
Abstract
Menopausal symptoms are known to affect quality of life and work productivity. This systematic review aimed to describe the range and effectiveness of workplace-based interventions for menopause. MEDLINE, PubMed, Embase, CINAHL, Cochrane Library, Web of Science, PsycINFO, EconLit, and SCOPUS were searched from the inception until April 2022. Quantitative interventional studies evaluating physical/virtual workplace-based interventions aiming to improve well-being, work, and other outcomes, that involved women in menopausal transition, or their line managers/supervisors were eligible for inclusion. Two randomized controlled trials and three uncontrolled trials, comprising 293 women aged 40–60 years and 61, line managers/supervisors, were included in the review. Results were narratively synthesized due to the heterogeneity of interventions and outcomes and we found that only a limited range of interventions have been evaluated for their ability to support women going through menopausal transition in the workplace. Self-help cognitive behavioural therapy (CBT); Raja yoga; and health promotion (involving menopause consultations, work–life coaching and physical training) improved menopausal symptoms significantly. Self-help CBT was associated with a significant improvement in mental resources for work, presenteeism, and work and social adjustment. Awareness programs significantly improved knowledge and attitudes of both employees and line managers/supervisors about menopause. The interventions have mostly been evaluated in small studies with selected populations but have improved menopausal symptoms and work outcomes. A customizable menopause wellbeing intervention package incorporating these evidence-supported interventions should be developed and implemented on a wider scale within organizations alongside robust evaluation of its effectiveness.
Introduction
Menopausal transition is a physiologically and psychosocially challenging period in a woman’s life. Occurring between the ages 45-55 years, transition from reproductive phase to menopause could take 4–8 years and is characterised by irregular or prolonged menstrual cycles and menopausal symptoms. Menopausal symptoms are vasomotor (hot flushes, night sweats), somatic (fatigue, insomnia, body aches, joint pains), psychosocial (poor concentration, forgetfulness, low mood, anxiety, and low confidence), sexual (decreased libido and sexual responsiveness), and urogenital (vaginal dryness and atrophy). They could last up to 5 years into menopause or may even worsen and persist into the latter stages of life.1–3
Menopausal symptoms interfere with day-to-day activities of women including employment.4–6 Poor concentration, tiredness, and poor memory have been reported in around 50% of women aged 45–55 in professional, managerial, and administrative roles. 4 Sleep problems during menopause have been associated with approximately half an hour reduction in work time per week and an annual loss of $2.2 billion of productivity per year. 7 A study on self-perceived ability to perform in the job currently and for the next 2 years, reported that almost one third of female workers in the health sector were concerned about reduced work ability during menopause. 8 Half of employed women at 50 years of age are more likely to retire or work fewer hours per week due to distressing menopausal symptoms. 9
Increased life expectancy has increased the age of retirement of women with the majority remaining in employment during and after menopausal transition. Most women expect their employers to know, communicate and be helpful during menopausal transition and to have workplace policies concerned with their overall wellbeing. They report difficulties working in poorly ventilated workplaces and that provision of cool water and rest facilities will improve their quality of work life.10,11 A review of guidance on menopause at workplaces reports that the available guidelines broadly focus on legislation, policies, information and training, workplace support, and the physical work environment. 12 The European Menopause and Andropause Society (EMAS) recommends health and wellbeing during menopause to be given a higher level of attention at the workplace by creating awareness, alleviating stigma, allowing flexible work schedules, dress codes, and controlling the physical environment. 13
Interventions to enhance the wellbeing of menopausal women include lifestyle modification, complementary and alternative medicines, and hormone replacement therapy. 14 There is a growing interest in potential workplace-based interventions to improve wellbeing and employment outcomes among menopausal women.15–17 These interventions could support women through physical and psychosocial stressors at workplaces and thereby improve the quality of work life. 11 The objective of this systematic review was to describe the range and effectiveness of workplace-based interventions in supporting women during the menopausal transition and to make recommendations for future interventions.
Methods
This review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses: PISMA 2020 statement. 18 The protocol is registered with the International Prospective Register of Systematic Reviews (PROSPERO) under the registration ID CRD42022308412.
Search strategy
Bibliographic databases MEDLINE (via Ovid), PubMed, Embase, CINAHL, Cochrane Library, Web of Science, PsycINFO, EconLit and SCOPUS were searched from inception date until April 2022, without any language restrictions. The search strategy was developed with input from a librarian using the keywords: (menopaus* OR menopausal transition OR climacteric OR middle-aged women OR perimenopaus* OR post-menopaus*) AND (work* OR workforce OR employ* OR workplace* OR occupation*) AND (adapt OR support* OR promote* OR prevent* OR intervention* OR program* OR experiment OR trial). The reference lists of selected papers were searched for any relevant studies.
Inclusion exclusion criteria
Quantitative randomized control trials (RCT), non-RCT, or uncontrolled trials evaluating any workplace-based interventions for women in menopausal transition, or their employers/mangers were eligible. The studies were included if the interventions aimed to improve physical and/or mental wellbeing, work outcomes, or awareness and attitudes among participants. Both physically and virtually conducted interventions were included. Community and clinic-based interventions and pharmacologic interventions such as HRT were excluded.
Outcomes
Primary outcomes related to physical and mental wellbeing, including menopausal symptoms and quality of life. Secondary outcomes related to the job e. g work ability, social support at work, presenteeism/absenteeism, and work stress. A third set of outcomes related to workplace culture such as awareness, attitudes, and behaviours towards menopause at work.
Selection of studies
Titles, abstracts, and full texts were screened for eligibility by two reviewers (CHR and ES) and any disagreements were resolved through discussion with another reviewer (SB). Articles were screened using Rayyan software.
Data extraction
Data were extracted using a data extraction form by two reviewers (CHR and ES) separately and compared for consistency. The extracted data included details on the setting, study population, inclusion/exclusion criteria, number of participants in intervention and control groups, outcomes, and number with each outcome. If a study had more than one publication, the publication with the larger sample or the publication including quantitative data was included. Study authors were contacted if further data was required.
Study quality
As both randomised and non-randomised studies were included, the Downs and Black checklist 19 was used to assess reporting, risk of bias, confounding, external validity, and the power of included studies. Study quality was assessed by two reviewers (CHR and ES) independently and any disagreements were settled by discussion with the third reviewer (SB). To make the scoring of the tool easier, the power sub-scale in the original checklist was interpreted as “reported” or “not” and this score was added to the “reporting” sub-scale. 20
Data synthesis
Due to the heterogeneity of included interventions and outcomes measured between studies, a meta-analysis was inappropriate, and data were narratively synthesized. Studies were grouped by study design and type of outcome measure.
Results
Selection of studies
The primary search provided 952 results. Following removal of duplicates and irrelevant titles, 79 articles were retained for abstract screening. Out of them 11 articles were selected for full-text screening. The full text screening excluded six studies because they did not meet the inclusion criteria: three qualitative studies,21–23 a secondary analysis of a larger community-based study,
24
and two clinic-based studies.25,26 The remaining five articles were included in the narrative synthesis. Figure 1 illustrates the study selection process. Study selection process and results.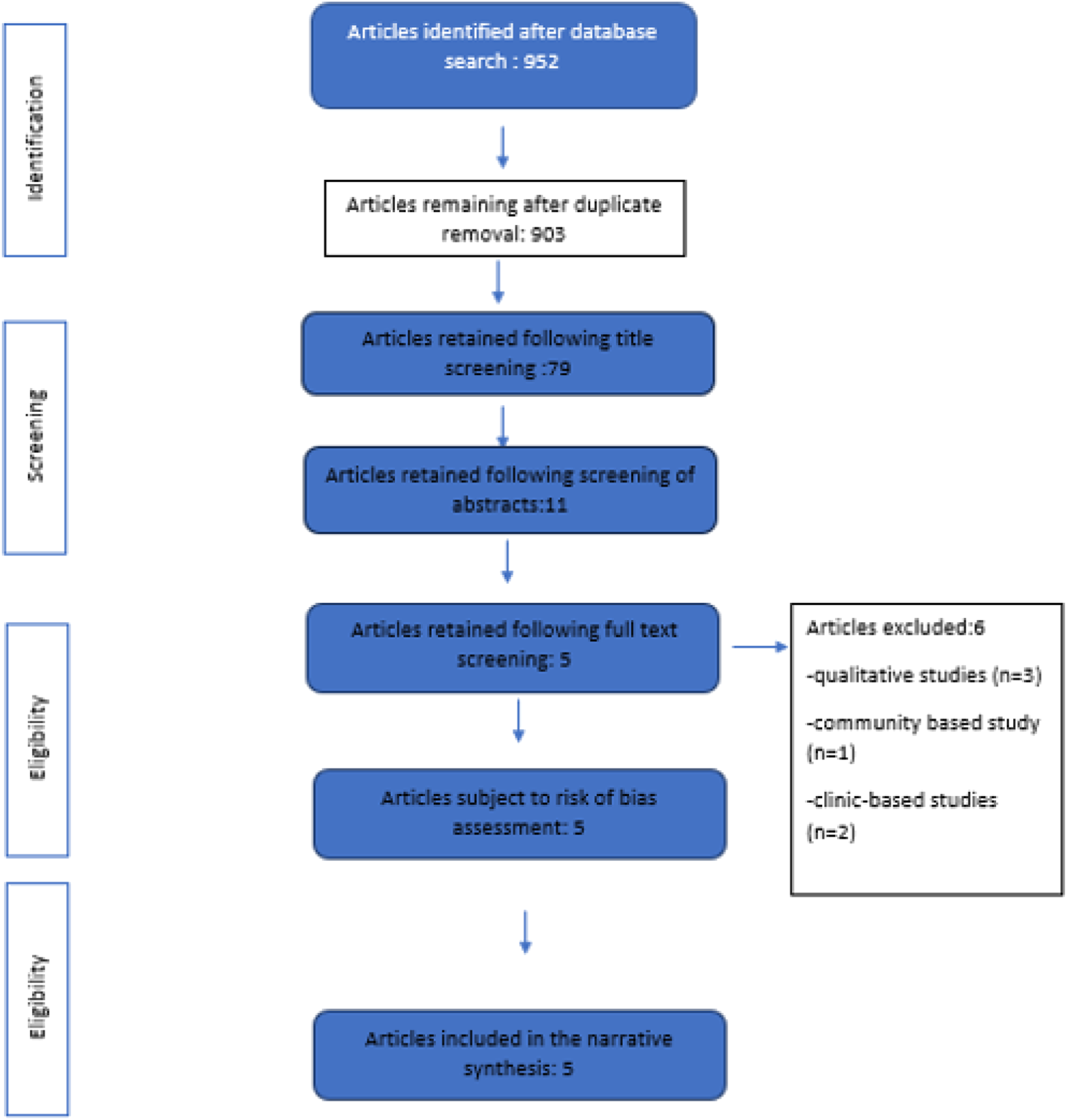
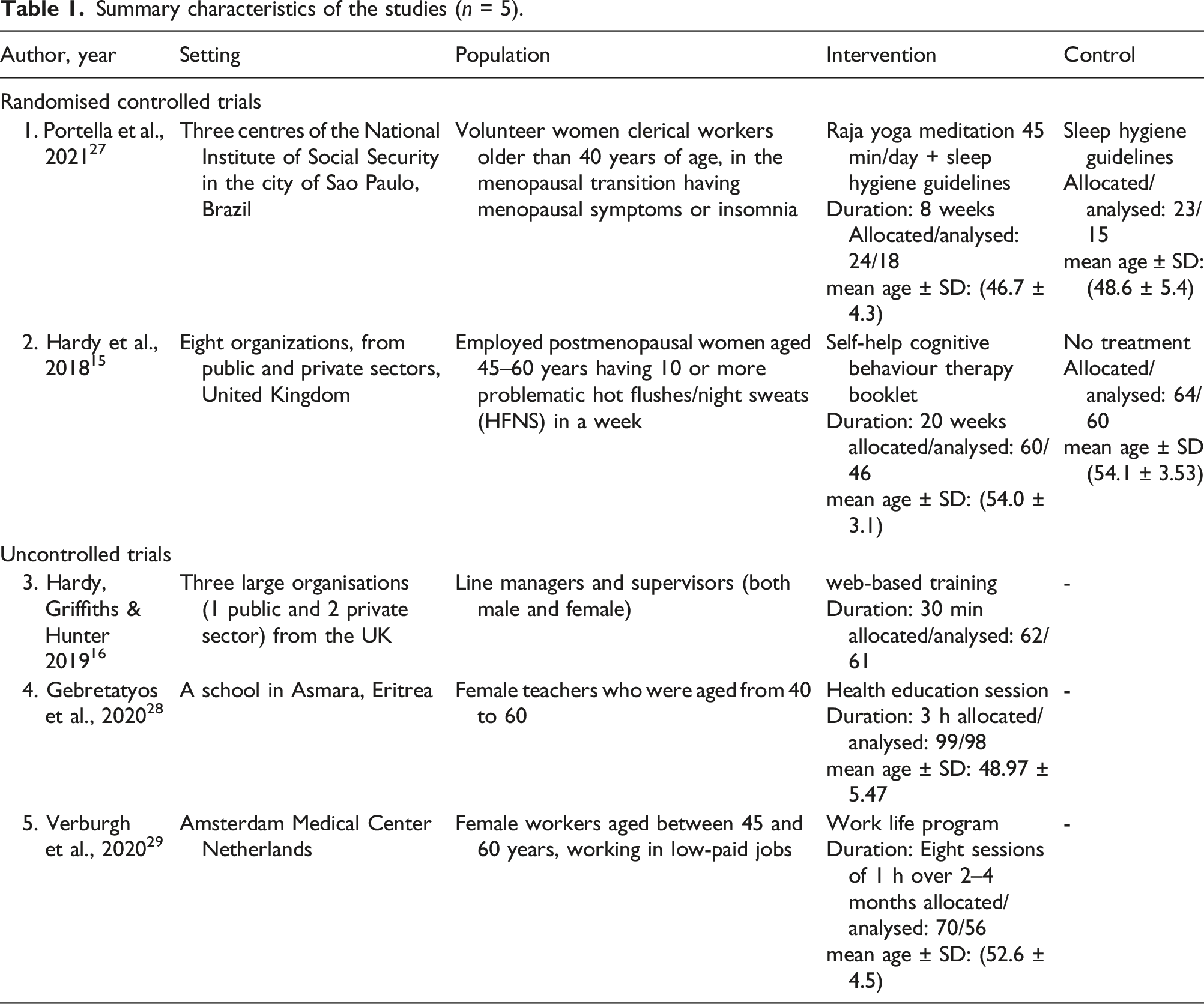
Study characteristics and quality
Summary characteristics of the studies (n = 5).
Summary of the quality of studies using Downs and Black tool a (n = 5).
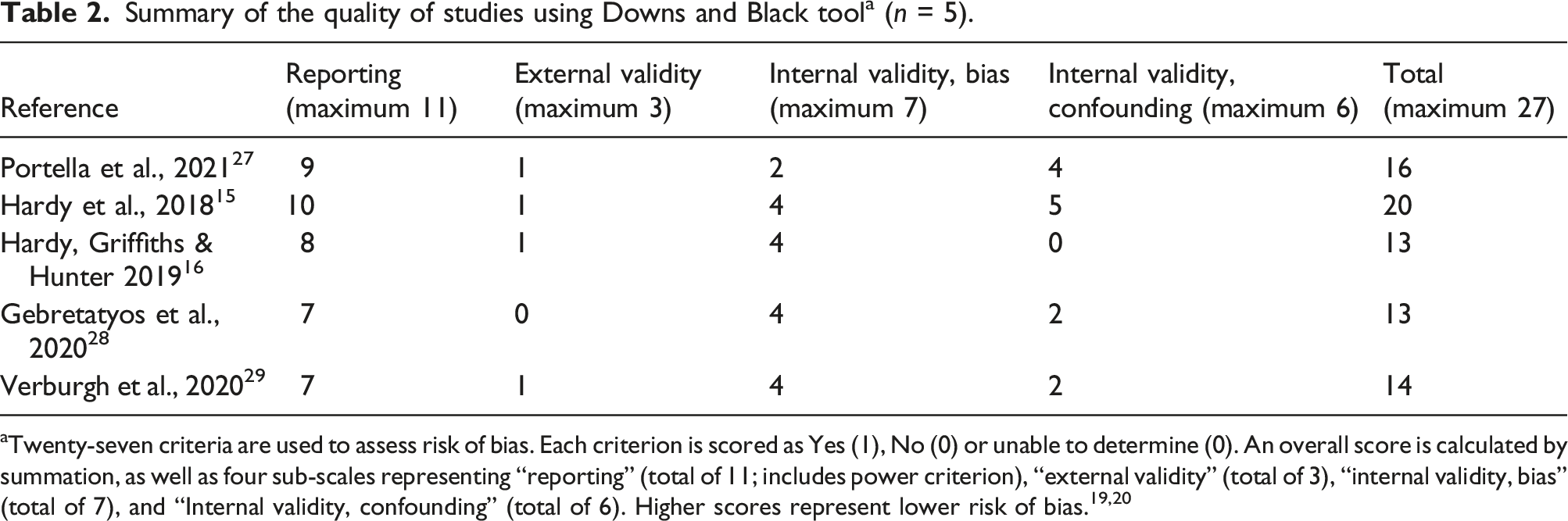
aTwenty-seven criteria are used to assess risk of bias. Each criterion is scored as Yes (1), No (0) or unable to determine (0). An overall score is calculated by summation, as well as four sub-scales representing “reporting” (total of 11; includes power criterion), “external validity” (total of 3), “internal validity, bias” (total of 7), and “Internal validity, confounding” (total of 6). Higher scores represent lower risk of bias.19,20
Interventions
Randomized Controlled Trials
Raja yoga meditation by Portella et al., focused on breathing and relaxation. After the introductory session participants were instructed to do the intervention for 45 min daily for 8 weeks at home and were followed up. The drop out rate was 16.6% (n = 4) from intervention and 21.7% (n = 5) in control group. 27 Self-help CBT by Hardy et al., was delivered via a mailed booklet which has been adapted from a previous community-based trial. 30 It included information and exercises about menopause, stress management, and cognitive and behavioural strategies, and was expected to be completed within 20 weeks. Completion rate was 65% (n = 28) at 20 weeks with self-reported use of breathing technique by 79% (n = 33) at least >1 time per week. 15 The booklet was rated as helpful by 88.1% (n = 35) to cope with problems faced at work and life in general by 63%.
Uncontrolled trials
Hardy et al. had recruited line managers/supervisors from three UK organizations for a short online training on menopause which contained videos, role plays, and real-life testimonials on menopause. Participation rate was 22.9% (62 out of 270 invited) and were followed up for 4 weeks. More than 90% found the intervention helpful. 16 In the intervention by Gebretatyos et al., a group of middle-aged school teachers (n = 99) were provided a group discussion-based training on menopause, physical activity, and nutrition by a midwife. The participation rate was 90% (n = 99). 28 The intervention implemented by Verburgh et al., was an adaptation of a pre-existing Work Life Program (WLP)21,29 and had multiple components: menopause consultations, work–life coaching sessions and physical training sessions. Participants consisted of food service assistants, service desk employees, and cleaners at a teaching hospital. Out of the recruited 80% participated until the end of intervention.
Outcomes
Randomized Controlled Trials
Menopausal symptoms
Self-help CBT significantly improved hot flushes and night sweats (p = 0.01), somatic symptoms (p = 0.01), and sleep problems (p = 0.001). 15 Raja Yoga significantly improved menopausal symptoms (p = 0.026) but did not to show a significant impact on insomnia and sleep quality. 27
Work outcomes
Self-help CBT intervention assessed work outcomes and reported significantly improved presenteeism (p = 0.001) (defined as “perceptions of being physically present at their jobs but experiencing decreased productivity and below-normal work quality due to their menopause”) and work and social functioning (p = 0.01) 14 at home, work, and other social situations.
Other outcomes
There was a significant improvement (p = 0.05) in well-being following self-help CBT. 14 The women reported having better awareness, taking better personal care, and improved confidence to talk about menopause following the intervention. Over one third (37%) had talked to their line manager about any menopause related problems by the time program was evaluated.
Uncontrolled trials
Summary of intervention outcomes (n = 5).
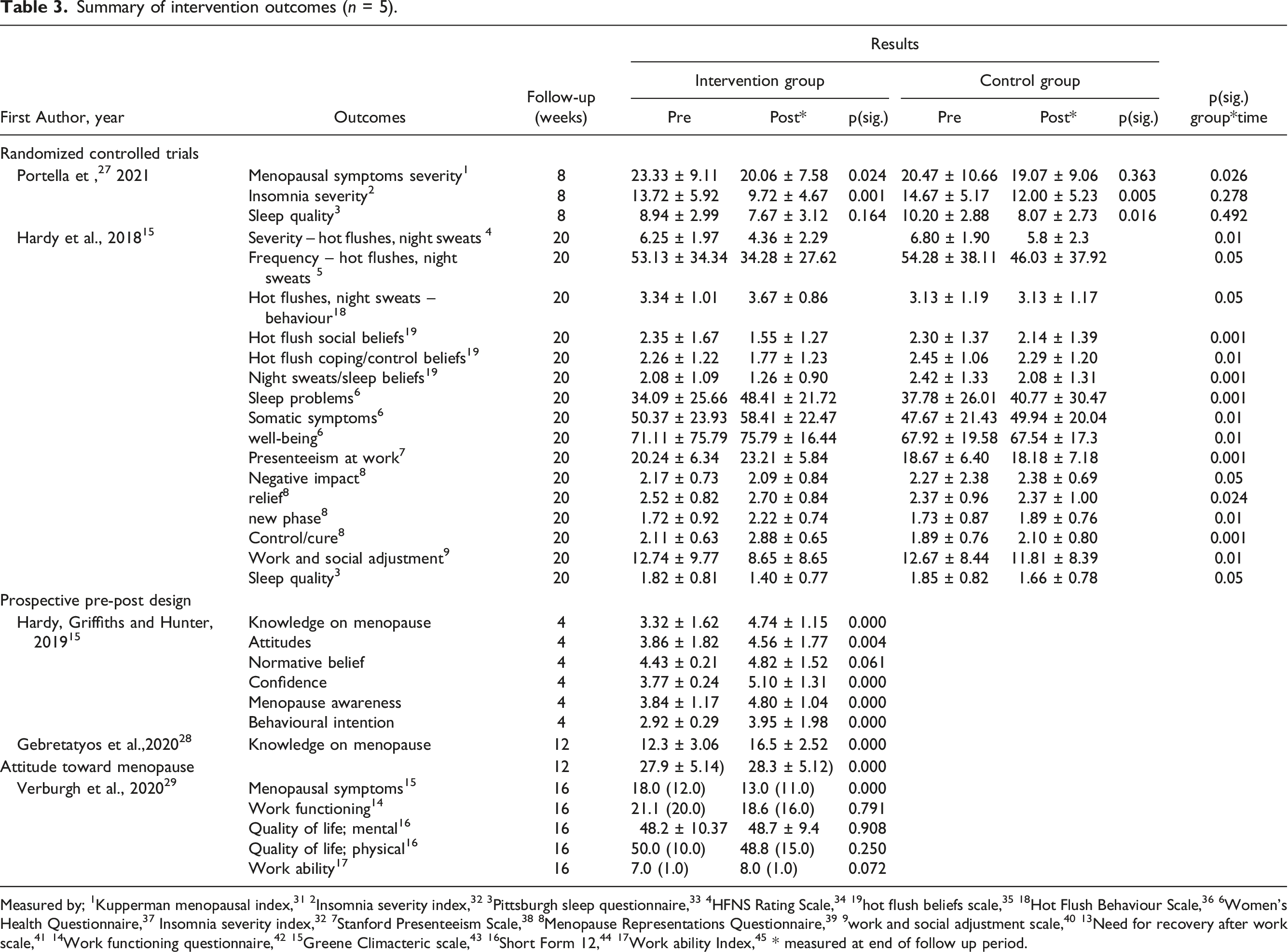
Measured by; 1Kupperman menopausal index, 31 2Insomnia severity index, 32 3Pittsburgh sleep questionnaire, 33 4HFNS Rating Scale, 34 19hot flush beliefs scale, 35 18Hot Flush Behaviour Scale, 36 6Women’s Health Questionnaire, 37 Insomnia severity index, 32 7Stanford Presenteeism Scale, 38 8Menopause Representations Questionnaire, 39 9work and social adjustment scale, 40 13Need for recovery after work scale, 41 14Work functioning questionnaire, 42 15Greene Climacteric scale, 43 16Short Form 12, 44 17Work ability Index, 45 * measured at end of follow up period.
Discussion
Principal findings
To the authors’ knowledge, this is the first systematic review exploring the effectiveness of workplace-based interventions for menopause. The interventions for menopause implemented at workplaces were limited in number, heterogenous, and included self-help CBT, Raja yoga, health promotion (including menopause consultations, work–life coaching, and physical training) and awareness programs.15,16,27–29 Menopausal symptoms significantly improved following Raja yoga 27 self-help CBT 15 and health promotion sessions. 29 In addition, self-help CBT reported a significant improvement in presenteeism and work and social adjustment. Awareness programs significantly improved knowledge and attitudes regarding menopause.16,28
Interpretation of results
This review supports self-help CBT as an intervention that can be employed at work settings to alleviate menopausal symptoms and to improve work outcomes. CBT helps to change negative cognitions linked with menopausal symptoms such as fear or embarrassment due to hot flushes. 30 CBT has been reported to reduce the work time impaired by insomnia 25 and is also recommended in NICE guidelines for menopause. Self-help CBT was identified as the only intervention leading to favourable work outcomes during this review.
This review observed the effectiveness of Raja yoga for alleviating menopausal symptoms among working women. Previous mind body therapy interventions of yoga and other breathing based exercises in the community have reported similar improvements in menopausal symptoms and sleep. 46 The WLP promoted a healthier lifestyle through guidance on nutrition, physical activity, and menopausal counselling. Proper nutrition and physical activity are essential for combating increased cardio-metabolic and osteoporosis risk among menopausal women and should be part of any wellbeing strategy for menopause. Menopausal counselling further enabled them to make healthy life choices. 29 The reviewed health education interventions16,28 were short and feasible. They effectively improved knowledge and attitudes relating to menopause highlighting a vacuum of awareness among participants. More robust awareness programs might elicit a significant change in communications on menopause at workplaces. 16
Strengths and limitations of this review
This review does not include a meta-analysis due to the wide heterogeneity observed among included studies. We observed that the study designs, type of workplaces, categories of staff, intervention types, duration, and outcome measures were unique and different for each study. Hence, we attempted to categorise studies by hierarchy of evidence and broad outcome groups during the narrative synthesis. In addition, the strength of evidence generated by this review is limited by the fact that we came across only a few interventions and they were different from each other. More RCT from each intervention type would have enabled to us to present more robust review findings. There is literature suggestive of interventions that are effective in the community setting for menopausal symptoms and functioning of menopausal women. Since the ‘workplace and menopause’ is a topic of current interest it is likely newer interventions will be carried out at workplaces in the future. Given the paucity of published interventions on the topic, we have collated and presented the currently available evidence.
Limitations in the literature and directions for future research
Our review included studies of moderate quality and their interpretations are subject to methodological limitations. Deficiencies noted in the methods were; unadjusted confounding in the uncontrolled studies, lack of blinding, allocation concealment and possible contamination in the RCTs. Outcomes measured using self-administered instruments could be subjective while volunteer participants are likely to be more health-conscious or be more affected by menopausal symptoms. Sample size calculations were also not outlined in most studies while some studies reported poor compliance due to work and other commitments. Further, the interventions were of short durations with the maximum being 5 months. Most studies had presented outcome data at the end of the intervention period and long-term follow-up data were lacking. Only the awareness programs had followed up participants following the intervention. Long term benefits are difficult to be ascertained with interventions limited to a few months and work-related outcomes could take a longer time to show an improvement. Longer duration higher quality RCT might provide stronger evidence as some studies have reported non-significant improvements in work outcomes.21,24,29,32 However, the interventions did not have any in-built mechanisms to ensure long term sustainability which would be necessary to obtain long term benefits in a dynamic workplace setting where there is likely to be a high turnover of employees.
Implications for policy and practice
The EMAS guidelines recommends for employers and organizations to make health and wellbeing during menopause a priority in the workplace with the support of line managers, healthcare workers and employees. 13 Interventions for menopause should be culturally and economically sensitive to ensure sufficient recruitment and compliance. Most women still feel that menopause is a taboo topic at work 22 and this is worsened by racial disparities and male dominance in managerial roles. Employers should consider initiating awareness on menopause at a wider scale as awareness alleviates the stigma and enables discussion and decision-making. Awareness is also likely to improve compliance for further interventions such as CBT and mind body therapy. Menopausal transition should be used as a window of opportunity to promote a healthier lifestyle at the workplace and thereby prevent undesirable health and work outcomes in future. Despite recommendations within existing guidance, this review did not identify any studies concerned with alterations to the physical environments of the workplaces.
The experience of menopause is unique to each woman and different modes of support are likely to be appreciated by different women and their employers. Given the heterogeneity of interventions observed during our review and their varying degrees of effectiveness in improving different outcomes among menopausal women we recommend development and implementation of a customisable multi-component package of interventions at workplaces for menopause incorporating the reviewed evidence. This menopausal wellbeing-oriented intervention package requires to be flexible and culture sensitive. Women, practitioners, and employers should be provided the necessary knowledge and empowered to choose interventions that are most appropriate for them depending on symptom presence or absence, type of employment and workplace requirements. Such a package should ideally include screening for unhealthy lifestyle and non-communicable disease since both are known to worsen the negative impacts of menopausal symptoms.
Conclusions
Self-help CBT, Raja yoga, and support to adopt healthy lifestyles are interventions that were significantly effective in reducing menopausal symptoms and should be considered for inclusion in work-based programmes to support women who are going through the menopause. There is still a vast knowledge and attitude gap to be filled among both menopausal women and their employers regarding menopause and this could be addressed using short duration health education sessions aiming to induce a behaviour change towards menopause at work. Sustainable interventions of longer duration are likely to be of more benefit and should be tested in the future. Overall, CBT, Raja yoga, support to adopt healthy lifestyles, and menopause awareness interventions reviewed in this study were found to improve various aspects of wellbeing among menopausal women and could be used in combination in future and customized to individual women’s or organizations’ needs as appropriate.
Footnotes
Acknowledgements
We would like to acknowledge the support extended by the Aberdeen Center for Women’s Health Research and Department of Public Health of the University of Aberdeen.
Contributorship
Paper conception and design was done by CHR, and SB. Literature search was done by CHR and review, and data extraction were done by CHR and ES. Manuscript and table preparation was done by CHR. Critical review/revision was done by SB, SP and MB.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.