
Abstract
Up to 70% of menopausal women report musculoskeletal (MSK) pain during and after the time of menopause. This observation suggests oestrogen deficiency may play a role in the development of MSK pain and conditions which cause it. Therefore, we hypothesise that hormone replacement therapy (HRT) will improve these symptoms; however, there is currently no guidance on the use of HRT for such symptoms. This review aims to synthesise current evidence on the associations between HRT and chronic MSK pain in menopausal women, to help guide clinical practice. MEDLINE, EMBASE, AMED, CINAHL, PsycINFO, Cochrane and Web of Science databases were searched from their inception to October 2024. The search initially identified 30,739 studies from which 57 studies, including a total 3,958,702 participants, were included. MSK outcomes were grouped into generalised MSK pain, osteoarthritis (OA), rheumatoid arthritis (RA), gout and carpel tunnel syndrome (CTS). Pooled analysis found no significant effect of ever HRT use versus never HRT use on generalised MSK pain (RR 1.00, 95% CI 0.96–1.04). For OA and RA outcomes significant heterogeneity between studies restricted our ability to undertake pooled analysis. Narrative synthesis of these outcomes revealed conflicting results on the effect of HRT on these conditions. This systematic review and meta-analysis demonstrates the substantial heterogeneity within this field and highlights the need for bespoke studies investigating the effect of HRT on MSK pain to draw any firm conclusions to guide clinical practice.
Keywords
Introduction
Menopause, defined clinically as the permanent cessation of menstruation due to the loss of follicular function, is a universal experience for women living beyond midlife. 1 The associated decline in oestrogen levels results in a plethora of symptoms including hot flushes, mood changes, cognitive dysfunction, sleep disturbance, fatigue, reduced libido and musculoskeletal (MSK) pain. While vasomotor symptoms (hot flushes and night sweats) have traditionally been regarded as the hallmark features of menopause, recent evidence suggests MSK pain is nearly as prevalent, affecting over 70% of women at the peak of menopause. 2
Emerging research indicates strong sex-based disparity in MSK disorders, with women experiencing higher rates of arthralgia and arthritis than men. 3 These differences become particularly pronounced during the menopausal transition, suggesting a potential link between oestrogen deficiency and the development and progression of such conditions. For example, the incidence of osteoarthritis (OA) rises exponentially in women over men at the age of menopause.4,5 Furthermore, oestrogen is known to exert anti-inflammatory and immunosuppressive effects, hence associations with new onset inflammatory conditions such as rheumatoid arthritis (RA) during and after menopause. 6 However, not all pain experienced during the menopause can be directly attributed to oestrogen deficiency. Joint and muscle pains can be related with fatigue, mood, sleep disturbance, and elevated Body Mass Index. The menopause is therefore likely to trigger and drive chronic pain syndromes.
MSK pain represents a substantial burden on both individual wellbeing and the economy. The global prevalence of OA among postmenopausal women has increased 1.3-fold in three decades 7 and MSK pain remains one of the most frequent reasons for primary care consultations. 8 Despite this, there are no comprehensive systematic reviews and meta-analyses examining the use of HRT for MSK symptoms in menopausal women.
The uptake of HRT has increased in recent years, perhaps due to increased awareness of menopause and associated campaigns. Currently the National Institute for Health and Care Excellence (NICE) only recommends HRT for the treatment of vasomotor symptoms, depression and altered sexual function. 9 However, anecdotal reports and preliminary studies suggest that HRT may be beneficial for the MSK complaints,4,10,11 although such evidence is conflicting.12–14
The high prevalence, complex aetiology, and substantial personal and societal costs of MSK pain in menopausal women highlights the need to evaluate whether HRT may offer meaningful therapeutic benefit to these women. This review aims to synthesise current evidence on the associations between HRT and chronic MSK pain in menopausal women.
Methods
This systematic review and meta-analysis was registered with the International Prospective Register of Systematic Reviews (PROSPERO) database (CRD42023467911) and is reported in accordance with Preferred Reporting Items for Systematic Review and Meta-analyses (PRISMA) 2020 guidelines. 15
Search strategy
A systematic search, developed with input from information specialists, of seven databases (MEDLINE, EMBASE, AMED, CINAHL, PsycINFO, Cochrane and Web of Science) from their inception to October 2024 was conducted. Searches utilised text word searching in the title, abstract and key words, along with database subject headings. The detailed search strategy for each database can be found in the supplemental materials. The search was extended by screening reference lists of existing systematic reviews related to this topic. There were no restrictions on study setting or language, and interpreters were utilised where possible. This search was conducted in tandem with another sister review exploring the prevalence and experience of MSK pain in menopausal women.
Study selection
Results were imported into Endnote X9 (https://endnote.com/) where duplicates were removed. Remaining unique references were uploaded to Rayyan software (https://www.rayyan.ai/cite/) to complete the screening process.
Title, abstract and full text screening were conducted independently by two reviewers (from RO, PA, AC, SR, VW, CB). Discordance between reviewers was resolved by team discussion or a third reviewer. Studies included reported the effects of non-contraceptive hormone replacement on outcomes relating to MSK pain in menopausal women. Observational studies specifically reporting outcomes relating to chronic and painful MSK conditions because of untreated menopause were excluded and analysed separately in a sister review. Studies were excluded if the intervention was an alternative menopause therapy, there was no full text available or no translation to English available. Secondary evidence, conference abstracts and unpublished studies were excluded.
Data extraction
Data extraction was conducted by one reviewer and independently verified by a second reviewer. Any disagreements were resolved through discussion and, if necessary, adjudication by a third reviewer. Data was extracted into a pre-piloted table, including author, year of publication, setting (country and healthcare setting), study design, study aim, funding, sample size, age, definition of menopause, painful condition and definition, details of comparator group, outcome measure(s) including measurement tools, duration of follow-up and measures of association.
Risk of bias assessment
Risk of bias was assessed by two investigators using the Joanna Briggs Institute critical appraisal tool (https://jbi.global/critical-appraisal-tools) appropriate for the study type. Results of the checklists were used to categorise studies as high (<50%), moderate (50–70%) or low (>70%) risk of bias. Studies were not excluded based on quality assessment.
Synthesis of results
Studies were grouped into those that reported generalised joint and muscle pain, knee OA, hip OA, hand OA, RA, gout and carpal tunnel syndrome (CTS). A narrative synthesis was carried out for all groups of studies, with meta-analysis to estimate the pooled effect of HRT on specific painful MSK conditions, where meaningful.
Statistical analysis
We performed a meta-analysis of randomised controlled trials to estimate pooled risk ratios (RRs) for positive outcomes in two groups using the meta package in R. Between-study variance was estimated with restricted maximum-likelihood, and both common-effect and random-effects models were fitted. Heterogeneity was assessed with I2, τ2, and Cochran’s Q test, and results were presented in forest plots with study-level RRs, 95% confidence intervals, and weights. All analyses were done using R programming software version 4.5.1.
Results
Characteristics of the included studies
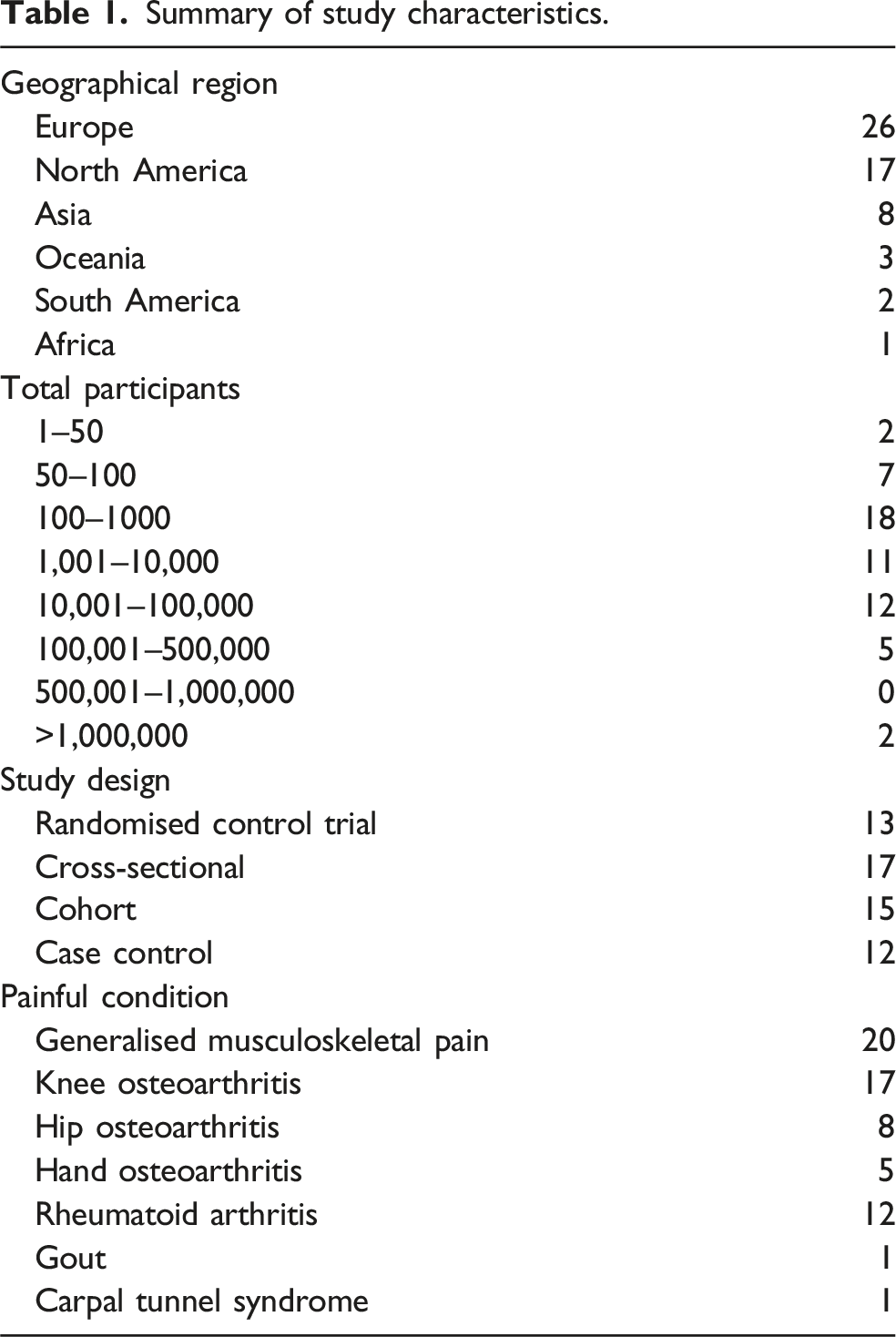
The results of the literature search up to final search are illustrated in Figure 1. The search identified 30,739 studies, of which 57 studies met the inclusion criteria, including a total 3,958,702 participants. Of the 57 studies included, 13 were randomised controlled trials (RCTs), 17 cross-sectional studies, 15 cohort studies, and 12 case control studies (Table 1). PRISMA Diagram. WHO, World Health Organization. Summary of study characteristics.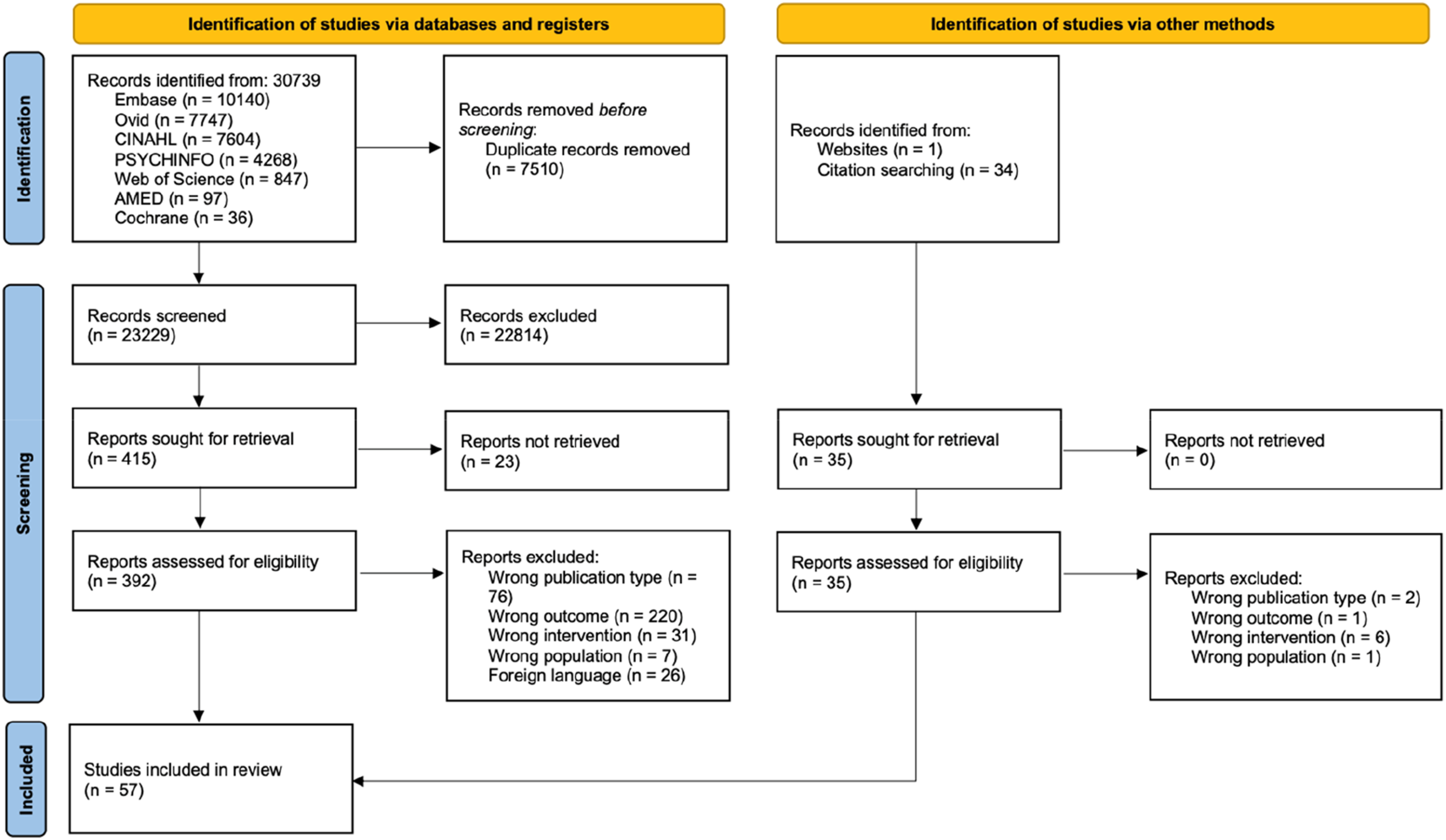
Association between HRT and generalised MSK pain
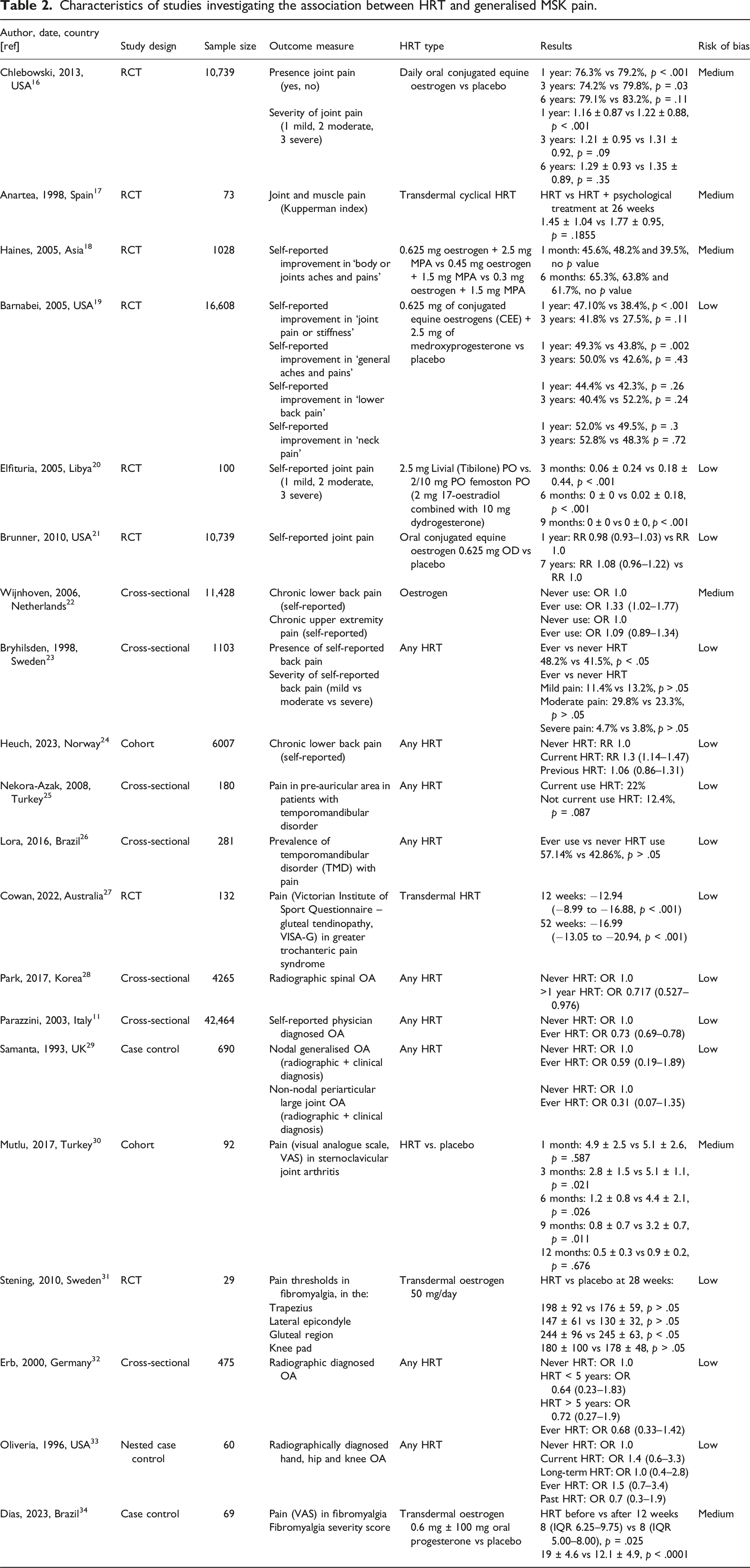
Characteristics of studies investigating the association between HRT and generalised MSK pain.
Meta-analysis was conducted including all studies which evaluated MSK pain as a binary (yes/no) variable. Pooled analysis indicates a statistically significant reduction in MSK pain in HRT users versus never HRT users using the common-effects model (RR = 0.95, 95% CI 0.92–0.98) but not when using the random-effects model (RR = 0.76, 95% CI 0.56–1.03). The plot indicates a high heterogeneity among the studies (I2 = 90%, p < .01) suggesting most of the variation in the study results are due to the differences between the studies rather than by random chance (Figure 2). The pooled results of the relationship between HRT and MSK pain. RR = risk ratio.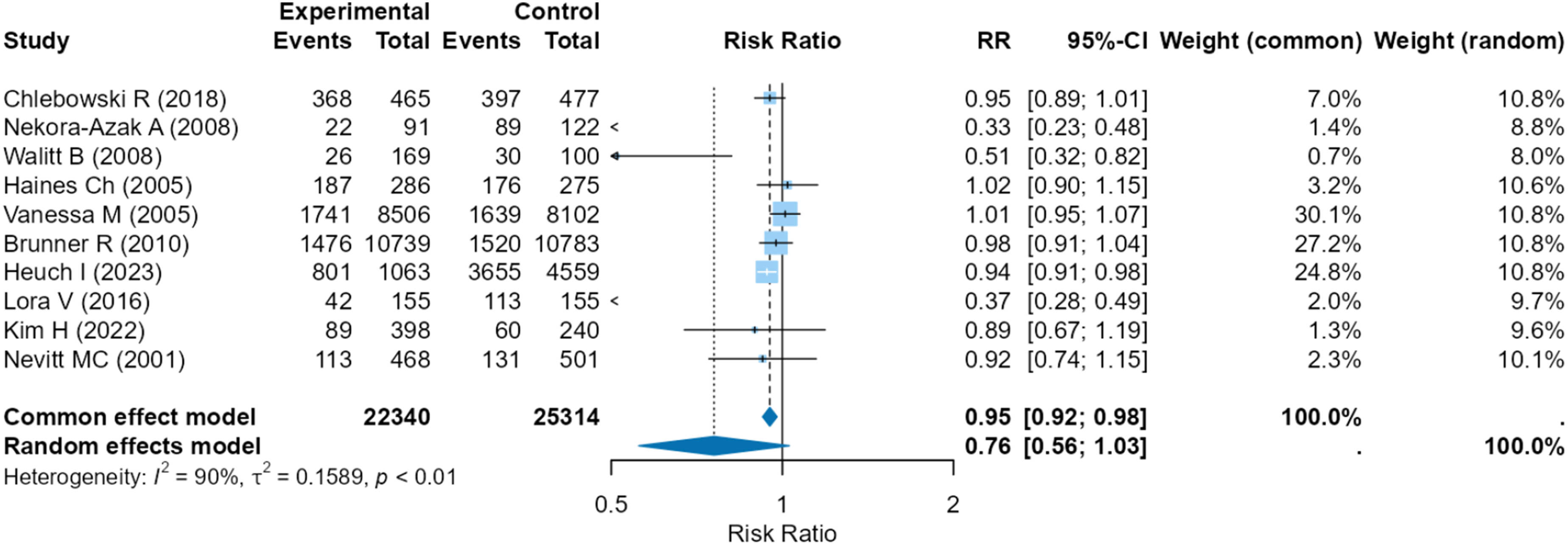
To reduce heterogenicity, a sensitivity analysis was conducted using just RCTs (I2 = 51%, p = .07). Pooled analysis indicated no benefit in MSK pain in HRT users versus never users according to the random-effects model (RR 0.98, 95% CI 0.95–1.02) (Figure 3). The pooled results of the relationship between HRT and MSK pain using RCTs only.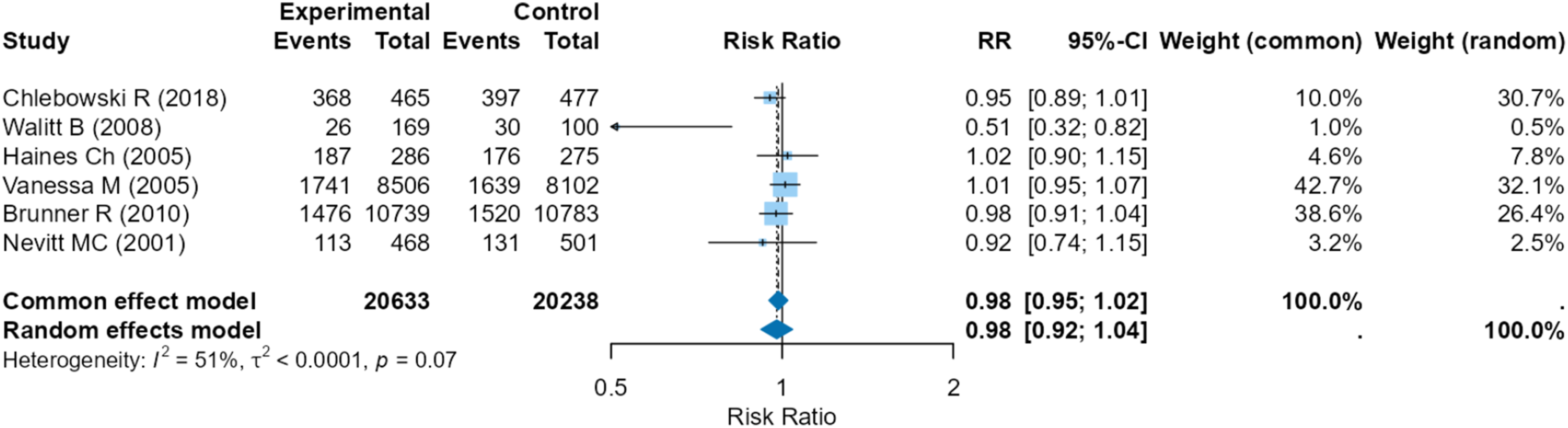
Association between HRT and knee osteoarthritis
Characteristics of studies investigating the association between HRT and knee OA.
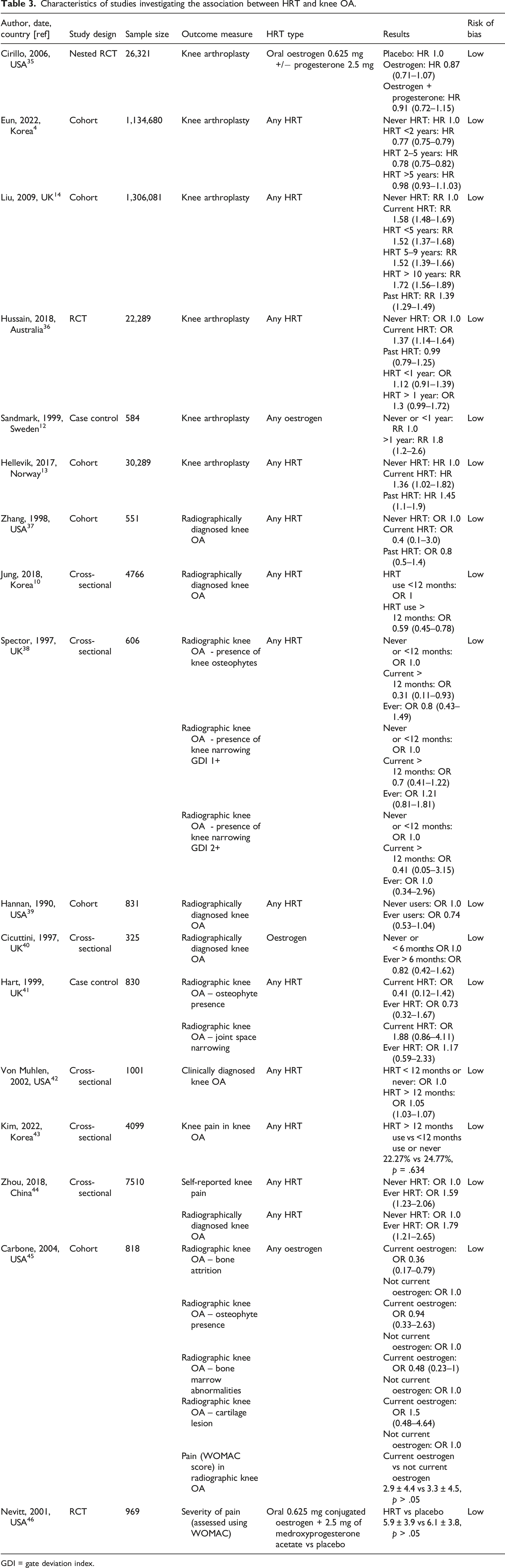
GDI = gate deviation index.
Eight studies reported the association between HRT and radiographic knee OA.10,37–41,44,45 Zhou et al. (2018) reported a positive association between ever use of HRT and radiographic diagnosed knee OA (OR 1.79, 1.21–2.65). Four studies found no association between HRT use and radiographic knee OA.39–41,47 Two studies reported a negative association between HRT use and bone attrition 45 and osteophyte presence 38 but otherwise no association between HRT and other X-ray features including joint space narrowing, bone marrow abnormalities and cartilage lesions. One study found a negative association between HRT use and radiographic knee OA. 10
One study 42 reported on clinical diagnosis of knee OA and found a mild positive association between use of HRT >12 months compared to <12 months or never (OR 1.05, 1.03–1.07).
Four studies reported the association between knee pain in participants with known knee OA and HRT use. Three studies found no association between HRT use and reported knee pain in knee OA.43,45,46 One study, Zhou et al. (2018), found a positive association between self-reported knee pain and ever use of HRT (OR 1.59, 1.23–2.06).
Association between HRT and hip osteoarthritis
Characteristics of studies investigating the association between HRT and hip OA.
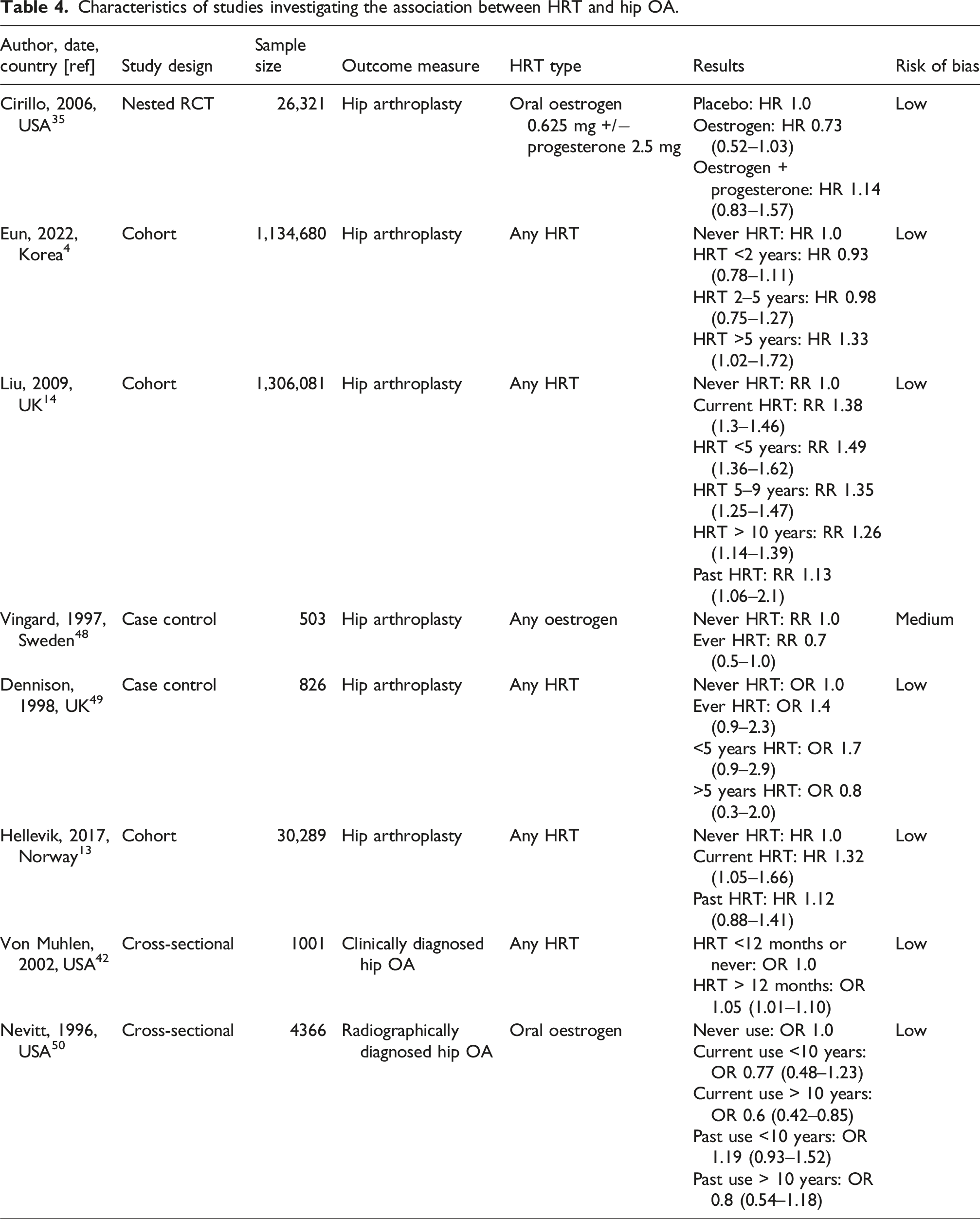
One study 42 observed the relationship between HRT and clinically diagnosed hip OA. They reported postmenopausal oestrogen use >12 months is associated with an increased risk of hip OA compared to < 12 months use or never use (OR 1.05, 1.01–1.10). One study 50 observed the relationship between HRT and radiographic Hip OA. Nevitt et al. (1996) reported that current use of oral oestrogen ≥ 10 years was associated with a reduced risk of grade 2–4 hip OA (OR 0.77, 0.48–1.23). There was no association between current use of oral oestrogen < 10 years and grade 2–4 (OR 0.77, 0.48–1.23). There was no association between past use of oestrogen and hip OA.
Association between HRT and hand osteoarthritis
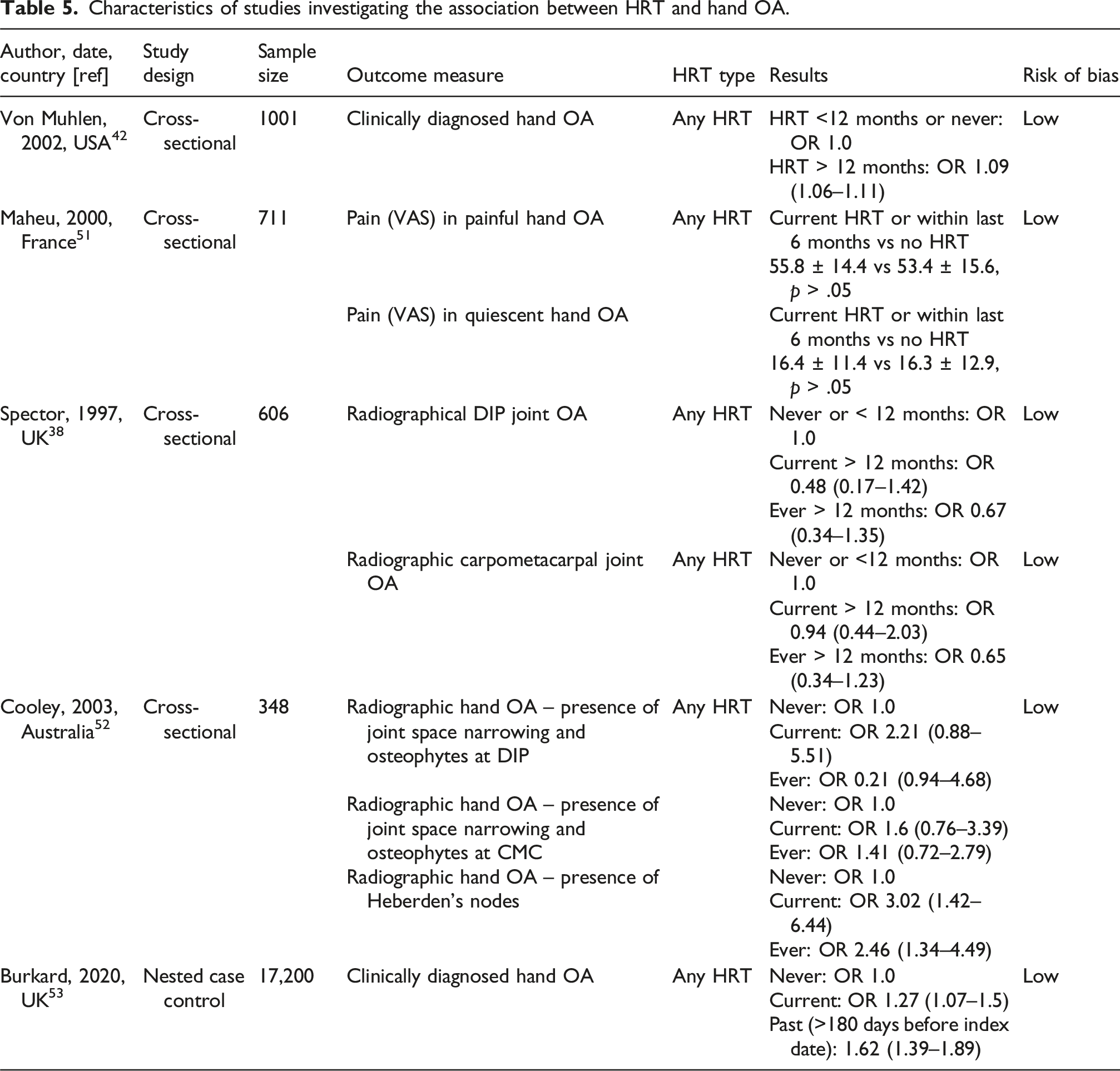
Characteristics of studies investigating the association between HRT and hand OA.
Association between HRT and rheumatoid arthritis
Characteristics of studies investigating the association between HRT and RA.
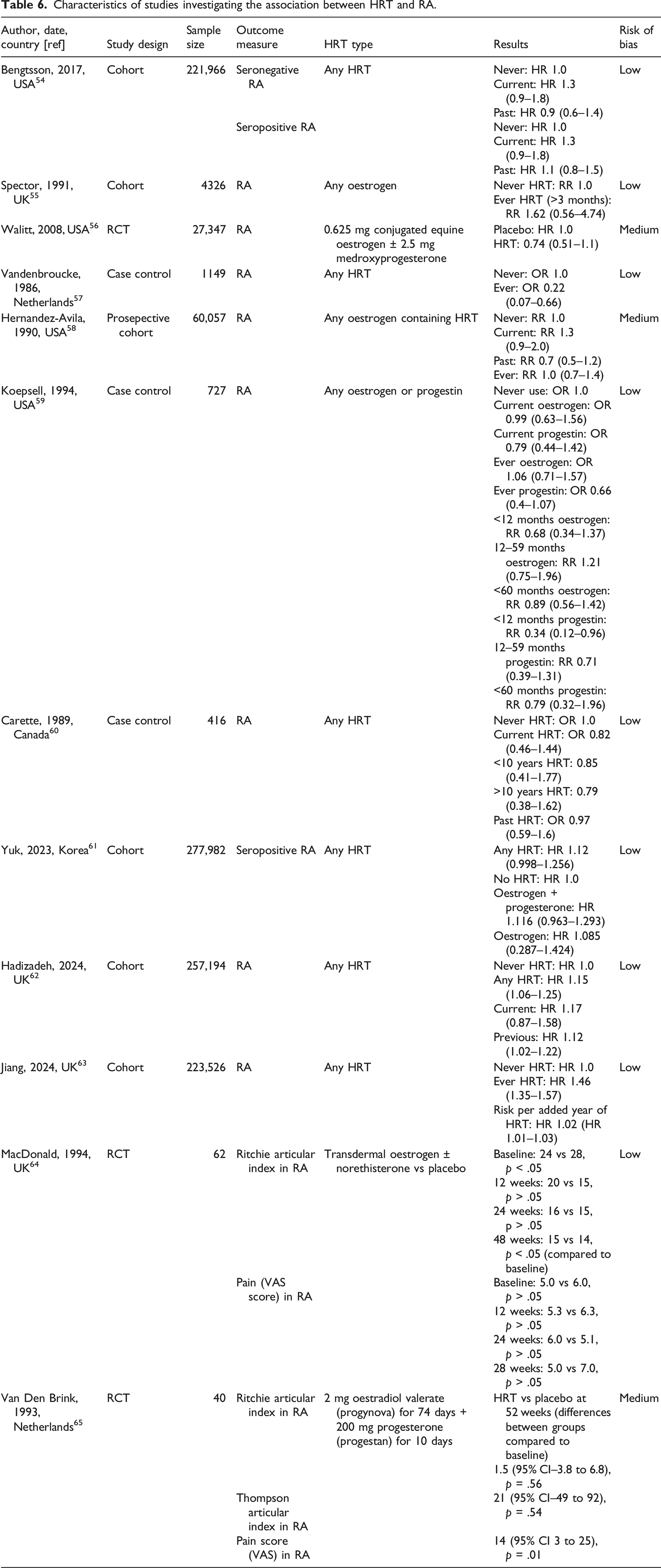
Two studies reported pain and stiffness outcomes in patients with pre-existing RA.64,65 Van Den Brink et al. (1993) found no effect of 1 year of HRT on joint pain, stiffness and swelling in patients with RA. MacDonald et al. (1994) found a statistically significant improvement in subjective overall wellbeing week 12 and 48 (p < .05 from baseline) and in the Ritchie articular index by week 48 of the study (p < .05 from baseline). However, neither Macdonald et al. or Van Den Brink et al. (1993) found any change in ESR levels following one year of HRT.
Association between HRT and gout
One study reported the association between HRT and the incidence of self-reported physician diagnosed gout. 66 Hak et al. found current use of HRT was protective against gout (RR 0.81, 0.7–0.94). There was no significant effect of previous HRT use on incidence of gout RR 1.04 (0.89–1.2) or the duration of postmenopausal hormone use among current users (p = .37).
Association between HRT and carpal tunnel syndrome
One study reported the association between HRT use and the prevalence of CTS. They reported ever users of HRT had a significantly increased risk of CTS compared to never users (OR 2.72, 2.56–2.88). 67
Discussion
The aim of this systematic review and meta-analysis was to assess the association between HRT and MSK pain, to help guide clinical practice. MSK conditions assessed included OA, RA, generalised MSK pain, fibromyalgia, gout and CTS. Overall, the evidence does not demonstrate a significant effect of HRT on MSK pain.
With recent reports highlighting the increasing burden of OA on menopausal women we hoped to draw conclusion on the effect of HRT on this condition. Thirty studies investigated the association between HRT and OA, but findings were inconsistent and contradictory. This mirrors earlier systematic reviews and meta-analyses, which have reported both positive63,66 and negative 67 associations between HRT use and OA. This may be attributable to the heterogenicity in HRT formulation and duration, as well as its complex interplay with other menopausal factors, which may act as confounders and limit the ability to draw robust and reliable conclusions.
In the subgroup analysis of generalised MSK group, including non-specific joint and muscle pain, we hypothesised that HRT would improve pain outcomes given the therapeutic benefits on mood, sleep disturbance and fatigue. A greater understanding of relevant physiological pathways including oestrogen’s modulation of inflammatory cytokines, nociceptive signally, and cartilage metabolism may help clarify these findings and should be explored in future research.
Notably, this is the first systematic review to evaluate the association between HRT and RA. With recent evidence illustrating that postmenopausal women had a 35% increased risk of developing RA compared to pre-menopausal women 6 we hypothesised that HRT would be associated with a reduced incidence and improve symptom control in patients with established RA. However, of the 10 studies examining the effect of HRT on incidence of RA only one found a reduced incidence, whilst seven found no effect and two found HRT in fact increased the incidence of RA. One explanation for this observation is detection bias: women on HRT are more likely to be engaging regularly with healthcare services and therefore have a greater likelihood of receiving a RA diagnosis. Although some studies observed improvements in subjective wellbeing with HRT use, this was not reflected in objective markers of disease activity (e.g. platelet count, ESR or CRP) 58 further supporting that HRT may not be directly influencing disease pathophysiology to improve symptoms.
The strengths of this systematic review and meta-analysis include its comprehensive scope and large sample size, which exceed that of previous reviews in this field. However, important limitations must be acknowledged. Crude data was preferentially used to ensure consistency across studies, reduce reporting bias and improve the accuracy of pooled estimates. However, for some studies included in this review the crude data directly contradicted the adjusted data. 30 Therefore, known confounding variables such as obesity and age have been carried through to the results of this review and may reduce the reliability of results presented here. Furthermore, the heterogeneity in study designs, HRT uses and diagnostic methods precluded robust meta-analysis in several domains. Because of this, it was preferrable to avoid pooling data and instead divide studies into smaller groups for best evidence synthesis.
This review highlights the necessity to standardise outcome measures and control variables to facilitate pooled analysis which could be used to guide clinical practice. The most significant source of heterogeneity between studies was the inconsistent classification of HRT exposure. For example, some studies included 6–12 months of HRT use with the ‘never users’ of HRT category, whilst others classed participants as users of HRT based on a single prescription of HRT. Given that even 8 weeks of HRT use can significantly increase oestrogen levels 24 we recommend future studies reserve ‘never users’ of HRT for those who have never received postmenopausal HRT. Similarly, we found studies had a varied definition of menopause including the date of the last period, 6- or 12-months amenorrhoea. We would recommend menopause be standardised within all future research as date of last menstruation, as stated by the NICE guidance 9 and the World Health Organisation. 68 Furthermore, we recommend greater consistency in defining HRT formulations (e.g. oestrogen-only, oestrogen + progesterone, and progestin) and utilising standardised diagnostic criteria or recognised symptom scores for MSK conditions.
Conclusion
Despite the large volume of literature examining the association between HRT and MSK health, it is not possible to draw any firm conclusions regarding the effect of HRT in this population. This systematic review and meta-analysis demonstrates the vast heterogeneity within this field and highlights the need for standardised studies looking at the effect of HRT on MSK pain to draw any firm conclusions.
Supplemental Material
Supplemental Material - The effect of hormone replacement therapy on musculoskeletal pain in menopausal women: A systematic review and meta-analysis
Supplemental Material for The effect of hormone replacement therapy on musculoskeletal pain in menopausal women: A systematic review and meta-analysis by Rachel Overton, Payam Amini, Adam Chew, Opeyemi Babatunde, Kayleigh Mason, Sneha Rathod, Victoria Welsh, and Claire Burton in Post Reproductive Health.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Contributorship
Study protocol: SR, CB, OB, RO.
Data extraction: CB, RO, PA, AC, VW.
Statistical analysis: PA, KJM.
Paper writing: RO.
Final approval of article: all authors.
Guarantor
RO.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.