
Abstract
Introduction
Care Pathway Management intends to enhance the quality of care by restructuring care services. As recipients of care, patients have relevant experiential knowledge on the provision of care, but they are rarely involved in Care Pathway Management due to various barriers. This study aims to acquire insights into how patients can be meaningfully involved in Care Pathway Management.
Methods
A case study was conducted to assess the implementation of patient involvement in the co-creation of the care pathways of Soft Tissue Sarcoma and Gastrointestinal Stromal Tumour at Erasmus MC Cancer Institute (the Netherlands), using the Interactive Learning and Action methodology. Within the pathways, seven patients and eight health professionals were involved. To overcome expected and encountered barriers to involving patients, reflection was stimulated on the care pathways and the development process. Qualitative data were collected via interviews, participatory observations and informal conversations. For analysis, a patient involvement evaluation framework and criteria for knowledge co-creation were used.
Results
Patients indicated specific improvements for current pathways regarding communication, the assistance of a nurse and integrated care. However, the co-creation process encountered several barriers, including limited opportunities to overcome patients’ knowledge gap on medical care services, limited time and uncertainties about responsibilities. Moreover, participatory reflection to enhance the co-creation process was constrained by power imbalances between patients and health professionals and health professionals’ restricted perceptions of their role.
Discussion
To enhance the meaningful involvement of patients in Care Pathway Management, constraints in joint reflection on the co-creation process must be overcome.
Keywords
Introduction
(Integrated) care pathways are increasingly developed and used in health systems worldwide. By developing care pathways, multidisciplinary guidelines are translated into local structures and subsequently care services. 1 Care pathways can be used as structured interventions for continuously managing different care specializations. 2 This method, also known as Care Pathway Management (CPM), aims to evaluate and improve the quality, coordination and patient satisfaction of current care services provided to a specific patient group within a defined period of time. 3
In the Netherlands, CPM is often implemented by care coordinators. These organizational advisors facilitate the process of developing and implementing care pathways based on the Value-Based Health Care methodology. Health professionals are involved in this process, and the ownership is occasionally transferred to them. Although the aim of CPM is to improve patients’ care by restructuring care processes, patients are rarely actively involved in these processes.4,5 By focusing mainly on the organizational aspects of care, patients’ needs are overlooked. 6 Yet, CPM can have disadvantages for patients such as depersonalizing services and limiting care options. 1 In addition, patients – as the recipients of care pathways – have experiential knowledge on care services. This experiential knowledge can make a valuable contribution to the development of care pathways by defining clinical outcomes measures, improved access and navigation across services and formulating information needs. 7
Since the 1980s, patients’ experiential knowledge has been increasingly acknowledged as a legitimate source of information. A broad range of initiatives has been set up to involve patients within different areas of healthcare improvement, including guideline development, assessing the quality of care and the development of self-management tools. However, studies show many cases of tokenism in which patients’ involvement was treated as a box-ticking exercise.8,9 It is argued that to meaningfully involve patients, involving them as equal partners in a knowledge co-creation process could be helpful. 10 This process consists of three steps: first, patients’ implicit knowledge is made explicit (knowledge articulation); integrated with that of researchers and health professionals (knowledge integration) and sustainably implemented in healthcare innovations (knowledge embedment). In many cases, patients have difficulties in articulating their needs and ideas due to limited medical knowledge or being unable to think at a more abstract level. 11 Furthermore, their impact on knowledge integration processes was found to be limited because of the higher status of scientific knowledge 12 and limited interaction and learning among stakeholders.13,14 Embedment of integrated knowledge is even more challenging and rarely takes place. 13 With regard to CPM, patient involvement has been generally confined to knowledge articulation by consultation through, for instance, interviews. 15 Therefore, this study aims to acquire insights into how patients’ involvement in co-creating CPM can be realized in a meaningful manner.
Methods
A case study was conducted from January to December 2016 to assess patients’ involvement in the development of two care pathways at Erasmus MC Cancer Institute in the Netherlands. This initiative derived from the Institute’s intention to institutionalize patient involvement in care, research and policy, as indicated in its long-term policy plan (Erasmus MC Cancer Institute, n.d.).
Case
This study focuses on the care pathways of Soft Tissue Sarcoma (Sarcoma) and Gastrointestinal Stromal Tumour (GIST) because of existing collaborations. Within the scope of this study, a care pathway encompasses all clinical decisions from the moment of a patient’s referral to the hospital until the treatment has been completed, the patient is discharged or has died. At Erasmus MC Cancer Institute, CPM is implemented by care coordinators who work as organizational consultants within the institute. Each care pathway trajectory consists of a kick-off meeting with a leading health professional and sessions with health professionals from various specializations. Patients’ involvement normally depends on the wishes of the leading health professional, varying from none to joining all sessions (apart from the kick-off meeting), but is mostly confined to consultation. It was decided to involve patients throughout the process.
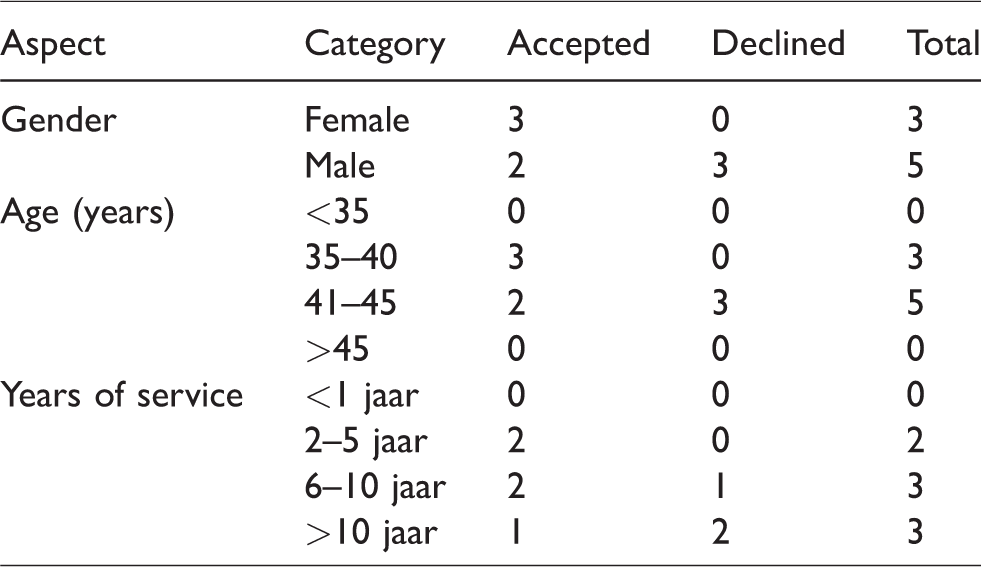
Participants comprised patients and health professionals. All health professionals working with the two patient groups were invited by the care coordinators via email. A representation of all relevant specializations (surgeon, internist-oncologist, radiologist, radiotherapist and pathologist) was sought. Five health professionals were invited for both the Sarcoma and GIST pathways. In addition, three radiotherapists were only invited for the Sarcoma pathway because radiotherapy is seldom used in GIST treatment. Respectively, five (62.5%) and three (60%) health professionals accepted the invitation. The pathologist declined for both pathways because he did not regard his presence as relevant. One radiotherapist and one internist–oncologist did not participate because their perspective was represented by a colleague. See Table 1 for an overview of the participating health professionals’ characteristics. For both trajectories, the surgeon took a leading role in the professional team. This role entailed that the surgeon was the contact person for the care coordinators and was responsible for the tasks of the professional team.
Invited health professional respondents’ characteristics (n = 8).
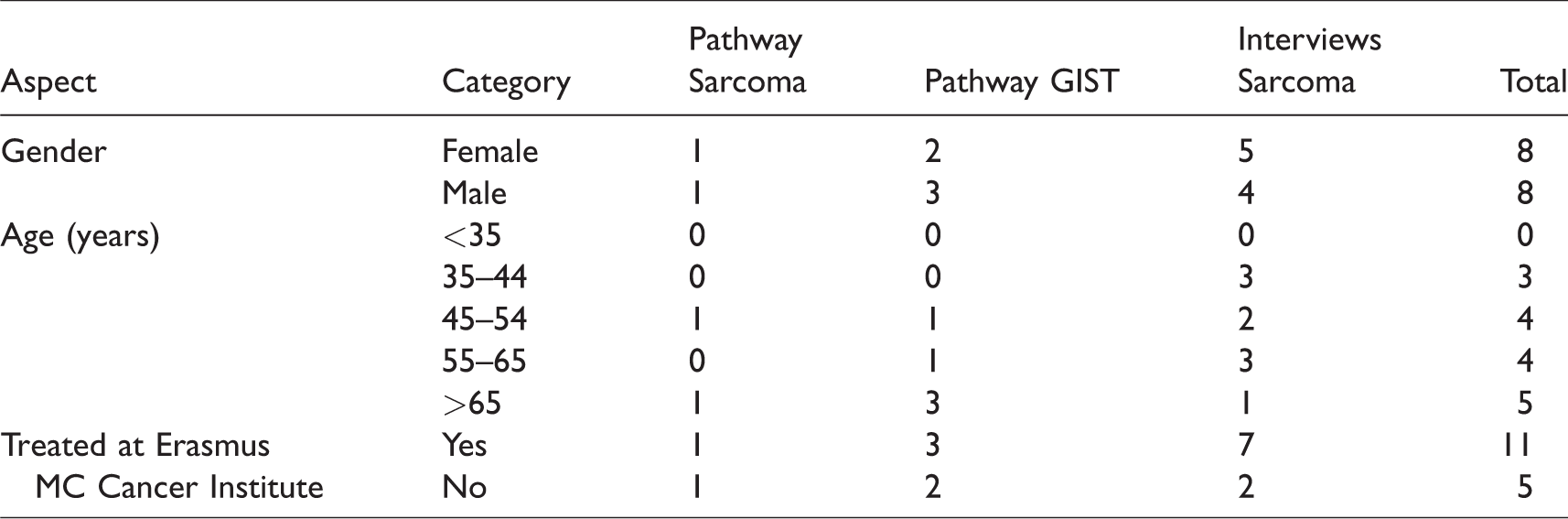
Patients’ representatives were recruited via direct contact by an involved health professional and newsletters of the patient organizations of Sarcoma and GIST. In 2016, the patient organizations had, respectively, 30 and 350 members. It was aimed to recruit at least two patients. Two Sarcoma and five GIST patients joined the trajectories. See Table 2 for the participating patients’ characteristics. Patients were invited to join both the kick-off meeting and the sessions. During the 90-minute kick-off meeting, the methodologies were introduced, and the CPM process was discussed. For the Sarcoma and GIST pathways, respectively, four and three sessions were organized. The sessions took approximately 1.5–2 hours and were facilitated by the care coordinators. Possibilities for improving current pathways and measuring relevant health outcomes were discussed. To increase the representativeness of patients’ input, the experiences of other patients were collected via interviews with nine patients recruited via the patient organization of Sarcoma (see Table 2) and the forum of the patient organization of GIST. The trajectories were conducted consecutively (see Figure 1 for the timelines of both trajectories).
Participating patients’ characteristics (n = 16).
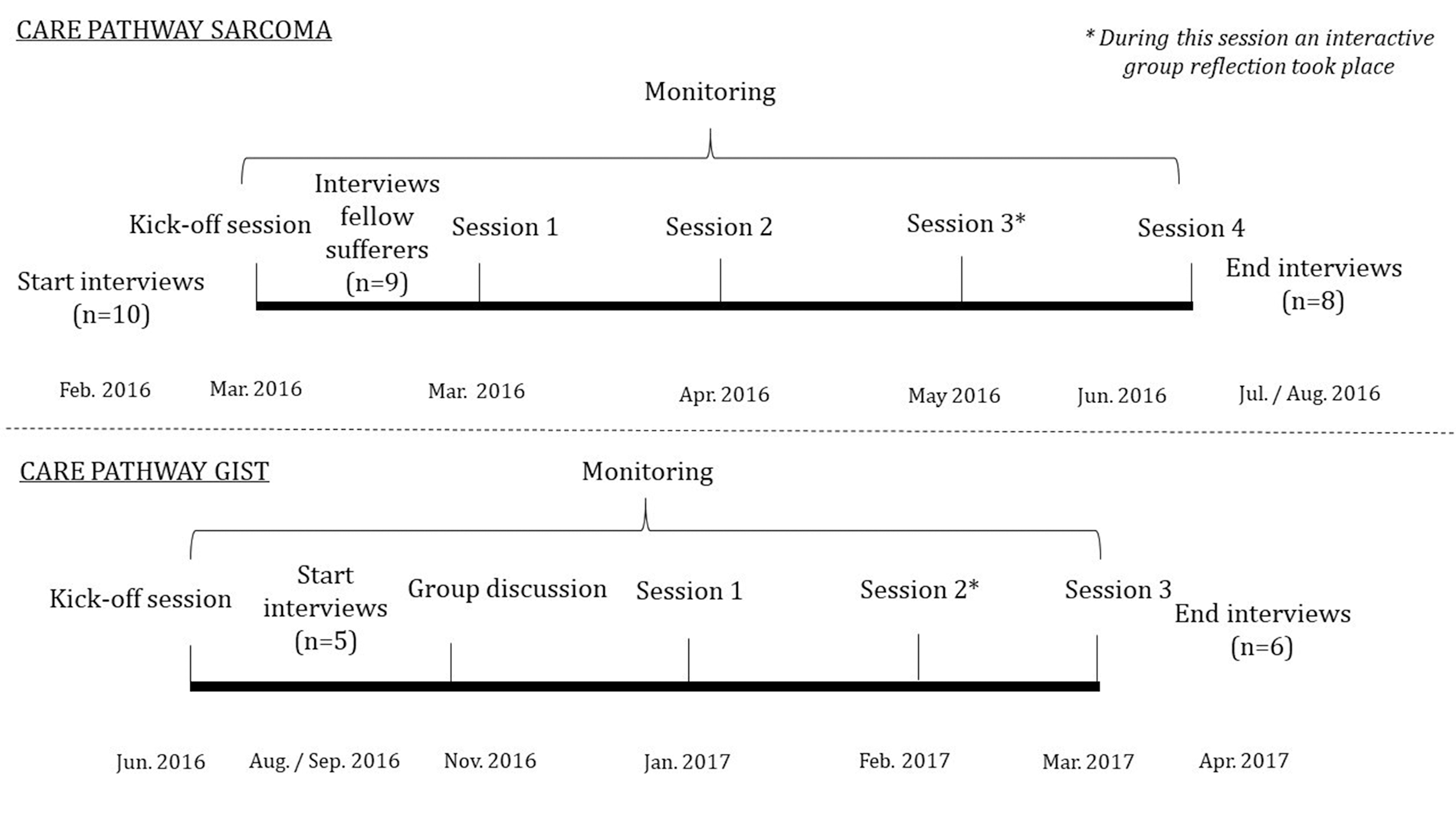
Timeline case study.
Research approach
To investigate the case in situ, the methodology Interactive Learning and Action was used. Interactive Learning and Action is a participatory approach for building common knowledge among stakeholders with diverse skills, interests and roles.16,17 The methodology actively involves participants in the monitoring process and enhances reflection among participants. Reflection is defined by Nguyen et al. 18 as a process of engaging in attentive, critical and iterative interactions with one’s thoughts and actions and their underlying frame, with a view to changing them and the view on the change itself. By stimulating learning, reflection is expected to overcome current barriers to involving patients in co-creating knowledge. 13
Data collection
Data were collected by the first author and a colleague who are academic researchers in the field of patient involvement via interviews, participatory observations and informal conversations. In line with the methodology, changes were made based on intermediate findings.
Interviews
Before the kick-off meeting and after the last session, semi-structured interviews were conducted with all invited participants. The start interviews focused on participants’ experiences and perspectives regarding patient involvement and expectations of the trajectory. The end interviews were held to reflect on participants’ experiences regarding their participation, the process and outcomes. One of the health professionals was not willing to participate in the end interview of both care pathways because of time constraints. The interviews were conducted by telephone and took 25–60 minutes.
Participatory observations
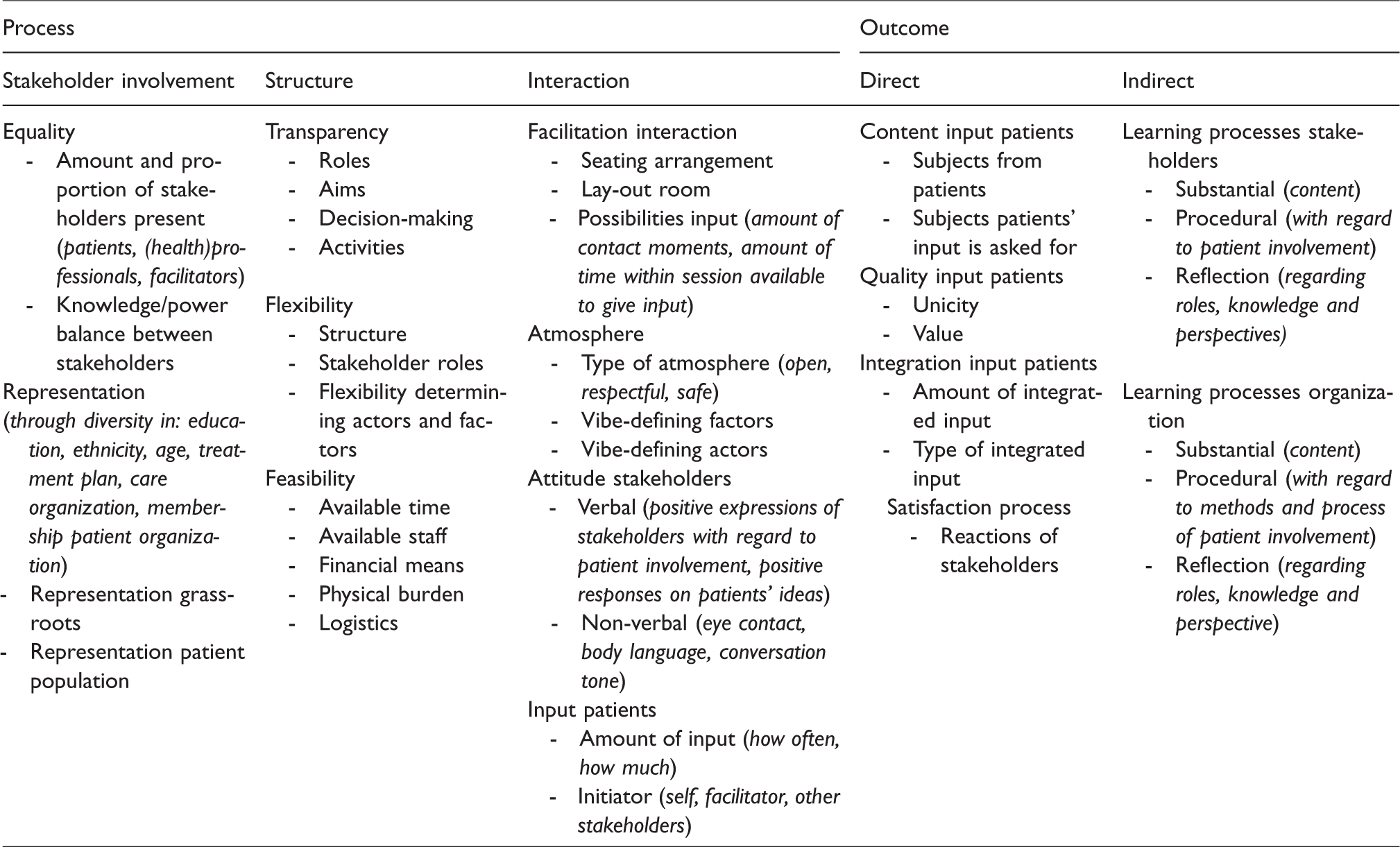
Participatory observations were used to monitor the quality of the process of patient involvement. Researchers recorded their observations of the (non-)verbal communication in field notes. An observation model (Table 3) was used, based on the evaluation framework of Caron-Flinterman et al., 14 and created to assess the quality of patient involvement in research agenda-setting, including both process and outcome criteria.17,19 The process was evaluated by looking at stakeholder diversity and methods of inclusion and the structure and management of the process. To what extent this involvement led to actual changes was evaluated by measuring the direct and indirect outcomes of the process. The researchers actively participated by assisting in the implementation of measures to improve the co-creation process.
Observation model to evaluate the patient involvement in the knowledge co-creation process, based on the evaluation framework of Caron-Flinterman. 17
Informal conversations
Throughout the trajectories, researchers had informal conversations with the participants, during which researchers asked participants to reflect on the process and provided additional information. After each session, the researchers and care coordinators mutually reflected on the process of the previous session and identified lessons learnt.
Strategies to stimulate reflection
To stimulate reflection throughout the trajectories, the strategies listed below were applied. These strategies evolved, adapting to stakeholders’ feedback and researchers’ observations.
Researchers encouraged individual participants to reflect during the interviews and informal conversations by posing critical supplementary questions and clarifying other perspectives. During the sessions, researchers stimulated group reflection by posing questions, asking for clarifications or giving additional information. Through their participation, researchers aimed to improve the quality of the patient involvement process. At the same time, researchers tried to remain neutral by maintaining a balance between their ‘insider’ and ‘outsider’ role. A group reflection was organized during the third (Sarcoma) and second (GIST) CPM session and facilitated by the researchers in collaboration with the care coordinators. For the Sarcoma care pathway, the Dynamic Learning Agenda was used as a reflective method, which supports learning processes by addressing challenges through reflection.
20
Based on participants’ feedback that this method was too time-consuming, another reflective method was developed for the GIST care pathway. This method made an inventory of participants’ positive and negative experiences by placing the statement: ‘I think it is good that …’, or ‘I think it would be good that …’ and the underlying reasons and causes.
Through these strategies, researchers tried to stimulate reflection on patients’ involvement in co-creating CPM (single-loop learning), decisions based on their involvement (double-loop learning) as well as underlying perspectives for these decisions (triple-loop learning). 21
Data analysis
The interviews were recorded and transcribed verbatim. The MAXqda 2007 software program was used to conduct a thematic analysis of the interviews. The transcripts were coded via a combination of closed and open coding. Codes were derived from the observation model (Table 3) and the assessment criteria of Pittens. 13 Although there is overlap, these criteria more specifically focus on knowledge co-creation. The field notes were coded manually based on the coding scheme of the interviews. The categorized segments were clustered into sub-themes and structured according to the three steps of the knowledge co-creation process. Subsequently, the categories and themes were discussed with the co-authors.
Ethics
In accordance with the Dutch law, ethical approval by a formal medical ethical committee was not required for this study. The researchers adhered to the national Code of Ethics for Research in the Social and Behavioral Sciences involving Human Participants. 22 All participants received prior verbal and written information about the study objectives and the possibility to withdraw from the study at any moment. All data were anonymized before analysis and stored securely.
Results
The results are structured according to the three steps of knowledge co-creation. We first present the findings in relation to the outcomes, followed by the findings on the process.
Articulation of patients’ and professionals’ knowledge
Outcomes
Both Sarcoma and GIST patients indicated that communication within the care pathways is currently limited. Specifically, the lack of communication after the first consultation and about transfers was mentioned as well as the limited possibilities to pose questions after the consultation. Although health professionals indicate that patients can always contact them, patients feel unable to do so because of the health professionals’ busy schedules. Patients also highlighted that due to the short time between diagnosis and initial treatment, there was little time to reflect, which is needed for shared decision-making. Both groups, but specifically, the GIST patients, indicated problems regarding transfers. Patients were frequently not, or not in a timely fashion, transferred to a specialized centre. Moreover, patients felt that health professionals lacked attention for informal caregivers, the reintegration into daily activities, physiotherapy and psychological support. Health professionals’ input was mainly focused on translating current practices into a care pathway and formulating practical limitations for implementing evaluation methods and improvement measures. The radiologist, for instance, mentioned that giving patients access to X-rays before the consultation could cause confusion because nuances in the accompanying texts are left out.
Process
Patients and health professionals also identified issues related to their involvement in the process. Patients valued the encouragement to share their knowledge. In addition, patients expressed their appreciation of researchers’ support in giving additional information.
Participation was, however, sometimes discouraged by health professionals’ results-oriented attitude. When the provided input was not directly related to the end terms of CPM, such as addressing a personal anecdote, evaluating the initiative or explaining the methodologies, some health professionals appeared absent by, for instance, looking at their mobile phone: ‘Some health professionals’ lack of interest dissuaded patients from asking their questions’ (Professional_Sarcoma_ EndInterview4).
Most patients pointed out that the discussions during the CPM sessions were not always accessible for the ‘general’ patient. The Sarcoma patients specifically indicated the difficulty in participating because they felt that they had to go along with health professionals’ way and pace of working. As a result, they did not have enough time to ask for explanations. Because the GIST sessions were difficult to plan, the kick-off meeting was too long ago for patients to remember the methodologies that were explained. In addition, preparation materials were sometimes lacking or sent too late to prepare properly. Patients’ lack of insights into hospital logistics and unfamiliarity with medical concepts and jargon hindered them from formulating their own knowledge.
Although patients acknowledged that it was impossible to truly represent the large diversity of patients, they felt that they could do this sufficiently because they were aware of the experiences of other patients through interviews and a forum. Contact with other patients during the trajectory was, however, a challenge, because the time between meetings was too short to organize consultations. In addition, one of the patient organizations had relatively few members and therefore limited possibilities for outreach in consulting other patients.
Some health professionals and a few patients commented on the efficiency of the process. This feedback was given informally and during the interviews but was not mentioned during the group reflections. The health professionals indicated that their efforts in the CPM process were constrained by their heavy workload. Compared to their other activities, involvement in CPM was not a high priority. According to these professionals, time could be saved by incorporating lessons from previous trajectories and by setting up the care pathway – which is already known – before the start of the sessions. Inefficiency was also mentioned by two health professionals regarding patients’ involvement. They advised consulting patients only on specific topics via phone or email. Two GIST patients also mentioned that participation was quite time-consuming and greater efficiency was desirable. On the other hand, other health professionals and most patients indicated that joining all the sessions created a safe atmosphere and resulted in unexpected lessons. A few health professionals thought that the group reflections took too much time. Although they would like to have a voice in the CPM process, reflecting on the process was regarded as a task of the care coordinators. Two other health professionals specifically mentioned that the reflections were valuable in generating new ideas, such as the need for involving patients in evaluating the care pathways in the long run, which was an eye-opener for them.
Integration of patients’ and professionals’ knowledge into decisions on CPM
Outcomes
Patients and health professionals articulated knowledge that was complementary. While patients’ input was mainly focused on creating a more transparent and empowering care pathway, professionals’ input generally addressed the efficiency, feasibility and practical implementation of improvement measures. The different types of knowledge were integrated into decisions on the inclusion of certain communications and care steps in the care pathways and the content and use of evaluation instruments. For instance, the decision to write a job profile to employ a specialist nurse was based on patients’ feedback on the limited chances to pose questions and professionals’ remarks about the lack of a case manager. Patients’ comment that limited attention is paid to reintegration into daily life and health professionals’ input that these services cannot be provided in a hospital setting led to the decision to look at integrated care pathways within CPM in the future.
Knowledge integration generated (mutual) learning among participants. Patients became more aware of the considerations in organizing care services and therefore became more sympathetic to health professionals’ perspectives. Professionals learned about patients’ needs and obtained insights into how the activities of different disciplines are connected. Moreover, patients and health professionals gained experience in how patients could be involved in CPM and what specific knowledge patients could add. Especially in relation to the Sarcoma patients, health professionals mentioned being surprised about their level of thinking. Although professionals’ actions are targeted on improving patients’ quality of life, this project showed that professionals’ ideas on patients’ needs are not always in line with patients’ wishes. That was an eye-opener for them. Professionals became aware that patients can have a valuable input. (Patient_Sarcoma_EndInterview12)
Process
According to both patients and health professionals, the use of preparation materials, the professional way the sessions were facilitated and the positive atmosphere during the sessions stimulated interaction and helped participants in integrating their knowledge. Participants showed interest in each other’s opinions and ideas by listening carefully and asking for each other’s views. Much time, however, was spent on clarifying the concepts and articulating knowledge, which restricted the time to discuss and integrate views. As a result, decisions were not made, for instance, on the accessibility of radiology reports and assigning a person responsible for improving the provision of information. In my opinion there was too little attention for the things we would like to change. We for instance discussed the use of surveys and the opportunities of certain measurements, but decisions were not made. (Professional_Sarcoma_EndInterview6) What I found difficult is that as an outsider you are introduced in a medical culture you are not familiar with and into a group of people who sees each other on a regular basis or are at any event used to deliberate with one another. (Patient_Sarcoma_EndInterview10) Well, if patients prefer professionals to join the group discussion, it is not for me to question this idea. I mean, those patients come here for the first time, get explanations about patient involvement. Then I cannot say: ‘I don’t feel like it’. (Professional_GIST_EndInterview4)
Embedment of integrated knowledge into CPM
Outcomes
The minutes of the sessions demonstrated that the results of knowledge integration on CPM were taken up by the care coordinators in the CPM pathway. In addition, the intention to include patients’ input in the long term was expressed. Patients were involved in writing a follow-up proposal on developing integrated care pathways in CPM, but no further appointments on future collaborations were made. Furthermore, most participants mentioned that there was limited feedback on the follow-up. Several patients indicated the wish for continuing future collaboration through regular contacts between patient representatives and health professionals in which they evaluate current care services.
Process
Care coordinators took several measures to implement participants’ feedback on the CPM process. Among others, the group reflection was shortened, and the initial pathway of GIST was developed before the sessions. This flexibility of adapting the trajectories motivated health professionals to continue, but there was less flexibility in further adapting CPM methodologies to be more efficient. Patients’ feedback on the difficulty of grasping the methodologies and concepts and therefore giving input did not directly lead to changes in the process.
Discussion
The results show that patients’ involvement in CPM leads to specific improvements for care pathways, like making pathways more transparent and empowering. However, to enhance the meaningful involvement of patients in CPM, constraints in joint reflection on the co-creation process must be overcome. This study showed that joint reflections were not well received by various participants, particularly the health professionals. Based on informal conversations, we argue that the top–down decision to set up the project and the extra workload due to the relocation of the Institute contributed to the limited motivation to reflect on the process. A lack of time has also been mentioned as a barrier for reflective practices among health professionals by Thompson and Thompson. 23 This study adds the finding that reflection was seen by most health professionals as the care coordinator’s area of responsibility. The group reflections were regarded as an extra activity in addition to the CPM trajectory, which they already regarded as a low priority compared to their ‘primary’ work, rather than an integral part of their work. In addition, reflection was impeded because neither patients nor health professionals felt comfortable about expressing critical views in a mixed setting due to the unequal quotas of power. These factors acted as a pragmatic boundary, such as described by Collins and Ison, 24 undermining the possibility of shifting from involvement to triple-loop learning (also referred to as social learning). The care coordinators, considered to be change agents within the process, went along with the health professionals’ need for efficiency to keep them on board. This decision further impeded triple-loop learning. Due to limited triple-loop learning, it was difficult to overcome expected and encountered barriers to co-creating knowledge such as limited time, power imbalances, uncertainties about responsibilities and lack of prioritization of the CPM process (and reflection on it). Single- and, to a lesser extent, double-loop learning took place, increasing both patients’ and health professionals’ empowerment.
A strength of the study is the use of multiple data collection methods in which findings from one method could be validated through another method. A limitation is that the same health professionals were involved in the GIST and Sarcoma pathway. The findings could therefore depend on the specific personalities and the characteristics and dynamics of the professional team.
To improve patients’ involvement in co-creating CPM, barriers to group reflections must be overcome. Based on the outcomes of this study, we suggest that care management should involve participants in setting up patient involvement initiatives in order to stimulate commitment and detect and overcome potential barriers (such as time constraints) at an early stage. Within this stage, it is important to create possibilities for participants to express their concerns outside group meetings in order to mitigate power imbalances. Digital reflection methods can also be useful for giving anonymous feedback. Furthermore, health professionals should be empowered to have a reflective interaction with patients by adding participatory reflections in the medical training curriculum. This could also help in overcoming restricted perceptions of appropriate roles. In tandem, showing the effectiveness of reflection should help in stimulating a culture in healthcare organizations that values reflective approaches. 23
In conclusion, patients’ value could be improved by meaningfully involving them in co-creating CPM. Meaningful involvement could be attained by overcoming barriers to joint reflections such as low prioritization, restricted role perceptions, a high workload and power imbalances.
Footnotes
Acknowledgements
We especially thank the participating patients and health professionals for their time. We also thank Eveline Smit for her help in collecting and analysing the data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This article was supported by KWF – the Dutch Cancer Society.