had an increased adjusted relative risk of 2.12 (2.08, 2.33) of an emergency department visit, 2.81 (2.72, 2.9) risk of hospitalization, and 3.52 (3.24, 3.82) of being readmitted to hospital compared to those with higher continuity of care.
Discussion
An association between continuity of care and unplanned health services utilization, where a lower use of unplanned health services was observed in the cohort of patients with chronic obstructive pulmonary disease experiencing higher continuity of care. Continuity of care makes philosophical and social sense in that care is provided by a known provider to a known patient and unnecessary investigations can be avoided.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is a chronic lung disease characterized by ongoing airflow limitation with respiratory symptoms. COPD is common, preventable, and treatable. Known causes include sustained exposure to noxious gases, such as cigaret smoke 1 and environmental pollutants. The international organization Global Initiative for Chronic Obstructive Lung Disease estimates the prevalence worldwide at over 6%, while the Canadian Chronic Disease Surveillance System (CCDSS) reported a prevalence of 9.4% in the population of adults over the age of 35 in 2011–2012. 2 COPD contributes to the highest rates of hospital admissions among major chronic illnesses 3 and to the death of approximately 3 million people globally. 1 The Canadian Chronic Disease Surveillance System 2 reported the age standardized all-cause mortality rates in 2011–2012 was 22.2 per 1000 for those with COPD compared to 8.2 per 1000 for those without COPD in Canada.
Effective COPD management aims to prevent disease progression, relieve symptoms, improve exercise tolerance and health status, as well as prevent and treat complications and exacerbations. 3 This is achieved through proper assessment and monitoring of the disease, reduction of risk factors, and management of a stable COPD as well as exacerbations. 3 Care for patients with COPD is provided in large part by family physicians in the primary care setting and by specialists, with patients receiving the most appropriate level of care from this team of providers. 4
Despite advances in medical care and implementation of national disease management guidelines, barriers such as geographic distance, specialist access, and poor care coordination influence the provision of care and leads to differences in outcomes for this population of patients. 5
Patients with chronic illnesses benefit from consistent care by the same care provider or team of providers in primary care. 6 Even with known treatments, the progressive nature of chronic illnesses necessitates a continuous and coordinated care approach. Care coordination has been extensively studied, as it a crucial element of and support for patient-centered quality care. While definitions of care coordination vary between studies, a review of literature by Schultz & McDonald identified five important themes that describe care coordination: “care coordination (1) involves numerous participants, (2) is necessitated by interdependence among participants and activities, (3) requires knowledge of others’ roles and resources, (4) relies on information exchange, and (5) aims to facilitate appropriate healthcare delivery. 7 ” When implemented within and across health settings, care coordination supports seamless interactions between providers across multiple settings, and therefore facilitates continuity of care.
Continuity of care, especially in the context of primary care, is characterized as care over time with a particular patient that is consistent, patient focused, and encompasses both health and illness.8–11 In the context of chronic disease management though, continuity of care can be “seen as the delivery of services by different providers in a coherent, logical, and timely fashion.”8,12,13 In this study using administrative data, continuity of care was measured using the Bice-Boxerman's Concentration of Care Index (COC) 14 that captured the care across different providers as well as the care coordination back to the family physician. 15 This index was shown to accurately measure the dispersion and concentration of care in similar studies. 15
Continuity of care is a key component of quality health care. A comprehensive systematic review of literature of 22 studies concluded that an increase in continuity of care by doctors was associated with lower mortality rates. 16 This observation was also reported by Maarsingh et al. in a robust 17-year prospective study in the Netherlands, where mortality was increased by 20% for those with the lowest level of continuity of care compared to those with the highest level. 17 Continuity of care by family physicians is associated with a lower number of hospital admissions for ambulatory care sensitive conditions and this effect was stronger for patients who were considered heavy users of primary care. 3 Continuity of care has also been associated with lower hospitalization with those who have diabetes.18,19As such, poor (or lack of) continuity of care often translates into higher unplanned health services utilization in the acute care setting (admissions and readmissions), with added costs to the health system and to the patient's quality of life. 20
Therefore, the overall goal of this study was to determine the association between COC and unplanned health service utilization in persons with a diagnosis of COPD. Focus of the study was on one region in southeastern Ontario (Local Health Integration Network) as there was concern raised by regional health system planners about high emergency use and hospitalization rates for patients with COPD. Information was needed to inform the planning of regional health services.
Methods
This population-based retrospective cohort was conducted using de-identified Ontario administrative datasets held by ICES. Ontario represents over 38% of Canada's population, with 13.45 million Ontarians on May 10, 2016. 21 In Ontario, COPD prevalence has increased steadily in past years to reach 9.5% in 2007 (male and females combined; all age groups combined), with females bearing the largest increase. 22
This study focused on the South East Local Health Integration Network (LHIN) region, which includes the sub-regions of Quinte, Rural Hastings, Rural Frontenac, Lennox & Addington, Kingston, and Lanark, and Leeds & Grenville. The South East LHIN is home to approximately 496,400 people, or 3.6% of the Ontario population. 23 Forty-five percent of the population lives in a rural area and a quarter of the population in a large urban center. 23 The South East LHIN has the highest proportion of seniors in Ontario, with 21% of residents of the South East LHIN aged >65 years. Relative to the province, the South East LHIN has a lower rate of population growth now and projected over the next 20 years, 24 a lower proportion of immigrants (8.5% vs 28.5% in Ontario), and a lower proportion of visible minorities (3% vs 26% in Ontario). In comparison to Ontario, the South East LHIN has a higher prevalence of people who are overweight or obese and reporting activity limitations. 23
The cohort included all patients residing within the South East LHIN region with a diagnosis of COPD as of April 1, 2013. Individuals meeting the following criteria were included in the study cohort: 1) age 35 to 99 years and living in Ontario; 2) diagnosed with COPD on or prior to April 1, 2013; 3) residing within the South East Local Health Integration Network region; 4) valid Ontario health card number for the duration of the 5-year follow-up period; and 5) at least one health care interaction (emergency department visit, hospitalization or physician visit) during the 5-year follow-up period. Individuals with COPD were identified using a case definition algorithm of 1 or more physician billing claims and/or 1 or more hospital discharges with a diagnosis of COPD as per the following codes: 491, 492, 496 (Ontario Health Insurance Plan and International Classification of Diseases, Ninth Revision codes) 25 or J41, J42, J43, J44 (International Statistical Classification of Diseases, 10th Revision codes). 26 The cohort was then followed for five years (April 1, 2013 to March 31, 2018). Demographic characteristics, socioeconomic status, and comorbidities were determined for descriptive purposes and used as covariates in modeling.
The following databases were linked to provide the required data: Hospital Discharge Abstract Database, National Ambulatory Care Reporting System, ICES-derived COPD cohort, Ontario Health Insurance Plan Claims Database, Ontario Marginalization Index, Postal Code Conversion File, and Registered Persons Database.
COC was calculated using billing codes for any outpatient family physician and specialty (respiratory and internal medicine) visits over the 5-year observation window and excluding participants who had less than 5 visits. As well, analysis was performed to identify the usual provider of care (UPC). The UPC reflects the concentration of care with a single provider or group of providers across time. UPC was measured by using the highest number of visits to a single practitioner or a group of practitioner and then divided by the total number of visits. 27
A cross-tabulations and descriptive statistics for the baseline characteristics of the study cohort was conducted. Dichotomous data is presented as N and percentage; continuous variables are presented as mean with standard deviation.
Generalized linear models were used to estimate the risk ratio between continuity of care and each study outcome (ER visits, hospital admission and readmission).
Standardized differences were calculated and represent the difference in mean outcome between groups divided by the standard deviation of outcome among participants and is considered significant when ≥ 0.1. Standardized differences were used as they better represent differences of clinical relevance when analysing very large datasets.
The full adjusted models included all available variables: age, sex, income quintile, socioeconomic status, material deprivation quintile, rural/urban residence, and comorbidity (major ADGs).
All analyses were conducted using SAS©. 28 This study received ethics clearance from the Queen's University Health Sciences and Affiliated Hospitals Research Ethics Board (NURS-472-19).
Results
Demographic and clinical characteristics of the study cohort
As of 2013, there were 42,916 adults with COPD residing in the South East LHIN. Of those, 40,033 had at least five visits to a healthcare provider and were therefore entered into the cohort for which a continuity of care (COC) index was calculated. Individuals were assigned to the higher or lower continuity of care sub-group based on their individual COC score relative to the median continuity of care index (individual score > median COC for the population = higher COC group). As presented in Table 1, the demographic and clinical characteristics of patients in the lower and higher COC populations were similar for age (M = 66.56, SD = 12.82) for the lower COC vs 65.50 (SD = 12.40) for higher COC, for the proportion of females (52.6% for lower COC vs 55.4% for higher COC), socioeconomic status, and the average time that patients had been diagnosed with COPD prior to the start of the study (M = 9.58 years, SD = 6.54) for the lower COC group vs 9.61 (SD = 6.47) year for the higher COC group). Both groups also had similar proportion of patients with concurrent asthma, diabetes and hypertension. In contrast, the distribution of patients enrolled in the various primary care models and their distribution in relation to the distance to their usual provider of care were different, as was the rate of residential instability (M = 3.50, SD = 1.24 for lower COC vs 3.42 (SD = 1.23) for higher COC group). In addition, the proportion of patients admitted to long-term care during the 5-year study window was statistically significantly different (1.0% for the lower COC vs 4.2% in the higher COC; standardized difference = 0.21), as was the risk of dying during the 5-year study period (26.8% in the lower COC vs 12.6% in the higher COC group; standardized difference = 0.36). Further analyses were performed to better understand the large difference observed in death rate between the two groups (see Table 3).
Demographic and clinical characteristics of the study cohort of adult patients with COPD as of April 1, 2013 and residing within the south east LHIN region and experiencing lower or higher continuity of care (COC).
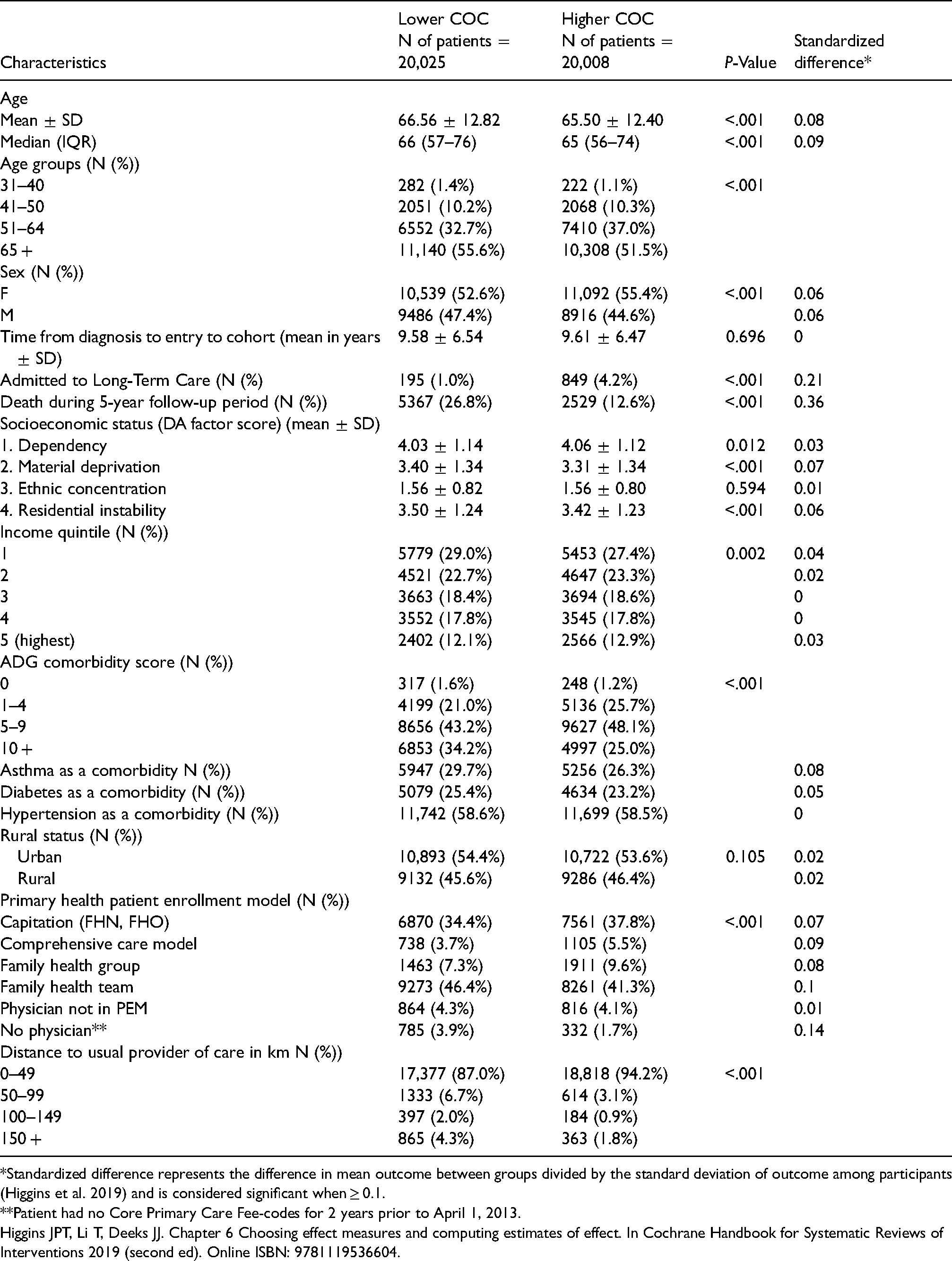
*Standardized difference represents the difference in mean outcome between groups divided by the standard deviation of outcome among participants (Higgins et al. 2019) and is considered significant when ≥ 0.1.
**Patient had no Core Primary Care Fee-codes for 2 years prior to April 1, 2013.
Higgins JPT, Li T, Deeks JJ. Chapter 6 Choosing effect measures and computing estimates of effect. In Cochrane Handbook for Systematic Reviews of Interventions 2019 (second ed). Online ISBN: 9781119536604.
Health services utilization for adults with COPD with lower and higher COC
Statistically significant differences were observed in the measured utilization of healthcare services. As reported in Table 2, patients with lower COC were 2.12 times (95% CI 2.08, 2.16) more likely to visit the emergency department (for any reasons), 2.81 times (95% CI 2.72, 2.9) more likely to be admitted to hospital (for any reason), and 3.52 times (CI 3.24, 3.82) more likely to be readmitted to hospital within 30 days of discharge, compared to those experiencing higher COC.
Relative risk of emergency department (ED) visits, hospital admissions and readmissions for residents of the south east LHIN during the 5-year follow-up period (April 1, 2013–March 31, 2018).
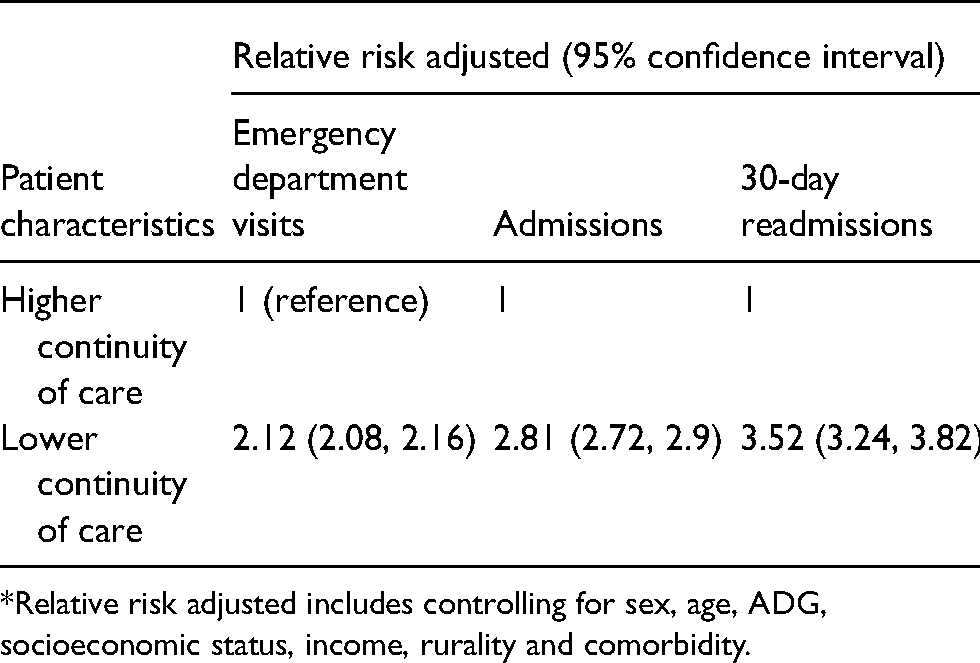
*Relative risk adjusted includes controlling for sex, age, ADG, socioeconomic status, income, rurality and comorbidity.
Study population who died during the 5-year follow-up period (April 1, 2013–March 31, 2018).
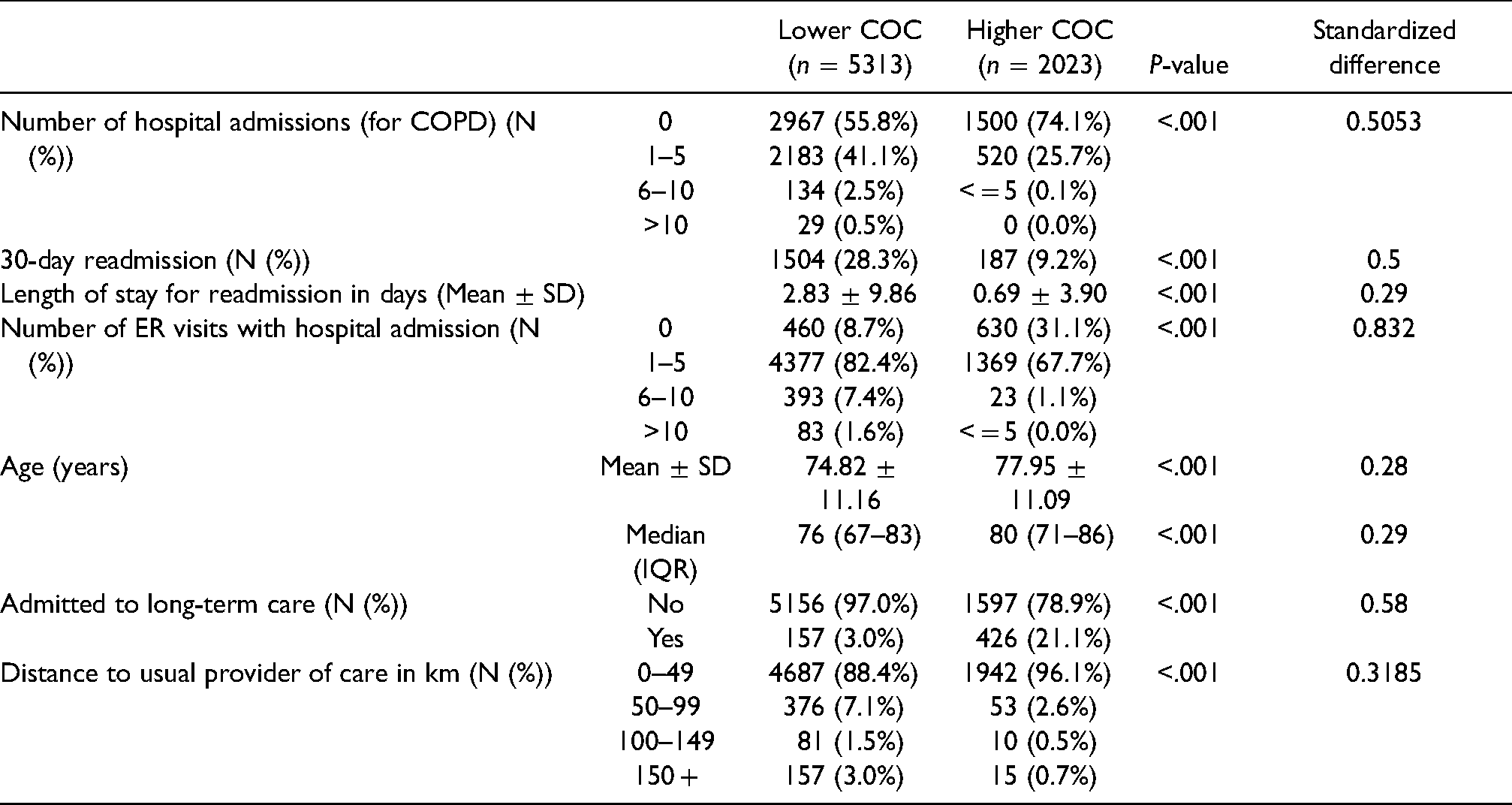
Characteristics of adults with COPD who died during follow-up period
Further to the observation that the death rate of the cohort was statistically different between those who had lower COC compared to higher COC (Table 1), additional analyses were conducted to identify potential differences between the two groups who died [lower COC = 5313 patients, higher COC = 2023 patients] (Table 3). Overall, fewer patients within the lower COC group were never admitted during the 5-year follow-up period (55.8% of patients for the lower COC group were not admitted vs 74.1% of patients in the higher COC group; standardized difference = 0.5053), patients within the lower COC had more ER visits that resulted in hospital admission (8.7% for the lower COC cohort never had to be admitted following an ER visit vs 31.1% of the higher COC cohort; standardized difference = 0.832), and were more often readmitted within 30 days (28.3% for the lower COC group were readmitted within 30 days vs 9.2% of patients in the higher COC cohort; standardized difference = 0.5). The length of stay in hospital for the lower COC was also longer (M = 2.83, SD = 9.86 for lower COC vs 0.69 days (SD = 3.90) for higher COC; standardized difference = 0.29). The distance to the usual provider of care was also longer for patients in the lower COC cohort (88.4% within 50 km of their provider for the lower COC group vs 96.1% for the higher COC group; standardized difference = 0.3185). In contrast, those with lower COC were on average younger (mean 74.82 for patients in the lower COC group vs 77.95 years for patients in the higher COC group; standardized difference = 0.28) and less likely to be admitted to long-term care (3.0% for the lower COC group vs 21.1% for the higher COC group; standardized difference = 0.58).
Discussion
The study was undertaken to understand the potential association between continuity of care experienced by a cohort of patients diagnosed with chronic obstructive pulmonary disease (COPD) and living in the South East Local Health Integration Network (SELHIN) region, and patterns of unplanned health services utilization. As such, the demographic and clinical characteristics of this population, as well as the frequency of ED visits, hospital admissions and readmission within 30 days, admission to long-term care and death were analyzed over a five-year follow-up period. Overall, the patients within the lower and higher COC groups had similar demographic and clinical characteristics, but the patients in the lower COC group were significantly more likely to die during the follow-up period, to require admission to hospital and readmission within 30 days, had longer hospital stays, and were less likely to be admitted to long-term care. Patients in the lower COC group also lived significantly further away from their usual care provider. As the South East Local Health Integration Network region boasts the highest proportion of residents living in rural areas of Ontario who cannot rely on a well-developed public transportation system, a large proportion of the SELHIN patients must have access to a car and/or drive to reach the major community and level 3 hospitals in the southern border along Lake Ontario and the St Lawrence River.
It is important to note that while the mortality rate for those with COPD was calculated to be approximately 20% over a five-year period (combined higher and lower COC groups; study data), higher continuity of care was associated with a lower mortality rate.
Continuity of Care is considered a benchmark of quality especially for those with complex health conditions and is a goal of primary care, as it has been shown to improve patient satisfaction, decrease hospitalizations and reduces health care costs. 29 As such, this study provides much needed population-level data to support integrated teams of health care providers working to meet individual patient needs 30 and will help in planning improved supports for a patient-centric network of care in which providers (and services) collaborate at the community level to deliver comprehensive and seamless care to patients with COPD. This knowledge may also form a strong basis for the development of coordinated care for other chronic conditions.
Additionally, patients with lower continuity of care were more likely to visit the emergency room, be admitted as a result of the visit and subsequently require readmission within 30 days, suggesting a disconnect or poor transition between the acute care setting and subsequent community care, to prevent a further exacerbation of COPD.
Those with lower COC had a higher rate of residential instability compared to patients experiencing higher COC. It could be hypothesized that those who move more often (higher residential instability) may find it more difficult to establish a stable relationship with a new family physician than those who live in the same place for longer periods of time.
It is interesting to note that patients from the higher COC group who died within the 5-year follow-up period were on average older (median difference four years) and more likely to be admitted to LTC, which makes sense in that they lived long enough to become frail and needing 24-h nursing care not available in the home.
Finding from this population-level study support the benefits of providing high continuity of care to patients living with a chronic condition such as COPD, as it reduces the relative risk of unplanned health service utilization (Emergency Department visits, admissions, and readmissions within 30 days).
Implications for health services delivery
COPD is a disease that requires a combination of self-care management by patients and their families, and disease management by a variety of healthcare providers, to ensure a good quality of life. Care provided by consistent health care providers or teams of providers who work collaboratively has been shown to allow optimal symptom management in the community, decrease the number of exacerbations of the disease and minimize unplanned visits to the hospital.
Chronic disease management in general requires careful oversight and, if possible, allow for the practitioner to provide a patient-centered and holistic management of the patients’ various diseases. Primary care teams of physicians, nurse practitioners, and nurses are ideally set up to provide this care to patients and their families, and to act as liaison with the acute healthcare system to seamlessly and quickly transition patients into community care. As such, any patient admitted to hospital for acute treatment would benefit from transitioning to a team of care providers immediately upon release from the hospital, to ensure an optimal disease management in the community, and decrease the number of admissions for COPD. This requires an increased effort to liaise with the community providers proactively.
It was clearly shown in this cohort that those who lacked continuity of care accessed the emergency department significantly more often, were admitted and then stayed longer, which can be interpreted that they were more unstable and required more aggressive treatment for longer than those who benefited from higher continuity of care.
Shortly after the completion of this study, the option to deliver virtual care by family physician and specialists has been more widely implemented and financially supported, in response to the COVID-19 pandemic. As the SELHIN region boasts the highest proportion of residents living in rural areas of Ontario and patients living rurally struggle with poorly developed public transportation, there is the possibility that this new care delivery method has improved continuity of care for some populations and had an impact on the provision of urgent and unplanned care for patients living with COPD. Future research would have to account for those who live at a distance from their care providers may have better access to care and are less likely to be in a lower continuity of care cohort. With the pandemic in 2020, care models have shifted to virtual model and future studies need to assess the best models of continuity in care that are adaptable to virtual/in person hybrid models.
The main strength of the study was the ability to precisely examine if there was there a difference in emergency room visits, admission to hospital and readmission in their sub region compared to the rest of the region as the study design and analysis allowed for a follow-up of a specific cohort of patients diagnosed with COPD over five years. Limitations of the study include not having access to prescribed and dispensed medication to the cohort, nor the status on screening for COPD using spirometry, as this data is unavailable.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by an Ontario Ministry of Health and Long-Term Care (MOHLTC) Applied Health Research Question grant (Project Trim 2020 0950 052 000). This study was supported by the Institute for Clinical Evaluative Sciences (ICES), which is funded by an annual grant from the MOHLTC. The opinions, results and conclusions reported in this paper are those of the authors and are independent from the funding sources. No endorsement by ICES or the Ontario MOHLTC is intended or should be inferred.