
Abstract
Background:
The menopausal transition involves multiple biological and psychosocial challenges that may render middle-aged women vulnerable to body image concerns.
Objective:
The aim of this study was to summarize evidence on the associations between menopause and body image perception in healthy middle-aged women.
Design:
This study is a systematic review of observational studies.
Data sources and methods:
Menopause-related exposure measures included menopausal stages, menopausal symptoms, and reproductive hormone levels during the menopausal transition. Studies investigating body image as an outcome, including through a positive (e.g. body self-esteem) or negative (e.g. body dissatisfaction) lens, were considered eligible. Articles published before March 2023 were identified through MEDLINE, PsycINFO, and Embase and underwent double screening, extraction, and quality assessment by two independent investigators. Characteristics and results were summarized using narrative synthesis.
Results:
A total of 820 non-duplicate records were identified, with 18 observational studies deemed eligible for inclusion after full-text screening. All studies investigating menopausal symptoms and body image (n = 6) found some significant association between them, with a higher frequency, intensity, or number of symptoms being associated with greater body image concern. Differences in body image perception between menopausal stages were inconsistent across studies (n = 12), while evidence of potential associations between reproductive hormones and body image was minimal (n = 2). Findings should be interpreted with caution as 17 of the included studies used a cross-sectional design, and not all studies adjusted their analyses for relevant confounders.
Conclusion:
Overall, menopausal symptoms showed relatively consistent associations with a more negative body image perception. Additional research is required to understand the potential role of menopausal stages and reproductive hormone levels in the body image perception of middle-aged women and to confirm the direction of reported associations.
Registration:
PROSPERO—CRD42021241637
Keywords
Introduction
Body image is a multidimensional concept that is commonly defined as a person’s perception, thoughts, attitudes, and feelings regarding their own body. 1 As a component of mental health, body image distinguishes itself by focusing on self-perceived appearance, attractiveness, and body functioning, and by encompassing the emotional importance attributed to one’s own appearance and the level of confidence and acceptance they feel toward their body.1,2 It is often assessed through a person’s level of satisfaction or concern in relation to these concepts, or through behavioral tendencies, such as concealing, altering, tending to, or checking on their body.3,4
Body image perception is an important contributor to global psychological well-being. People with more body image concerns tend to have lower self-esteem 5 and experience greater levels of depressive symptoms, 6 anxiety, 7 and disordered eating behaviors. 8 The implications of body image also go beyond mental health, with evidence showing that a more positive body image is associated with greater sexual well-being, 9 adherence to various health-promoting behaviors,10,11 and better overall quality of life. 12
Women tend to be disproportionately affected by body image disturbances, as they usually attribute more importance to their appearance than men. 13 Although research on body image has mainly focused on younger women, a number of studies reported rates of body dissatisfaction that ranged from 40% to 80% in middle-aged and older women,14 –16 highlighting how body image concerns continue to significantly affect women as they age. Throughout women’s lives, periods involving great physical, hormonal, and psychosocial changes such as puberty, pregnancy, and post-partum have been identified as windows of vulnerability for increased body dissatisfaction.17 –19 However, investigations into the menopausal transition as a particular period of interest have been more limited, and the relationships between women’s experience of menopause and their body image perception are not well understood.
The term menopause refers to the cessation of women’s menses and reproductive potential due to the reduction of ovarian follicular activity. 20 It is a natural process occurring during middle age (40–65 years old) and most commonly during women’s early 50s, 21 although it can also be induced through medical intervention. Whereas menopause is declared retrospectively following 12 months of amenorrhea, 21 the menopausal transition is a wider term that also encompasses the stages surrounding menopause, including peri- and postmenopause, during which women can experience irregular menses, hormonal fluctuations, and various types of menopausal symptoms (e.g. hot flashes, night sweats, insomnia, mood swings, brain fog, migraines, vaginal dryness, frequent urination, etc.). 22 Changes in the length and regularity of menses start on average 6–8 years before the final menstrual period. 23 However, menopausal symptoms, which are reported by approximately 75% of women, 24 have a median duration of 7.4 years including 4.5 years after the cessation of menses, 25 highlighting the extent to which women’s lives may be affected by the menopausal transition. In addition to skin aging and changes in hair density and distribution,26,27 the menopausal transition implicates significant changes in body composition (i.e. increase in fat mass and a decrease in muscle mass) and body fat distribution (i.e. increase in trunk fat and visceral fat mass),28,29 which strays away from the western societal ideal of beauty and may exacerbate body image concerns. Evidence also suggests that mental health issues could be more prevalent during the menopausal transition, with a number of studies finding an increased risk of anxiety and depressive symptoms during peri- and postmenopause when compared to the premenopausal stage.30,31 Finally, limited evidence from younger populations has found that body dissatisfaction and eating disorder symptoms may be partly dependent on phases of the menstrual cycle and reproductive hormone levels,32 –38 leading to the suggestion that the variations in estrogen and progesterone levels experienced during the menopausal transition could influence body image perception. 39
This combination of biological and psychosocial factors has led researchers to investigate if women’s body image, similar to what is observed during puberty or post-partum, could be negatively affected by the menopausal transition. Some narrative reviews discussing body dissatisfaction and disordered eating in middle-aged and older women briefly mentioned this hypothesis,40,41 while a systematic scoping review of heterogeneous study designs published by Pearce et al. in 2014 concluded that, although research on this issue was still in its infancy at the time, the relationship between menopause and body image seemed equivocal and should not be considered as strictly positive or negative. 42 Considering that the number of post-menopausal women worldwide is expected to reach 1.2 billion by 2030, 43 the understanding and optimal management of women’s physical and psychological health through this transition is of great importance.
As this area of research has expanded in recent years, we aimed to perform a systematic review of the literature to identify and summarize observational studies addressing associations between the menopausal transition and body image perception in healthy middle-aged women. We compared the results obtained from three menopause-related exposure variables, namely (1) menopausal stages, (2) menopausal symptoms, and (3) reproductive hormone levels during the menopausal transition. Finally, we aimed to identify current research gaps and make recommendations for future studies surrounding this topic.
Methods
This review is reported using recommendations from the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement. 44 The PRISMA checklist is available in Supplemental Appendix A. The detailed protocol can be accessed through the International Prospective Register of Systematic Reviews (PROSPERO ID: CRD42021241637).
Eligibility criteria
Observational studies presenting quantitative results from original research using menopause as an exposure variable (i.e. independent variable), body image as an outcome variable (i.e. dependent variable), and healthy middle-aged women as the population of interest were sought for inclusion in this review. Qualitative studies, reviews, abstracts, dissertations, commentaries, letters, and books were not included.
As an exposure variable, the experience of the menopausal transition can be assessed using menopausal stages, which are commonly determined using self-report of menstruation history, although confirmation through hormonal biomarkers is recommended. 45 Most studies included in this review defined pre-, peri- and postmenopause as proposed in the 1981 Research on Menopause report published by the World Health Organization (WHO). 46 Accordingly, this article will also use the following criteria when referring to menopausal stages: (1) premenopause relates to the period prior to menopause, when there is no change in the usual frequency of the menstrual cycle, or when there have been changes for less than 3 months; (2) perimenopause refers to the period for which there have been at least 3 months of change in the frequency of menses, but less than 11 months of amenorrhea; and (3) postmenopause begins after 12 consecutive months of amenorrhea. As the menopausal transition involves various somatic and vasomotor symptoms which are experienced by most women throughout different menopausal stages, 22 studies using comprehensive scales of menopausal symptoms as an exposure variable were included in this review. The assessment of reproductive hormone levels such as estradiol (E2), progesterone (P4), and follicle-stimulating hormone (FSH) during the menopausal transition was also considered as an exposure of interest. Studies that included surgically menopausal women exclusively, or that investigated middle-aged women without specifically using menopausal stages, symptoms, or reproductive hormone levels as an exposure variable in their analyses were excluded from this review.
Body image is a psychological measure commonly assessed using validated self-reported scales and questionnaires. 3 Other terms used to refer to this concept include, but are not limited to, body self-esteem, body acceptance, body satisfaction or dissatisfaction, body perception, self-representation, and appearance evaluation. All studies investigating body image-related measures were included, with no restriction on the use of tools with a positive (e.g. body appreciation) or negative (e.g. body dissatisfaction) connotation. Studies investigating general self-esteem, with no measure or subscale pertaining directly to body image, were excluded from this review.
To better isolate natural menopause as the exposure variable, studies focusing on women with a medical condition that can significantly interfere with body image (e.g. breast cancer survivors) were excluded from this review.
Literature search
The MEDLINE, PsycINFO, and Embase databases accessed through Ovid® Synthesis Clinical Evidence Manager were searched to identify relevant records. Language was restricted to French and English articles as these are the primary languages of our research team. No restrictions were applied to the publication period. Searches were initially run in March 2021 and were last updated in March 2023. A citation check was additionally performed for all included studies. Unpublished records were not sought.
Per our main objective, the search strategy comprised menopause and body image as its principal themes. The Menopause and Body image MeSH terms were used, and various other terms were added to the strategy to allow for the identification of studies on a range of body-image-related measures. This included body perception/satisfaction/dissatisfaction/representation/schema/confidence OR weight/shape concern OR appearance evaluation OR perceived attractiveness OR body self-esteem. The full search strategy is available in the published protocol (PROSPERO ID: CRD42021241637).
Study selection
All identified records were imported into the Covidence screening and data extraction tool to facilitate removal of duplicates and multi-step screening. As recommended by the Cochrane Handbook for Systematic Reviews of Interventions, 47 two authors (C.V. and V.O.) began by independently screening all identified records by title and abstract to exclude irrelevant records. The same two authors then independently performed full-text screening of the remaining records to select eligible studies. At both steps of screening, conflicts were resolved by discussions with a third author (A.M.B.). During full-text screening, reasons for exclusion included (1) wrong publication type (e.g. conference abstracts, reviews, qualitative studies), (2) wrong exposure (i.e. studies in which no menopause-related measures were used as the independent variable), (3) wrong outcome (e.g. general self-esteem and mental health measures not specifically related to body image), (4) wrong population, and (5) insufficient data (e.g. a study that investigated both variables of interest but did not report results on the association between the two).
Data extraction
Extraction of characteristics and results of included studies was also performed by two authors (C.V. and V.O.), with disagreements being resolved by discussions with a third author (A.M.B.). Data extraction was conducted independently using Excel spreadsheets and combined into one common document once all disagreements were resolved. Data collected from eligible articles included year of publication, country of origin, study design, study duration, sample size, sampling methods, sample demographic information, inclusion/exclusion of women using hormonal replacement therapy (HRT), and women who underwent a surgically induced menopause, exposure variables and related assessment tools, outcome variables and related assessment tools, control for confounding variables, and results pertaining to our variables of interest.
Methodological quality assessment
As all of the eligible studies included in this review used a cross-sectional design, except for one micro-longitudinal pilot study (⩽ 40 days), the assessment tool selected to measure risk of bias was the Newcastle-Ottawa Quality Assessment Scale (NOS) adapted for cross-sectional studies.48,49 The NOS is the most commonly used tool for the critical appraisal of cohort and case–control medical studies and allows for the adaptation of scale items based on the review’s exposure and outcome variables of interest. 50 It was first adapted for the cross-sectional design by Herzog et al. 49 and has since been effectively used by reviews in the mental health field.51,52 This quality assessment scale previously demonstrated moderate reliability and superior ease of use when compared to other tools, 53 although there is currently no established gold standard for the critical appraisal of cross-sectional studies. The adapted NOS uses a star system by which each star accounts for 1 point, with a maximum score of 10 points, and with a higher score being indicative of better methodological quality and lower risk of bias.49,54 Stars are allocated through three subscales: (1) Selection (five stars), which assesses the representativeness of the sample, sample size, rate of non-respondents, and methods used for the assessment of the exposure variable; (2) Comparability (two stars), which relates to the control of confounding factors; and (3) Outcomes (three stars) relating to the assessment of the outcome variable and the appropriate use and reporting of statistical tests. The total score then allows for the classification of studies in four levels of methodological quality: unsatisfactory studies (0–4 points), satisfactory studies (5–6 points), good studies (7–8 points), and very good studies (9–10 points).51,55 The detailed NOS scale and clarifications on how it was used in this review can be found in Supplemental Appendix B. The quality assessment was completed independently by two authors (C.V. and V.O.) for all included studies. Disagreements between assessors’ judgments were resolved by discussion with a third author (A.M.B.).
Synthesis method
As included studies were considerably heterogeneous in methodology, their characteristics and results were summarized using narrative synthesis. 56 Indeed, many different tools were used across eligible studies to measure various aspects of body image, with multiple studies also using several distinct body image scales and subscales as part of their analyses. Similarly, not all menopausal stages were included or characterized the same way in all studies, while menopausal symptoms were also assessed through various tools, with varying ways of categorizing symptom categories, frequency, and severity. Considering the substantial risk of bias in included studies, and the diversity of assessment tools, statistical tests, and covariates used, a meta-analytic synthesis was deemed inappropriate. A qualitative table of study characteristics and results combined with a comprehensive narrative synthesis of emerging trends was considered optimal to accurately synthesize the methods and results of included studies.56,57
Results
Search results
Results from the identification and selection process can be found in the PRISMA flow diagram (Figure 1). After removal of duplicates, 820 records were screened by title and abstract, with 50 records undergoing full-text screening and 17 articles being deemed eligible for inclusion in this review. One additional eligible study was identified during the citation check, bringing the total number of included articles to 18. The most common reason for exclusion during full-text screening was wrong publication type (n = 16),58,59 followed by wrong exposure (n = 8),60,61 and wrong outcome (n = 6).62,63

PRISMA flow diagram.
Study characteristics
The main characteristics of included studies are presented in Table 1. All studies used a cross-sectional design, except one micro-longitudinal correlational pilot study which measured daily salivary E2 and P4 levels over one menstrual cycle or up to 40 days. 64 All included studies were published after the year 2000, with 15 studies published after 2010.
Main characteristics and results of articles included in the review (n = 18).
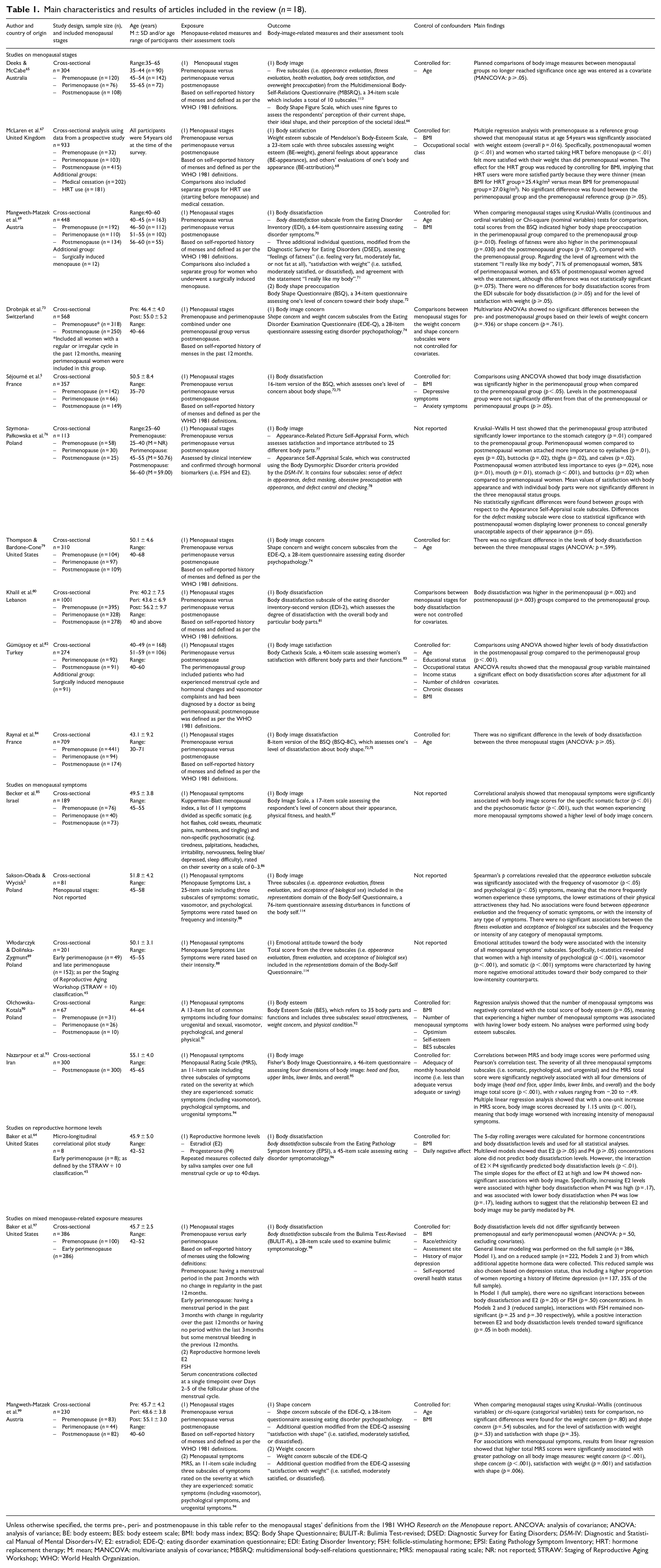
Unless otherwise specified, the terms pre-, peri- and postmenopause in this table refer to the menopausal stages’ definitions from the 1981 WHO Research on the Menopause report. ANCOVA: analysis of covariance; ANOVA: analysis of variance; BE: body esteem; BES: body esteem scale; BMI: body mass index; BSQ: Body Shape Questionnaire; BULIT-R: Bulimia Test-revised; DSED: Diagnostic Survey for Eating Disorders; DSM-IV: Diagnostic and Statistical Manual of Mental Disorders-IV; E2: estradiol; EDE-Q: eating disorder examination questionnaire; EDI: Eating Disorder Inventory; FSH: follicle-stimulating hormone; EPSI: Eating Pathology Symptom Inventory; HRT: hormone replacement therapy; M: mean; MANCOVA: multivariate analysis of covariance; MBSRQ: multidimensional body-self-relations questionnaire; MRS: menopausal rating scale; NR: not reported; STRAW: Staging of Reproductive Aging Workshop; WHO: World Health Organization.
Sample characteristics
When excluding the previously mentioned micro-longitudinal pilot study which only included 8 participants, 64 the sample size of eligible studies ranged from n = 67 90 to n = 1001, 80 with an average of 387 participants (SD = 291). As presented in Table 1, the age range required for inclusion was generally between 40 and 65 years.2,64,69,85,89,90,93,97,99 Other studies established the minimum age at 25, 76 30, 84 or 35 years,5,65 and the maximum age at as high as 71 years. 84 Notably, only some of these studies reported controlling their analyses for the effect of age. In studies where a mean body mass index (BMI) was reported, most reported a value within the “normal-weight” (18.5–24.9 kg/m2),69,76,99 or the “overweight” categories (25–29.9 kg/m2).67,79,97 Rates of participants reporting being married or in a partnership were generally above 75%,2,5,64,69,84,85,89,90,93,99 while education level varied greatly across study samples. Studies also differed considerably in their inclusion of women who were using HRT, or who underwent surgically induced menopause. Details on the sample characteristics of included studies, including BMI, employment, marital/relationship status, education level, and the inclusion of HRT users and women who underwent surgical menopause can be found in Supplemental Appendix C.
Menopause-related exposure measures
To investigate associations between menopause and body image, most studies (n = 15) used menopausal stages as an exposure measure, and defined pre-, peri- and postmenopause as described in the WHO Research on the Menopause report 46 (see Table 1).
Of these studies, Baker et al. 97 did not include all three menopausal stages as their study focused on premenopausal and early perimenopausal women, while Gümüşsoy et al. 82 only included peri- and postmenopausal women, with their third group of interest consisting of women with surgically induced menopause. In addition, the study by Drobnjak et al. 73 categorized their participants as either pre- or postmenopausal, but the criteria used to define stages implied that perimenopausal women who experienced an irregular cycle over the past 12 months were included in the premenopausal group.
All studies used self-reported menstruation history to assign menopausal stage, with the exception of the study by Szymona-Pałkowska et al. 76 which assessed menopausal status by clinical interview and confirmed it with FSH and E2 levels, and the study by Gümüşsoy et al. 82 in which perimenopausal women had their menopausal status diagnosed by a doctor. Notably, Baker et al. 64 and Włodarczyk and Dolińska-Zygmunt 89 were the only studies that reported using the Staging of Reproductive Aging Workshop (STRAW + 10) classification, 45 considered as a gold standard to define menopausal status. However, none of these two studies used menopausal stage as an exposure measure in their analyses.
The second most common menopause-related exposure measure was menopausal symptoms, which were used by a total of six studies.2,89,90,93,99 Different tools were employed across studies to assess symptoms. Two studies2,89 used the Menopause Symptoms List, 88 a 25-item scale that includes three subscales of symptoms: somatic (e.g. sleep difficulty, headaches, weight gain, dyspareunia, loss of sexual interest), vasomotor (e.g. hot flashes, night sweats, shortness of breath, palpitations, numbness, and tingling), and psychological (e.g. irritability, depressed feelings, crying spells, poor concentration). The Menopausal Rating Scale (MRS) 94 was used by two studies93,99 and contains 11 items categorized as somatic (including vasomotor symptoms), psychological, or urogenital (e.g. vaginal dryness, frequent urination, discomfort with intercourse) symptoms. Becker et al. 85 used the Kupperman–Blatt Menopausal Index, 86 a tool containing 11 symptoms categorized as specific somatic (e.g. hot flashes, cold sweats, rheumatic pains, numbness, and tingling) or non-specific psychosomatic (e.g. tiredness, palpitations, headaches, irritability, nervousness, feeling blue/depressed, sleep difficulty). Finally, one study used a 13-item list of common symptoms proposed by Jane and Davis, 91 in which menopausal symptoms are categorized into four domains, namely urogenital and sexual, vasomotor, psychological, and general physical (somatic) symptoms. 90 Symptoms were used as an exposure variable by assessing their intensity, frequency, or both.
The third method used to explore associations between menopause and body image involved the assessment of reproductive hormone concentrations during the menopausal transition and was employed in two studies conducted by the same authors.64,97 In their first study, Baker et al. 97 included pre- and early perimenopausal women and measured E2 and FSH serum concentrations once over Days 2–5 of the follicular phase of the menstrual cycle. In their subsequent study, Baker et al. 64 included early perimenopausal women exclusively and collected daily saliva samples to measure E2 and P4 concentrations over one full menstrual cycle, or up to 40 days. They then proceeded to use 5-day person-standardized rolling averages of hormone levels and of their outcome measures to perform their analyses. The measurement of salivary hormone levels has been found to be an accurate surrogate marker of serum concentrations for reproductive hormones, such as E2 and P4, particularly when measuring variation over time.32,100,101
Body-image-related outcome measures
Overall, 17 different scales and questionnaires were employed to assess body image across the 18 studies included in this review, with two of these tools (i.e. the Body Shape Questionnaire (BSQ) and the Eating Disorder Inventory (EDI))70,72 also being used under multiple versions.75,81 Moreover, seven studies either used more than one tool or reported results using multiple distinct subscales of a tool.2,65,69,73,76,93,99
Most studies (n = 10) employed tools designed for the assessment of body image specifically,5,65,67,69,76,82,84,85,90,93 such as the Body Image Scale, 87 the Body Shape Figure Scale, 66 the BSQ, 72 the Body Cathexis Scale, 83 Mendelson’s Body-Esteem Scale, 68 Fisher’s Body Image Questionnaire, 95 the Body Esteem Scale, 92 the Appearance-Related Picture Self-Appraisal Form, 77 and the Appearance Self-Appraisal Scale. 78 Seven studies used body-image-related subscales that were included in questionnaires designed to assess eating disorder symptomatology,64,69,73,79,80,97,99 such as the Bulimia Test-Revised (BULIT-R), 98 the Eating Pathology Symptom Inventory (EPSI), 96 the EDI, 70 the Eating Disorder Examination Questionnaire (EDE-Q), 74 and modified questions from the Diagnostic Survey for Eating Disorders (DSED). 71 The complete list of tools used in each study is available in Table 1. Notably, many of the tools were focused on the respondents’ negative emotions about their bodies, with an emphasis on body dissatisfaction, concern, and preoccupation.
Methodological quality of studies
The methodological quality assessment showed an average quality score of 6.6/10 points, indicative of a satisfactory quality level and considerable overall risk of bias across studies. Detailed quality ratings for each study can be found in Table 2. Notably, just under half of studies (n = 8) controlled their statistical analyses for BMI and at least one other variable.5,64,67,69,82,90,97,99 Moreover, few studies (n = 2) included a sample size justification and no studies used random sampling exclusively, although most study samples (n = 15) were considered to be somewhat representative of the average in the target population.2,5,65,67,69,76,79,84,85,90,93,99 Two studies were also penalized for the Statistical test item, as they presented significant p-values as “p < .05” instead of providing an exact value.2,5
Methodological quality assessment of included studies (n = 18) using the Newcastle-Ottawa Scale adapted for cross-sectional studies.

Source: Newcastle-Ottawa Scale adapted for cross-sectional studies 49 (adapted by authors).
One star (✱) = 1 point. Quality score classification: 9–10 points = very good studies; 7–8 points = good studies; 5–6 points = satisfactory studies; 0–4 points = unsatisfactory studies. Refer to Supplemental Appendix B for details on the adaptation of the tool and specific scoring criteria.
Associations between menopausal stages and body image
Results from all included studies are presented in Table 1. Of the 12 studies investigating the association between menopausal stages and body image, 4 studies found no significant differences between the body image of pre-, peri- and postmenopausal women.65,79,84,99 Baker et al., 97 who only included pre- and early perimenopausal women, also found no differences between groups. Similarly, Drobnjak et al. 73 did not find significant differences when comparing postmenopausal women to pre- and perimenopausal women combined.
The remaining six studies found contrasting results that depended on the body image measures or subscales that were analyzed, or that differed by the stages at which body image was found to be of greater concern. First, Séjourné et al. 5 reported that levels of body dissatisfaction were significantly higher in the perimenopausal group when compared to the premenopausal group (p < .05), while no significant differences were found between the postmenopausal and the pre- or perimenopausal groups (p ⩾ .05). Similarly, Mangweth-Matzek et al. 69 found that the total scores from the BSQ indicated higher body shape preoccupation in the perimenopausal group compared to the premenopausal group (p = .010), and that “feelings of fatness” were higher in the perimenopausal (p = .030) and the postmenopausal groups (p = .027) compared to the premenopausal group. Nonetheless, they did not find significant differences when using scores from the EDI body dissatisfaction subscale (p ⩾ .05) or the level of satisfaction with weight (p ⩾ .05). 99 Khalil et al. 80 found that body dissatisfaction was higher in perimenopausal (p = .002) and postmenopausal (p = .003) women compared to premenopausal women, while Gümüşsoy et al. 82 found higher levels of body dissatisfaction in the postmenopausal group compared to the perimenopausal group (p < .001). McLaren et al. 67 also found that menopausal status at age 54 years was significantly associated with weight esteem (p = .016). However, unlike the previously mentioned studies, they reported that postmenopausal women (p < .01), and women who started taking HRT before menopause (p < .01), felt more satisfied with their weight than did premenopausal women, with no significant difference between the pre- and perimenopausal groups. 67 The authors mentioned that the effect for the HRT group was reduced by controlling for BMI, implying that HRT users were more satisfied with their weight partly because they were thinner. 67 Finally, Szymona-Pałkowska et al. 76 found no difference in women’s level of satisfaction with their appearance or with specific body parts depending on menopausal status, but found significant differences in the importance attached to certain body parts. In particular, they found that postmenopausal women attributed less importance to eyes (p = .024), nose (p = .01), mouth (p = .01), stomach (p < .001), and buttocks (p = .02) when compared to premenopausal women, leading the authors to conclude that postmenopausal women may derive greater satisfaction from their body. 76
Associations between menopausal symptoms and body image
As presented in Table 1, the six studies that investigated body image perception in relation to menopausal symptoms found some significant relationships between body image and the intensity, frequency, or number of certain menopausal symptoms.2,85,89,90,93,99 First, Becker et al. 85 found that body image scores were significantly associated with menopausal symptoms, both for the specific somatic (p < .01) and the psychosomatic factor (p < .001) of the Kupperman–Blatt Menopausal Index, such that women experiencing a higher severity of menopausal symptoms presented with greater body image concerns. Similarly, Włodarczyk and Dolińska-Zygmunt 89 reported that emotional attitudes toward the body were associated with the intensity of all menopausal symptoms’ subscales, with women reporting a high intensity of psychological (p < .001), vasomotor (p < .001), and somatic (p < .001) symptoms having more negative attitudes toward their body. Mangweth-Matzek et al. 99 echoed these findings with their results showing that the total score from the MRS was significantly associated with all assessed body image measures, including weight concern (p < .001), shape concern (p < .001), satisfaction with weight (p = .001), and satisfaction with shape (p = .006). Olchowska-Kotala 90 reported that the number of menopausal symptoms experienced was negatively correlated with body esteem scores (p = .05). Furthermore, Nazarpour et al. 93 found that the severity of all three menopausal symptoms subscales (i.e. somatic, psychological, and urogenital) from the MRS, and the MRS total score, was significantly negatively associated with all dimensions of body image and with the body image total score (p < .001). They also performed linear regression and reported that with a one-unit increase in MRS score, body image scores decreased by 1.15 units (p < .001), meaning that body image worsened with increasing intensity of menopausal symptoms. 93 However, Sakson-Obada and Wycisk 2 reported mixed findings. Contrary to Włodarczyk and Dolińska-Zygmunt 89 who used the total score of the representations’ domain from the Body-Self Questionnaire to assess body image, Sakson-Obada and Wycisk 2 performed separate analyses for each of this domain’s three subscales (i.e. appearance evaluation, fitness evaluation, and acceptance of biological sex). They found no associations between the fitness evaluation and acceptance of biological sex subscales and the frequency or intensity of any category of menopausal symptoms. However, the appearance evaluation subscale was significantly correlated with the frequency of vasomotor (p < .05) and psychological (p < .05) symptoms, meaning that women’s estimation of their physical attractiveness was lower when they experienced these symptoms more frequently. Nonetheless, no associations were found between the appearance evaluation subscale and the intensity of symptoms.
Associations between reproductive hormone levels and body image
The study by Baker et al., 97 which measured body dissatisfaction as well as FSH and E2 serum concentrations using a single measurement in time, recruited a subsample of pre- and early perimenopausal women from the Study of Women’s Health Across the Nation (SWAN). They used general linear modeling on their full sample (n = 386, Model 1) and on a reduced sample (n = 222, Models 2 and 3) from which additional appetite hormones data had been collected. In Model 1, no significant interaction was found between body dissatisfaction and E2 (p = .20) or FSH (p = .50) concentrations. In Models 2 and 3, interactions with FSH concentrations remained non-significant (p = .25 and p = .30 respectively), while a positive interaction between E2 concentrations and body dissatisfaction levels trended toward significance (p = .05 in both models). Baker et al. 97 proposed that this trend-level finding may suggest that the fluctuating E2 concentrations during midlife could affect body fat accumulation and waist circumference, which in turn could influence body dissatisfaction.102,103
In their subsequent micro-longitudinal pilot study, Baker et al. 64 measured salivary E2 and P4 concentrations and body dissatisfaction levels daily for one full menstrual cycle, or up to 40 days, in eight early perimenopausal women. 64 Multilevel models showed that salivary E2 and P4 concentrations alone were not associated with body dissatisfaction levels. However, the interaction of E2 × P4 significantly predicted body dissatisfaction levels (p < .01). This interaction was further investigated using simple slopes for the effect of E2 levels when combined with high- and low-P4 concentrations, which showed non-significant associations with body image. Specifically, increasing E2 concentration was associated with higher body dissatisfaction when P4 was high (p = .17), and with lower body dissatisfaction when P4 was low (p = .17), leading the authors to suggest that the potential relationship between E2 concentrations and body image during perimenopause may be partly mediated by P4 concentrations. 64
Discussion
This systematic review compiled 18 observational studies on the associations between menopause and body image. Emerging trends include relatively consistent associations between a greater intensity, frequency, or number of menopausal symptoms, and higher levels of body dissatisfaction, with all six studies on this topic reporting some significant findings.2,85,89,90,93,99
Menopausal symptoms have been found to be associated with several mental health issues, such as depressive symptoms, 30 but the direction and explanation behind these associations remain poorly understood. Across included studies, different types of symptoms showed significant associations with body dissatisfaction, including vasomotor, somatic, urogenital, and psychological symptoms. Two out of the six studies on this topic only used the total score from global menopausal symptoms scales,90,99 and one study found mixed results for different categories of symptoms, 2 making it difficult to draw specific conclusions. Indeed, as menopausal symptoms are highly varied in type, severity, and etiology, it is unclear whether they interact with body image altogether as an accumulation of negative physical and psychological experiences, or whether certain symptoms are more strongly associated with body image. It is possible that different types of symptoms have different explanations for their association with body image, going from physical changes (e.g. weight gain, skin, and hair changes), increased discomfort or body alienation (e.g. hot flashes, night sweats, rheumatic pains, palpitations, numbness and tingling, frequent urination, vaginal dryness, discomfort with intercourse), to more somatic (e.g. headaches, sleep difficulties) and psychological issues (e.g. mood swings, poor concentration, feeling blue/depressed, tiredness, irritability). Further research is needed to understand how different menopausal symptoms interact with body image, and how to help women maintain a positive body image perception while experiencing such ailments.
On the other hand, studies investigating menopausal stages as an exposure found contrasting results. Six studies reported no relationship between menopausal stages and body image,65,73,79,84,97,99 while six studies found some significant relationship.65,73,79,84,97,99 Two studies reported that certain body dissatisfaction measures were greater in perimenopausal women compared to pre- and postmenopausal women,5,99 one study found higher body dissatisfaction in both peri- and postmenopausal women compared to premenopausal women, 80 one study found higher body dissatisfaction during postmenopause compared to perimenopause, 82 and two studies reported that postmenopausal women seemed to be more satisfied with their body image than other menopausal status groups.67,76 Although convenient for conducting research, the use of menopausal stages based solely on self-reported menstruation history has been criticized, as the commonly used WHO definitions of pre-, peri-, and postmenopause have no hormonal biomarkers and are based on an arbitrary number of months spent in a certain state (e.g. perimenopause includes the first 11 months of amenorrhea, while postmenopause begins after 12 months). As noted by Sherman, 20 “The lack of unambiguous, non-overlapping criteria for classifying women into menopausal status categories that reflect homogeneous physiologic phenotypes has been a barrier to the comparison, generalization, integration, and dissemination of findings. . . .” 20 Indeed, there remains no clear, reliable, and universally accepted criteria to define the onset and offset of each menopausal stage. 99 Efforts have been made to provide more comprehensive staging tools, such as the STRAW + 10 classification, 45 which uses information relating to menses, certain hormone levels (i.e. FSH, anti-Müllerian hormone (AMH), inhibin B), and some menopausal symptoms to provide criteria for each stage. This staging system is considered the gold standard to define stages of reproductive aging.104,105 However, although its first version was published over 20 years ago, 106 none of the studies included in this review used this tool to assess and categorize menopausal stages when using them as the exposure variable.
Other factors may also play a role in the inconsistent results found regarding the association between menopausal status and body image. As previously mentioned, menopausal symptoms can occur during all stages of the menopausal transition. Their occurrence increases during the 2 years preceding the last menses, which often includes late premenopause and perimenopause, and they continue well into postmenopause with a median duration of 4.5 years following the final menstrual period. 25 Moreover, different women will experience different sets of symptoms, which can also vary in type, frequency, and intensity as they progress through each menopausal stage.24,107 Our review suggests that menopausal symptoms may be a key driver of disturbed body image during the menopausal transition, which could shed light on the lack of consistent and significant differences found between the body image perception of pre-, peri- and postmenopausal women.
Similarly, hormonal variations are not uniform across all women as they progress through menopausal stages. A longitudinal study from the SWAN used trajectory clustering of E2 and FSH concentrations among women undergoing the menopausal transition and found four distinct E2 trajectories and three distinct FSH trajectories. 108 Indeed, 27% of women experienced a slow decline in E2 over the 8 years preceding and following the final menstrual period, while 13% experienced a rise in E2 followed by a slow decline, 32% experienced a rise followed by a steep decline, and 29% had a relatively flat trajectory. 108 This implies that even if women are classified as being in the same menopausal stage as defined by history of menses, they could still present large inter-individual variations of reproductive hormone levels.
Several researchers have suggested that hormone levels should be taken into account to provide a full description of the association between body esteem and the menopausal transition.5,90 Unfortunately, the evidence identified in our review was too limited to allow for any conclusion regarding a potential association between reproductive hormones levels and body image perception. Of the two included studies on this topic, the first used one-time measurements of FSH and E2 serum concentrations to investigate associations with body dissatisfaction. 97 As mentioned in their article, 97 similar studies performed in young adults usually collect multiple measurements of the same hormones over a longer period of time to explore the impact of changing hormone levels on a psychological variable of interest.32,35 –37,109 The use of within-person change may be more informative than single-measure data when using reproductive hormone concentrations as an exposure, particularly during menopause, as hormonal trajectories over the course of the menopausal transition can differ significantly across the population of women. 108 In their subsequent pilot study, Baker et al. 64 took inspiration from young adult literature and collected daily salivary hormonal samples for a full menstrual cycle, or up to 40 days. 64 Their results suggested that the interaction between E2 and P4 concentrations could be associated with body dissatisfaction levels, which does reflect findings in younger women.36,37 Nevertheless, additional research is required to understand the role of hormonal variations in the association between the menopausal transition and body image and how it may affect women differently across all menopausal stages.
Overall, current literature seems to support the existence of an association between menopausal symptoms and body image, while evidence on the role of menopausal stages is conflicted, and findings on hormonal variations are scarce. It should also be considered that these three factors are strongly interrelated and may interact with each other to influence body image perception during the menopausal transition. Using them together as complementary menopause-related exposure measures may allow for a more thorough understanding of the timeline and mechanisms of influence between menopause and body image.
Methodological considerations
The findings of this review should be interpreted in the context of certain limitations. The methodological quality assessment revealed substantial overall risk of bias, with most studies using small sample sizes and convenience sampling. The limited overall number of included studies and the cross-sectional design used by most of them also weaken the strength of reported findings. Indeed, this design cannot establish the direction of the relationship between the exposure and outcome variable, and as such, does not allow for definitive causal inferences. In other words, there is no certainty as to whether menopausal symptoms affect body image, or whether women who have a disturbed body image experience symptoms more intensely or report them at a higher rate and severity. For example, a study by Rubinstein & Foster 110 found that women who reported greater body dissatisfaction held more negative attitudes toward menopause, which could potentially influence their perception on the experience of menopausal symptoms. 110 Moreover, many of the studies included in this review did not control for important confounders, such as age, BMI, physical activity levels, or psychological factors, which can hinder the ability to isolate menopause as the exposure of interest. For instance, the study by Deeks and McCabe 65 found significant associations between body image and menopausal stages, but only before controlling their analyses for the effect of age. 65
The large diversity of tools used to measure body image across studies also limits comparability. This heterogeneity in methods may partly be due to studies from different countries using scales created or already validated in the language of their participants. The scales assessed various themes, such as body dissatisfaction, weight and shape concerns, health and fitness evaluation, acceptance of biological sex, emotional attitude toward the body, weight esteem, body esteem, or general body image, which could partly explain the variety of results reported across studies. Many of the scales focused on negative attitudes toward the body (e.g. concern, preoccupation, dissatisfaction), which can have bias limitations. Previous qualitative and mixed-method studies on women’s perception and feelings about menopause highlighted a number of positive aspects of this transition, including a sense of freedom and liberation from the burdens and responsibilities associated with reproductive life.110,111 As such, tools that assess both negative attitudes and feelings of satisfaction, esteem, or happiness toward the body could offer a better balance to explore women’s global body image during the menopausal transition. 42
Although studies were conducted in a variety of countries, there was limited information available regarding the ethnicity or cultural background of study participants. Only four studies explicitly reported their samples’ ethnic background proportions,64,69,79,97 and only one included race/ethnicity as a covariate. Investigating differences between various ethnic backgrounds may be relevant, as women living in cultures with greater societal emphasis on beauty and attractiveness, as well as more negative attitudes toward aging or menopause, could potentially experience greater body image concerns during this transition. As explained by Voedisch et al., 112 “not only does the age and prevalence of symptoms fluctuate globally, perceptions of perimenopause and menopause are as varied as global cultural diversity.” Indeed, menopause is perceived differently across cultures and countries, which can influence both how women experience it and how health professionals view and approach issues related to it. 112
Finally, the narrative synthesis method used to summarize findings in this review does not allow for the determination of specific effect sizes regarding associations between the exposure and outcome variables, which limits the interpretability and generalizability of the results. Moreover, our searches were restricted to English and French language publications. Thus, it is possible that articles relevant to this review but published in other languages were not taken into consideration.
Gaps in knowledge
Additional research is required to better understand the interactions between menopause and body image, as the number and quality of studies identified in this review were limited. Future studies could verify and complement previous findings using optimal sample sizes, random sampling methods with adequate reporting of response rate, diverse samples, and by controlling for a larger number of relevant confounders. Crucially, there is a need for longitudinal studies on this topic. A longitudinal design would allow for the analysis of changes in the body image perception of the same sample of women over time in relation to changing menopausal stages, reproductive hormone levels, or variations in the number, frequency, and intensity of menopausal symptoms, thus allowing for a stronger understanding of the potential influence of all variables of interest. This design could also provide more information on the direction of the association between menopausal symptoms and body image and could be used to perform cluster analyses and identify subgroups of women that may be at a higher risk of experiencing body image concerns during the menopausal transition.
Future studies on menopausal symptoms should explore whether certain symptom categories or individual symptoms are more strongly related to body image, which could help deepen our understanding of the etiology behind this association. Qualitative or mixed-design studies could complement these findings by providing insight into women’s experience of menopausal symptoms and how they believe it may relate to their body image. Importantly, menopausal stages should be defined using validated criteria such as the STRAW + 10 classification and confirmed by the assessment of hormonal biomarkers, 45 while studies investigating reproductive hormones should aim for the assessment of changing hormone levels over time instead of using a single measurement. Moreover, future research should consider analyzing menopausal stages in conjunction with the assessment of menopausal symptoms and reproductive hormone levels to explore how these three menopause-related measures potentially interplay to influence body image. Other challenges that are common during the menopausal transition (e.g. weight gain, depressive symptoms, sleep difficulties, and fear of aging) could also play a role in mediating the association between menopause and body image and would benefit from further investigation. Finally, there is little research on the potential repercussions of increased body dissatisfaction during the menopausal transition, and on what strategies or behaviors middle-aged women may employ to cope with or alleviate such concerns.
Conclusion
Body image is an important component of self-concept that can interfere with many aspects of mental health and quality of life. While the menopausal transition is a normal yet complex and individualized experience, it commonly involves physical ailments, bodily changes, and psychosocial challenges that could potentially render middle-aged women susceptible to body image concerns. This systematic review aimed to summarize evidence from observational studies on women’s body image perception in relation to the menopausal transition. Our findings suggest that menopausal symptoms may be associated with body image concerns, while no definitive role of menopausal stages or reproductive hormone levels could be established. This information can be used to inform future research and help clinicians better support women during this paramount life transition. Additional research is required to address gaps in evidence and confirm the direction of reported associations.
Supplemental Material
sj-docx-1-whe-10.1177_17455057231209536 – Supplemental material for Associations between menopause and body image: A systematic review
Supplemental material, sj-docx-1-whe-10.1177_17455057231209536 for Associations between menopause and body image: A systematic review by Coralie Vincent, Alexandra M Bodnaruc, Denis Prud’homme, Viviane Olson and Isabelle Giroux in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057231209536 – Supplemental material for Associations between menopause and body image: A systematic review
Supplemental material, sj-docx-2-whe-10.1177_17455057231209536 for Associations between menopause and body image: A systematic review by Coralie Vincent, Alexandra M Bodnaruc, Denis Prud’homme, Viviane Olson and Isabelle Giroux in Women’s Health
Supplemental Material
sj-docx-3-whe-10.1177_17455057231209536 – Supplemental material for Associations between menopause and body image: A systematic review
Supplemental material, sj-docx-3-whe-10.1177_17455057231209536 for Associations between menopause and body image: A systematic review by Coralie Vincent, Alexandra M Bodnaruc, Denis Prud’homme, Viviane Olson and Isabelle Giroux in Women’s Health
Footnotes
Acknowledgements
The authors are grateful to University of Ottawa library staff for providing their unreserved support. The authors thank all the authors of studies included in this systematic review for their work.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.