
Abstract
Introduction
This study investigates future integrated care competencies among workforce in health and social service sectors in the context of the national health and social services reform in Finland.
Methods
The sample was drawn from the registers of competent workforce in the social and health sectors in Finland in three different forerunner areas. Eight working sectors were identified. A total of 1943 participants represented a 16% of the sample (N = 12,250). Factor analyses were conducted on ratings from the COPE scale measuring integrated care competences. Logistic regression analyses were used to examine the associations between background variables and competence factors.
Results
The present study identifies three factors about the competences of future integrated care competencies. The factors were client-oriented needs assessment, holistic service guidance, and ensuring service path. The sectors of services for older people and administration indicated the highest level of competence needs, whereas the sector of social services indicated the lowest level. Variations between sectors and background variables are remarkable.
Discussion
The study points out three dimensions of generic competence needs perceived by employees that are required to secure client-oriented integrated care processes in the future. New competencies and targeted processes in organizations and between sectors are crucial in developing the quality and effectiveness of integrated care by improving future care processes. Professional education and training should advance the learning of generic competences shared by all professionals and sectors in accomplishing integrated care.
Keywords
Introduction
Integration has been found to be the core aspect in improving health care quality and the continuity of care between different actors in the health and social care sectors. Concrete collaboration between different actors in health care and particularly between professionals in health care and social services are significant for better integration. 1 Fragmentation of services may increase costs and decrease care quality due to duplicate tests, lack of communication between service providers, and disrupted continuity. An aging population increases the negative outcomes of fragmentation as there are also a growing number of patients with co-morbities. 2
The health and social care system in Finland has experienced considerable difficulties with citizens’ equal access to and integration of services. The health and social services (SOTE) reform is an initiative undertaken by the governments in the 2010s to manage those challenges through restructuring the organization of public health care and social services. Other major drivers for the reform are increased costs due to the rapidly aging population and economic disparity of municipal health and social care services.3,4 Therefore, larger organizations than municipalities are needed to take responsibility of health and care services. 5 The law proposal suggests that in the future 18 counties would take responsibility of all health and social services.
Besides the larger service purchasers, another guiding principle of the reform is to increase freedom of choice in services, where the citizens can choose a service provider among a variety of authorized providers from the public, private, or third sector. The integration of previously separate health care and social welfare services is considered a key method for improving the equality of services and organizing them efficiently and cost-effectively. This requires that the client’s needs are assessed as a whole and information flows smoothly between the actors. In addition, digital transformation is among the key priorities in the reform to ensure a uniform service platform, integrated information systems and digital services. 4
Integrated care as an emergent worldwide working model6,7 requires new skills and competences. According to the World Health Organization, key competences for integrated health services are patient advocacy, effective communication, teamwork, people-centered care, and continuous learning. 7 A recent EU report 8 further points out increased demand on multiprofessional competences, such as multi- and interdisciplinary team working, regulatory awareness, and systems thinking. The aim of interprofessional working is to ensure a responsive and integrated approach to care management focused on the needs of patients or clients. This further requires an integrated assessment and plan of service that is implemented in partnership with clients. 9
This paper aims to investigate the competence needs related to integrated care in the context of the recent health and social services reform in Finland. Recent studies show that macro-level organizational changes are not sufficient to achieve care integration in everyday micro-level practices.10,11 Therefore, it is important to identify novel competences required to overcome present inadequacies, such as poor communication, “silo” thinking and unclear responsibilities, that hinder care integration. 1 For example, Jolanki et al. 1 found that patients in health care clinics were forced to take an active role as the coordinator of their care, which is in contradiction with the idea of people-centered care. 7 In line with previous scarce research, a recent report 12 emphasizes generic competences learned and shared by all professional groups as a prerequisite for successful reform. Shared competences related to working with clients, developing services, and managing changes in collaboration should provide the basis for care coordination across the health and social care sectors. 12 Generic competences, however, do not diminish the importance of professional expertise, but help to get the best out of it in the integrated service provision aiming to meet the complex health and social care needs of the future. 9
Competence can be generally defined according to Weinert 13 as a “specialized system of abilities, proficiencies, or skills that are necessary or sufficient to reach a specific goal”. Other definitions specify for example key and meta competences, general and special cognitive competences, 13 and technical and behavioral competences including attitudes. 14 According to Mulder, 15 professional competence is a generic, integrated, and internalized capability to deliver sustainable effective performance for instance in a certain professional domain, role, and task situation. Competence consists of various competencies that are coherent clusters of knowledge, skills, and attitudes, which can be utilized in real performance contexts. Currently, the idea of competence is institutionalized by the EU. 15 The European Qualifications Framework (EQF) within which learning outcomes are linked to concrete competence requirements arising from working life increasingly guides professional education and training in Europe. They are conceptualized in terms of knowledge, cognitive and practical skills, autonomy, and responsibilities at each education level. 16
Aim
The study investigates and compares expected competence needs among the workforce in forerunner organizations in Finland, which have anticipated the health and social services reform and been active in the reorganization of integrated health and social services. Furthermore, associations between future competence needs and organizational change are examined. The specific aim was to construct and pilot a self-report measure based on competencies of integrated care especially required in working with clients.
Methods
Participants and data collection procedures
The present study operates in the context of the “Competent workforce for the future” (COPE) project. The project explores the transition in health and social services and its impact on employment, competence needs and development. The study protocol has been described in detail elsewhere (https://www.stncope.fi/en/project-information/).
The total sample was drawn from the personnel registers of three large organizations or areas arranging and providing social services and health care. The areas were South Karelia, North Karelia, and Central Uusimaa. Data were obtained electronically. Two reminders were sent by the contact persons in the areas. The present study was a cross-sectional research design, and data were collected in 2017. The questionnaire in Finnish covered topics on work and management changes, competence, professional decision-making, influence on work-related matters, stress at work, management, welfare, and a multicultural approach. The data set consisted of 1943 participants representing 16% of the sample (N = 12,250). The Research Ethics Committee of the National Institute for Health and Welfare (THL) expressed an affirmative statement of the study.
Measures
Development of competencies
As a part of the questionnaire, the respondents were asked to evaluate future changes in competence needs. The questions were constructed for the present study based on the aims and principles of integrated care within the health and social services reform. Three experts of health care and social services were consulted to ensure the validity of questions. Following the EQF guidelines, 16 competences were operationalized as concrete competence requirements in the integrated care process.
The scale consisted of 21 items covering four different patterns of competences expected to be relevant to all professionals with regard to integrated care. They were client orientation, clients’ responsibility for personal or a loved one’s welfare, access to services, and the fluency and clarity of services. The respondents were asked to rate the change of each competence need within the next five years at their work, ranging from “decrease very much” (1) to “increase very much” (5). From these items, three factors were formulated using factor analysis and counted sum indices. For the further analyses, we dichotomized the sum indices at the mean to indicate either high or low factor value.
Demographics and covariates
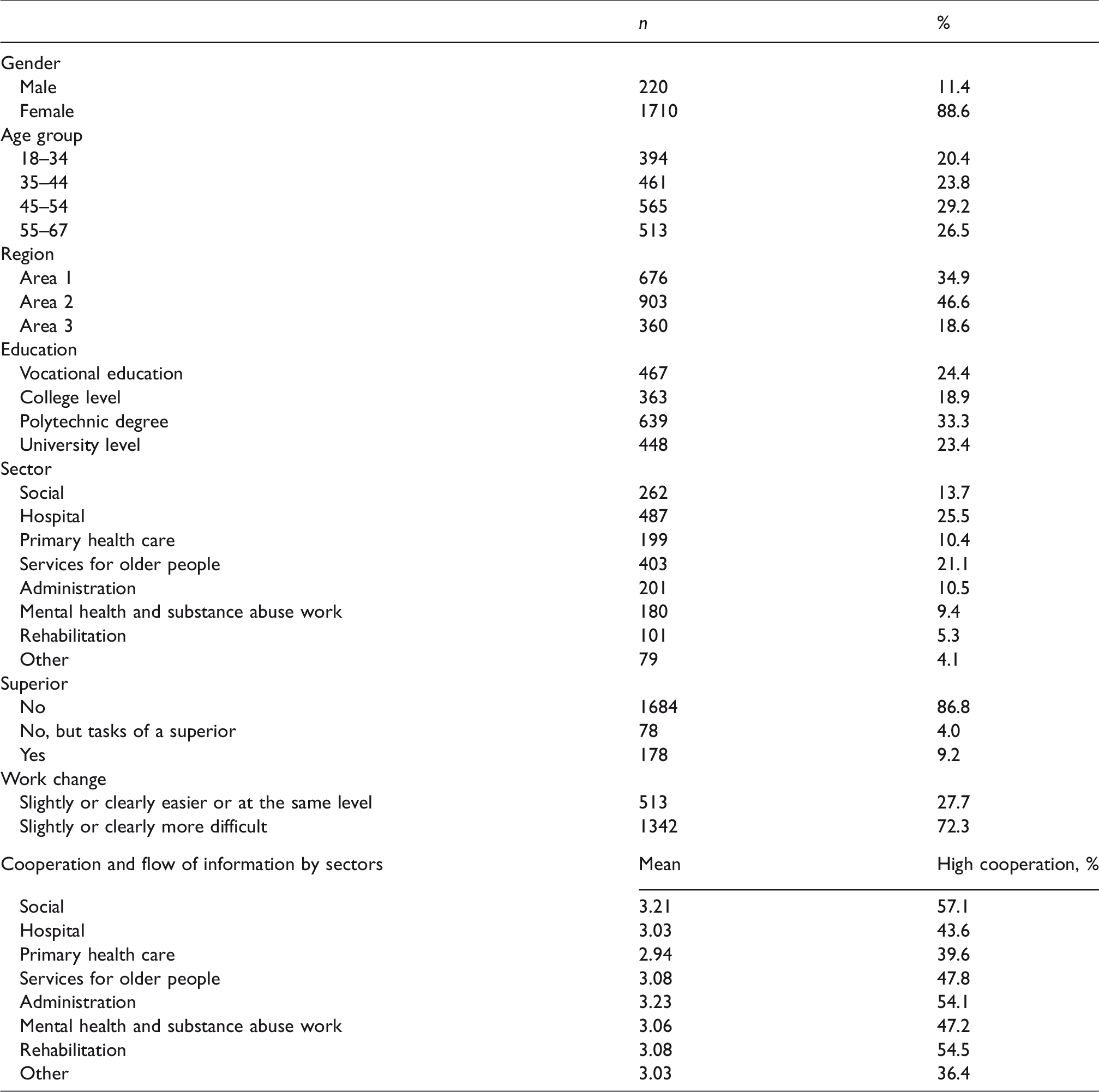
For control purposes, the following background sociodemographic information were included in the analyses: gender, age group, region, and education. The respondents were divided into four age categories: 18–34, 35–44, 45–54, and 55–67. The mean age was approximately 47 years. The three working place categories were South Karelia, North Karelia, and Central Uusimaa. Education was coded into four categories: vocational education, college, polytechnic (bachelor’s degree), and university (master’s degree) level.
Working sector
The main working sector was based on the respondents’ self-reporting. The number of alternatives was approximately thirty. Consequently, responses were combined and classified into eight groups. The working sectors were social services, hospital, primary health care, services for older people, administration, mental health and substance abuse work, rehabilitation, and other.
Superiority
Working status was examined with the question: “Are you working as a superior?” The answer alternatives were “No”, “No, but I have the tasks of a superior” and “Yes”.
Cooperation and flow of information
The respondents were asked to think about a client who needs different health and social care services and to rate “How good the cooperation and flow of information between your work unit and other units/organizations is from the viewpoint of the client?” Cooperation and flow of information was based on a sum index. Cooperation with eight different professional partners was evaluated on a five-point scale ranging from “poor” (1) to “very good” (5). The professional partners and sectors were primary health care, special health care, services for older people, mental health and substance abuse work, social work, other social services, other municipal sector, and third sector. The sum index was dichotomized at the mean to indicate either “high” or “low” cooperation.
Work change
Work change was defined by the answer to the question “How have the requirements of your work changed during the last one to three years?” It contained five alternatives: “much difficult”, “slightly difficult”, “same level”, “slightly easier”, and “clearly easier”. It was dichotomized with the three latter alternatives as “same/easier” and the two first alternatives as “difficult”.
Statistical analyses
A factor analysis was used to explore the ratings from the Cope data (Table 2). Cronbach’s alpha was used to evaluate the internal consistency of the 21-item scale and the subscales covering the initial four patterns of competences. Logistic regression analyses were used to examine the associations between the comprised factors and the independent variables (Tables 3 and 4). The results are presented using odds ratios (OR), 95% confidence intervals (CI), and variances explained (R2 Nagelkerke). Table 3 presents the differences between the working sectors by factors. Each category was compared to the overall effect. ORs below one indicate that a rate is less common than average and vice versa.
Description of variables (n, %, mean).
Factor analysis of the future competence needs from Cope data.
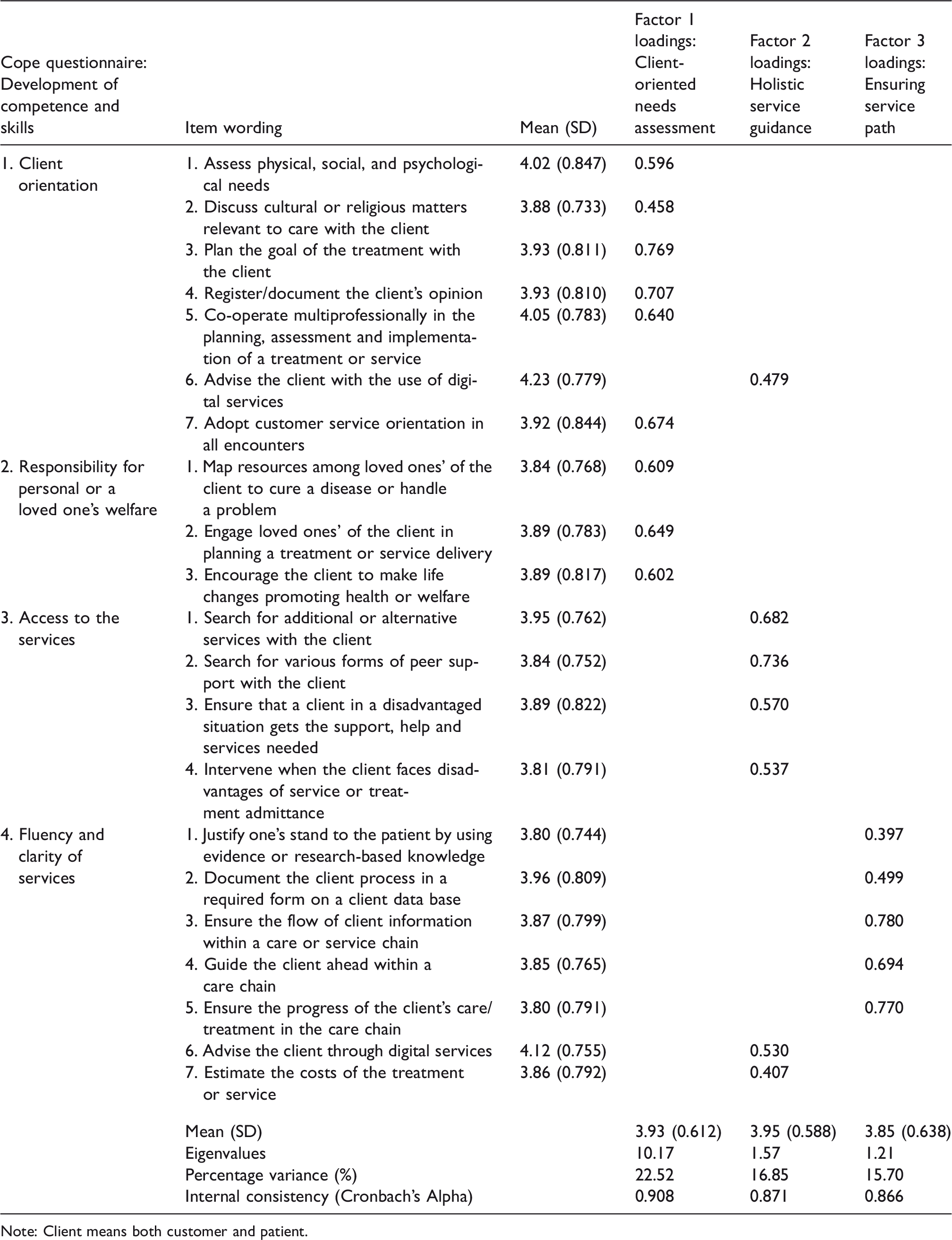
Note: Client means both customer and patient.
Odds ratios (OR) and 95% confidence intervals for factors 1–3 by sectors, reference group the whole data (OR = 1).
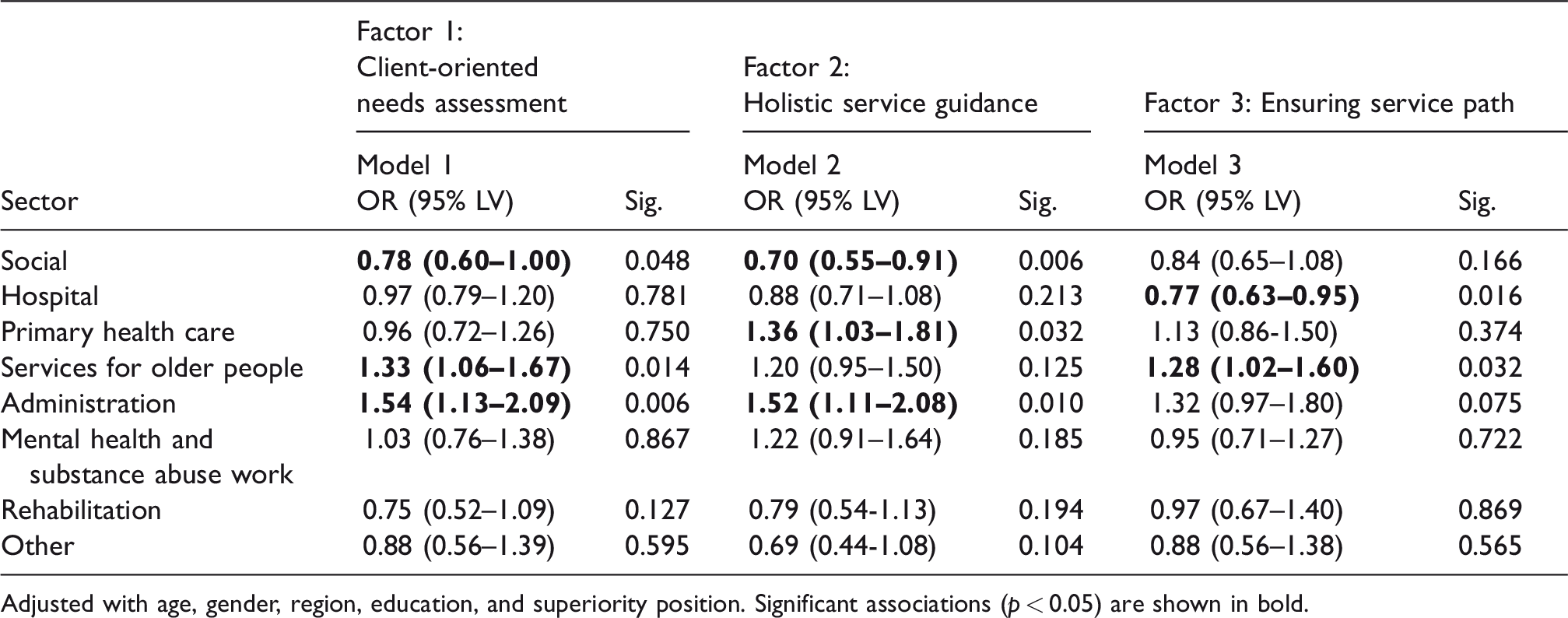
Adjusted with age, gender, region, education, and superiority position. Significant associations (p < 0.05) are shown in bold.
Odds ratios (OR), 95% confidence intervals and R 2 (Nagelkerke) for factor 1 (customer oriented need mapping), factor 2 (holistic service guidance), and factor 3 (ensuring service path) by gender, age, education, region, superior, cooperation, and flow of information and work change.
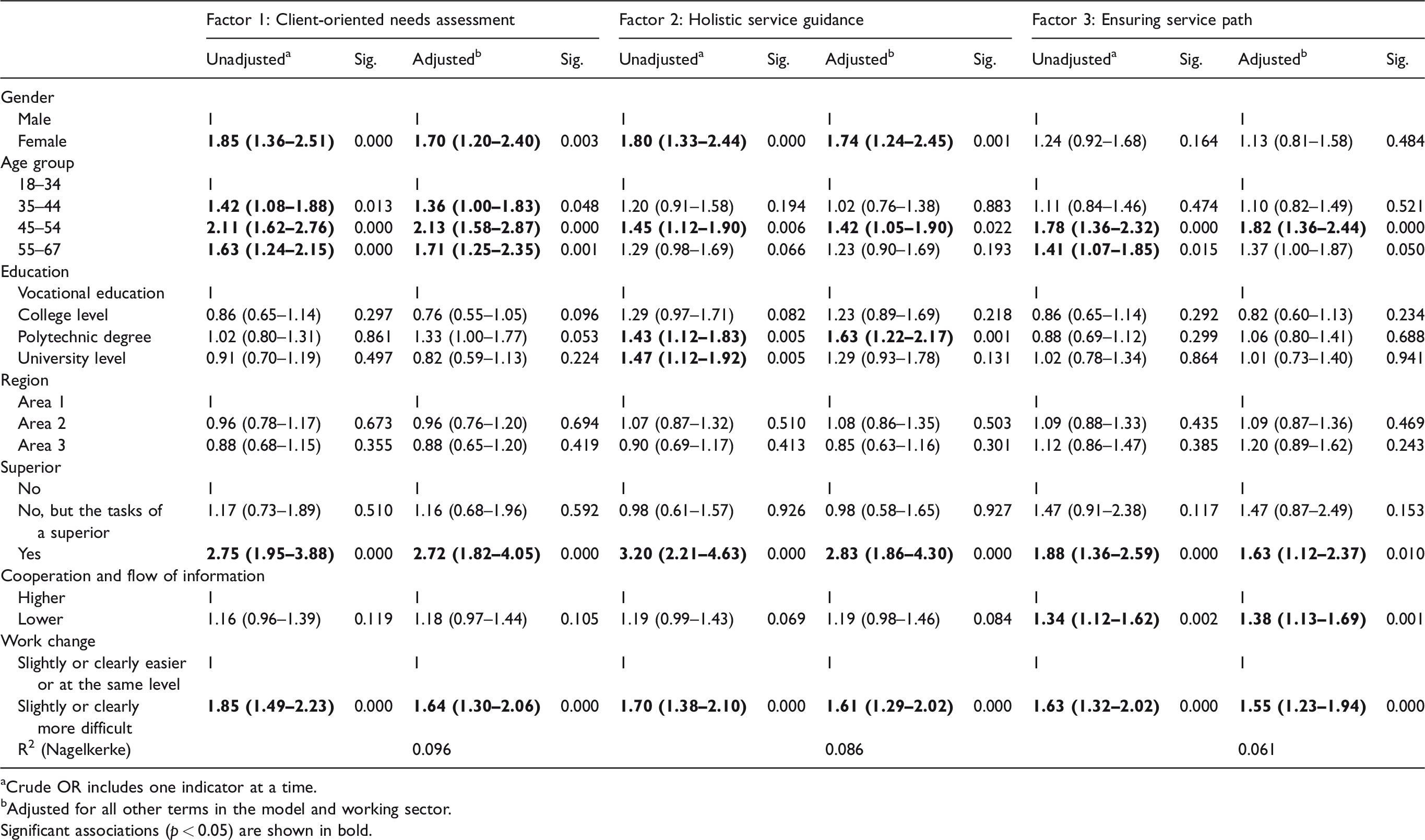
aCrude OR includes one indicator at a time.
bAdjusted for all other terms in the model and working sector.
Significant associations (p < 0.05) are shown in bold.
Data were analyzed using the IBM SPSS version 25.0 software package.
Results
Demographics of the respondents and other study variables are reported in Table 1.
Table 2: Factors
The 21-item scale was examined for construct validity by using factor analysis (Table 2). The KMO (Kaiser–Mayer–Olkin measure of sampling adequacy) was 0.952. Bartlett’s test of sphericity was significant for the whole scale (p < 0.001). The maximum likelihood factoring extraction produced three interpretable factors. The results indicated that a three-factor solution was the best fit to data. Factor names were determined based on the items’ content. The factors were named as “Client-oriented needs assessment” (factor 1), “Holistic service guidance” (factor 2), and “Ensuring service path” (factor 3). Cronbach’s alpha for the whole 21-item scale was 0.95. In addition, Cronbach’s alpha for the 9-item scale (factor 1) was 0.91, for the 7-item scale 0.87 (factor 2), and for the 5-item scale 0.87 (factor 3).
The descriptive statistics of factors (mean, standard deviation) showed that the highest mean (rounded) was 3.95 (SD = 0.59) in factor 2, 3.93 (SD = 0.61) in factor 1 and 3.85 (SD = 0.64) in factor 3, indicating that workers saw the competence needs to increase in all areas. Of the single items, workers saw the competence needs in “Advise the client with the use of digital services” (4.23) and “Advise the client through digital services” (4.12) to increase the most. The mean value was also relatively high in “Co-operate multiprofessionally in planning, assessment, and implementation of treatment or service” (4.05) and “Assess physical, social, and psychological needs” (4.02).
Table 3: Working sectors
According to Table 3, client-oriented needs assessment (factor 1) was seen to increase more in services for older people and administration than in other sectors. In contrast, in social services, these competency needs were evaluated lower than in other sectors.
The results for holistic service guidance (factor 2) showed that increase requirements in primary health care and administration competencies were bigger than in other sectors, and in the sector of social services, the increase was smaller than in other sectors. Also, among the services for older people and mental health and substance abuse work, these competencies were seen to increase more than average, but the relationship was not statistically significant.
The analysis on ensuring service path (factor 3) showed an above average increase only in services for older people. In administration, competencies in ensuring service path were seen to increase slightly more than in other sectors, but the results did not reach statistical significance. Finally, in the hospital sector, increasing the competency needs related to ensuring service paths was lower than in other sectors.
Table 4: Associations of competences with background variables, co-operation, and changes at work
According to the figures in Table 4, competencies in client-oriented needs assessment and holistic service guidance were seen to increase more among females than males. This was also observed particularly among the 45–54 years age group regarding all factors. In addition, higher education indicated somewhat higher needs in holistic service guidance. Also, workers in a superiority position saw the need for an increase in all the competences in the future more clearly than others.
The odds ratios rather consistently indicated a strong association with client-oriented needs assessment and the indicators of the role of being a superior and work change. The results indicate that superiors see competencies in client-oriented needs assessment to increase much more that employees. The lower cooperation and flow of information was related to the higher increase of competencies in ensuring service path than in the group of higher cooperation.
The previous changes at work were related to the increase of all competences. The odds ratio was almost double if work had become more difficult than in cases where no change in work difficulty had happened. Workers’ ratings of cooperation and flow of information among other sectors were related only to the increase of competencies in ensuring service path.
The last row of Table 4 shows that there was a slightly higher percentage of explained variance (R2 Nagelkerke) by all indicators in factor 1 (approximately 10%) than in the other factors (9% in factor 2; 6% in factor 3). The information indicates that background variables had stronger correlations to factors 1 and 2.
Discussion
Main findings
The present study showed that the 21-item scale on the development of competencies was sound in terms of construct validity and internal consistency. The scale was conducted to measure and identify several constructs which are significant for integrated care in the context of the health and social service reform in Finland. The analyses revealed the existence of three independent factors about future competencies related to working with clients. The factors were named “Client-oriented needs assessment” (9 items), “Holistic service guidance” (7 items), and “Ensuring service path” (5 items). The highest needs among single competencies were those related to e-services.
Workers in services for older people and administration saw the competency needs in client-oriented needs assessment (factor 1) to increase higher in the future than other groups and in social services the increase was seen lower. Need of competence in holistic service guidance (factor 2) was seen to increase mostly in administration and primary health care and to decrease in social services. Competence in ensuring service path (factor 3) was seen to increase mostly in services for older people and less so in hospitals.
The present study found that the most important indicators associated with all of the factors were the position of being a superior and changes that had occurred at work during the past few years. Higher age, particularly the age group 45–54 was associated with all of the factors, too. Poorly functioning cooperation and flow of information was associated significantly particularly with factor 3, ensuring service path. Additionally, higher level of education was associated with holistic service guidance (factor 2).
Discussion of the findings
The three identified dimensions in competence needs can be expected to be crucial for patient experience of high-quality care.17,18 Client-oriented needs assessment involves a client-oriented mind-set and client engagement in treatment plans as crucial competencies that in turn require skills in client-centered counselling. 12 Competencies in holistic service guidance reflect efforts to maximize clients’ opportunity to obtain the most suitable services to their needs and to secure their entitled admission to services; these competencies seems to be related to patient advocacy 7 and other capabilities in ethical practice. 9 Competencies related to ensuring service path entail actions to secure effective and seamless services from the perspective of client, which requires evidence-based decision-making, standardized documentation, and responsibility taking for the functionality of the care chain.
The findings reveal a demand for multiprofessional competencies, consistent with recent international accounts.7,8 Multiprofessional working is obvious in coordinating care and services and securing an individual care path (factors 2 and 3), but it also plays an important role in comprehensive needs assessment (factor 1, item 5), which provides the basis for integrating care. Furthermore, novel competencies in using information technology are required in providing e-services and ensuring the flow of information and, therefore, are fundamental for the integration of services. 6
The findings regarding lower increases in competencies of client-oriented needs mapping and holistic service guidance in the sector of social services compared to other sectors may be due to the requirements of the new Social Welfare Act in 2015. 19 The act stipulates social welfare workers to make a service needs assessment according to the client’s life situation and co-operate with professionals in other sectors to meet the client’s individual needs for services. New competences in professional education as well emphasize comprehensive needs assessment as one of the key competences. 20 Obviously personnel are already working in line with the new requirements and recent competencies are assumed to be in balance with future needs.
With regard to other differences among the sectors, it is easy to understand that competence needs are especially seen to increase in primary health care and services for older people. It may be assumed that primary health care is a natural junction where clients are guided to other services and older people are the ones who use most of the integrated health and social care services. One could argue that a growing proportion of home care for older people, a decreasing proportion of institutional care 21 and caring for people with multimorbidity are main challenges 22 not only in services for older people, but also for primary care and other sectors.
The finding that low co-operation and flow of information are associated with higher competence needs in ensuring service path is generally congruent with previous studies from Finland reporting difficulties in multiprofessional and cross-sectorial collaboration in health care. 23 In this study, those with a lower level of cooperation and flow of information may have recognized the importance of an effective service path in meeting future work requirements better than others. The present findings suggest that multiprofessional collaboration is needed throughout the care chain that further requires advanced interprofessional and teamwork competencies.6–8 The findings revealed a rather clear pattern with regard to differences between some sectors. It can be argued that interprofessional competencies are a key factor in handling differences in professional and organizational cultures and legislation and, therefore, are a prerequisite for successful health and services reform. 1
According to the present findings, those in a superior position saw needs for all competences to increase more than other employees. The findings imply the high risks of the dichotomization of the workforce suggesting that those with a superiority position may have the highest responsibility during the reforms. On the other hand, from the viewpoint of the workforce, the ongoing health and social care reform is a continuous process of changes. Employees have usually experienced the possibilities to influence the reform low. Therefore, the motivation of the workforce regarding the new reform and work changes is the main question. 24
Strengths and limitations
The present study has both strengths and weaknesses. We employed a relatively large data set and several significant background variables could be controlled. The downside is that generalizations derived from the present study could be biased due to low response rate and should therefore be made with caution. It was not possible to collect information on the nonrespondents. However, it is significant to note that low response rates do not necessarily increase nonresponse errors. 25
Secondly, the survey is based on self-assessments, not on objective measures on competencies. Thus, the results should be interpreted with caution. However, some valuable information can only be collected using a questionnaire as was done in the present study.
The noteworthy limitation is also the influence of the Finnish context. The scale concerning the competence and skills seems to be usable among a Finnish social and health sector workforce. Nevertheless, more research in different contexts may help to evaluate the validity in other countries.
The design of the study was cross-sectional. Causal inferences were not possible to be drawn from the results. However, theoretically the question of causality is somewhat irrelevant to the present study. In addition, it should be kept in mind that several details not included in the present study are also related to integration. For example, it was not possible to examine individual professions and associations with integration.
Conclusions
The study points out three dimensions of generic competence needs perceived by employees that are required to secure a client-oriented integrated care process in future. New competencies and targeted processes in organizations and between sectors are crucial in developing the quality and effectiveness of integrated care. Professional education and training should advance the learning of generic competences shared by all professionals and sectors in accomplishing integrated care. Appropriate attitudes, practical skills, and assumed responsibilities play an important role in building client-centered care. It is important to specify these competency requirements in curricula and take them into account in advancing further education and training.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was conducted in Competent Workforce for the Future-Project (No. 303605, 303608) funded by the Strategic Research Council (SRC) at the Academy of Finland.