
Abstract
Introduction:
Orthotopic neobladder (ONB) reconstruction following radical cystectomy for bladder cancer is a viable alternative to the formation of an ileal conduit. Although robotic surgery is gaining popularity, neobladder reconstruction is still most commonly done extra-corporeally (eONB) with a lower midline-laparotomy rather than intra-corporeal ONB (iONB) reconstruction. The novelty of a robotic approach has made several centres apprehensive to adopt this. This systematic review aims to compare functional outcomes as well as perioperative outcomes and common complications of robotic-assisted radical cystectomy with iONB versus eONB reconstruction.
Materials and methods:
A search of the literature from 2011 to 2021 was performed through PubMed, EMBASE, Medline and Scopus to identify articles comparing eONB formation with iONB formation. Urodynamic (UDS) outcomes (bladder volume, flow rate, post-voiding residual volume, continence rates and rate of clean intermittent catheterization (CIC) use) and perioperative outcomes (estimated blood loss, length of stay and operative time) were extracted as endpoints of interest. This review was registered with PROSPERO on 19 October 2022 (CRD42022366667).
Results:
Our searches identified 84 abstracts, of which 4 articles with 410 patients were eligible. Our results showed patients undergoing iONB had a higher bladder capacity and continence rate and achieved full continence much sooner than eONBs. iONBs, however, seemed to be left with higher residual volumes and a higher percentage of patients who needed CIC to void.
Conclusion:
Both perioperative outcomes and complications favoured the iONB technique; however, eONB seemed to give better functional outcomes.
Level of evidence:
Not applicable
Keywords
Introduction
Radical cystectomy is the gold standard treatment for patients with muscle-invasive bladder cancer (MIBC) and some patients with high-risk non-muscle-invasive bladder cancer. Following cystectomy, urinary diversion (UD) involves either the formation of an ideal conduit or the construction of an orthotopic neobladder (ONB). Although ileal conduits (ICs) are still most commonly performed, ONB is emerging as the gold standard and tends to give patients an improved quality of life (QOL). 1 They also help in the conservation of body image and replicating normal voiding function. ONB procedures also tend to have lower rates of reoperation and lower post-operative mortality when compared to IC counterparts. 2
Although the rate of local or distant metastasis is comparable when evaluating oncological outcomes post-UD, the data show that neobladders have lower rates of secondary urethral tumours than IC and other methods of UD. 3
Despite the absence of any formal surgical eligibility criteria to determine whether a patient is more suited for an ileal conduit or an orthotopic bladder substitution, different institutions seem to have their own methods of assessing suitability, in terms of existing comorbidities and success of future outcomes. An ONB is usually reserved for physically and mentally healthy patients with satisfactory renal function. It is supposed that these patients would be motivated enough to comply with neobladder training regimen and survive the complex ONB approach with its longer anaesthetic time. 2 ICs, however, have historically been selected for older patients with significant comorbidities or patients with previous urethral strictures and a history of an anterior urethral tumour.3,4
Other factors to consider when deciding on method of urinary diversion include: patient’s cardiopulmonary health, availability of post-operative support, mental health and personal preference. 4
An ONB is constructed following cystectomy by reshaping an isolated section of the patient’s bowel, usually the terminal ileum, to create a substitute for the bladder. The use of the terminal ileum helps maintain a low-pressure environment which is needed to prevent renal damage and incontinence. 5 Thus, it is the most preferred intestinal segment for a neobladder reconstruction. The sigmoid and colon have also been used. 5 Despite the benefits of using the terminal ileum, it is important to remember that using bowel as a replacement for bladder tissue can also cause metabolic acidosis, uretero-ileal stenosis and B12 deficiency. 4
The use of a lower midline incision for ONB reconstruction post-robotic-assisted radical cystectomy (RARC) is still the most commonly performed procedure. The International Robotic Consortium registry detailed that, of the 198 neobladders constructed post-RARC 2003–2011, only 61 were constructed completely intra-corporeally (6.5% of cases). 6 This could be possibly due to the novelty of robotic surgery, its perceived difficulties, longer operation times and lack of knowledge about complexities and functional outcomes both in the short and long terms.
Several techniques for totally intra-corporal neobladder reconstruction have been developed. Although these were only performed in less than 10% of cases, they seem to have completely replaced open surgery in some very specialist centres with the uptake of this method increasing to 17% in 2016.1,7
Potentially, a robotic construction would offer a minimally invasive approach, thereby reducing intra-abdominal exposure and the need of handling bowel. There is also evidence of reduced blood loss and the possibility of decreased complication rate, for instance, reduction in ureteral strictures due to reduced need to handle the ureters while operating in this manner. 8 Since the EUA guidelines recently have advocated orthotopic neobladder construction in all patients undergoing cystectomy, understanding the optimal technique is vital. 4
Materials and methods
A systematic review of the literature was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (PROSPERO). A published protocol is accessible online.
A literature search in PubMed, EMBASE, Medline and Scopus was performed. Any articles not published in the last 10 years that is from 2011 to 2021 were excluded. Studies not published in English or animal series were also excluded. Key words including Neobladder, Robotic surgery, Open surgery, RARC, Cystectomy, Bladder Cancer, Urinary Diversion, Outcomes, Functional outcomes and Urodynamics were used. The MeSH terms for the same were also included. We searched references of identified studies for any additional studies as well as searching relevant conference proceedings for the previous three years, for unpublished studies from annual meetings of the British Association of Urological Surgeons (BAUS), American Urological Association (AUA), and the European Association of Urology (EAU). The review considered all published studies, reviewing intra-corporeal ONB (iONB) and extra-corporeal ONB (eONB) including randomised controlled trials, non-randomised prospective and retrospective studies (if level 1 evidence was not available) reporting functional outcomes and complications. Two authors independently confirmed the suitability of the studies for inclusion (O.E. and M.B.).
All patients undergoing orthotopic neobladder construction following radical cystectomy were included; those undergoing cystectomy for indications other than bladder cancer, extended procedures (e.g. additional nephroureterectomy), and salvage/palliative cystectomy were excluded. Any disagreement in study selection was resolved by consulting a third reviewer (V.H.). In the case of incomplete reporting, the corresponding authors were contacted for further clarification.
The following details were extracted: year of publication, first author, country, study design, total number of patients, number of patients in each study arm, length of follow-up. Endpoints of interest were identified and discussed by all authors and included: Urodynamic study (UDS) outcomes (bladder volume, flow rate, post-voiding residual volume, continence rates and rate of clean intermittent catheterization (CIC) use),and perioperative outcomes (estimated blood loss, length of stay and operative time). Continence was defined as the complete freedom from use of pads. All of the data retrieved from the selected studies were recorded in an electronic database. Quality control of the electronic data recording was performed.
Sub-analysis of study data was performed to assess perioperative outcomes and complications from both techniques of orthotopic neobladder reconstruction from the studies (if available).
For the quality of non-randomised trials, we used the Newcastle-Ottawa scale (NOS) which was assessed independently by three reviewers (M.B., O.E. and V.H.). A score with a range of 0–9 was allocated to each study, and those with a score of 7 or more were considered to be higher-quality studies.
Statistical analysis
Descriptive statistics were used. A weighted average and range were calculated for all rates where available. A meta-analysis on risk factors for morbidity was not possible due to the high heterogeneity of reporting in the multivariate analysis across studies.
Results
Characteristics of studies obtained
Our searches identified 84 abstracts (Figure 1). Following elimination of duplicates and exclusion of articles not meeting our inclusion criterea, 4 articles were included for systematic review. Characteristics of the included studies are shown in Table 1. Three out of the 4 (75%), were single-centre studies and one study (15%) was multi-centre. Only one study was prospective in nature. The included studies all had recent publication dates (2016 or later) and all iONB were performed using the da Vinci surgical system (Intuitive Surgical, Sunnyvale, California, USA) as well as the AirSeal port system.
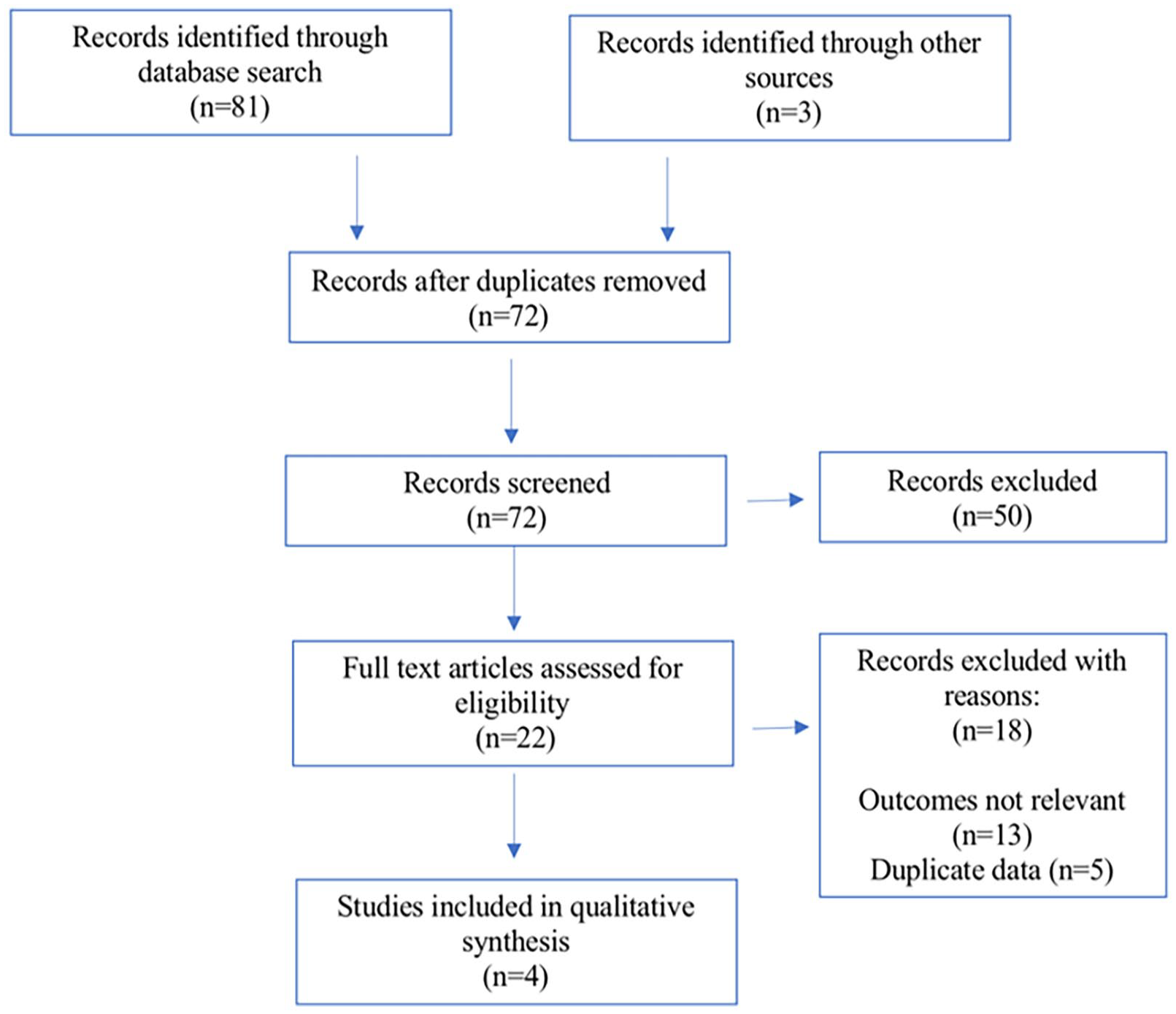
PRISMA chart. PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analysis.
Studies included in qualitative synthesis.
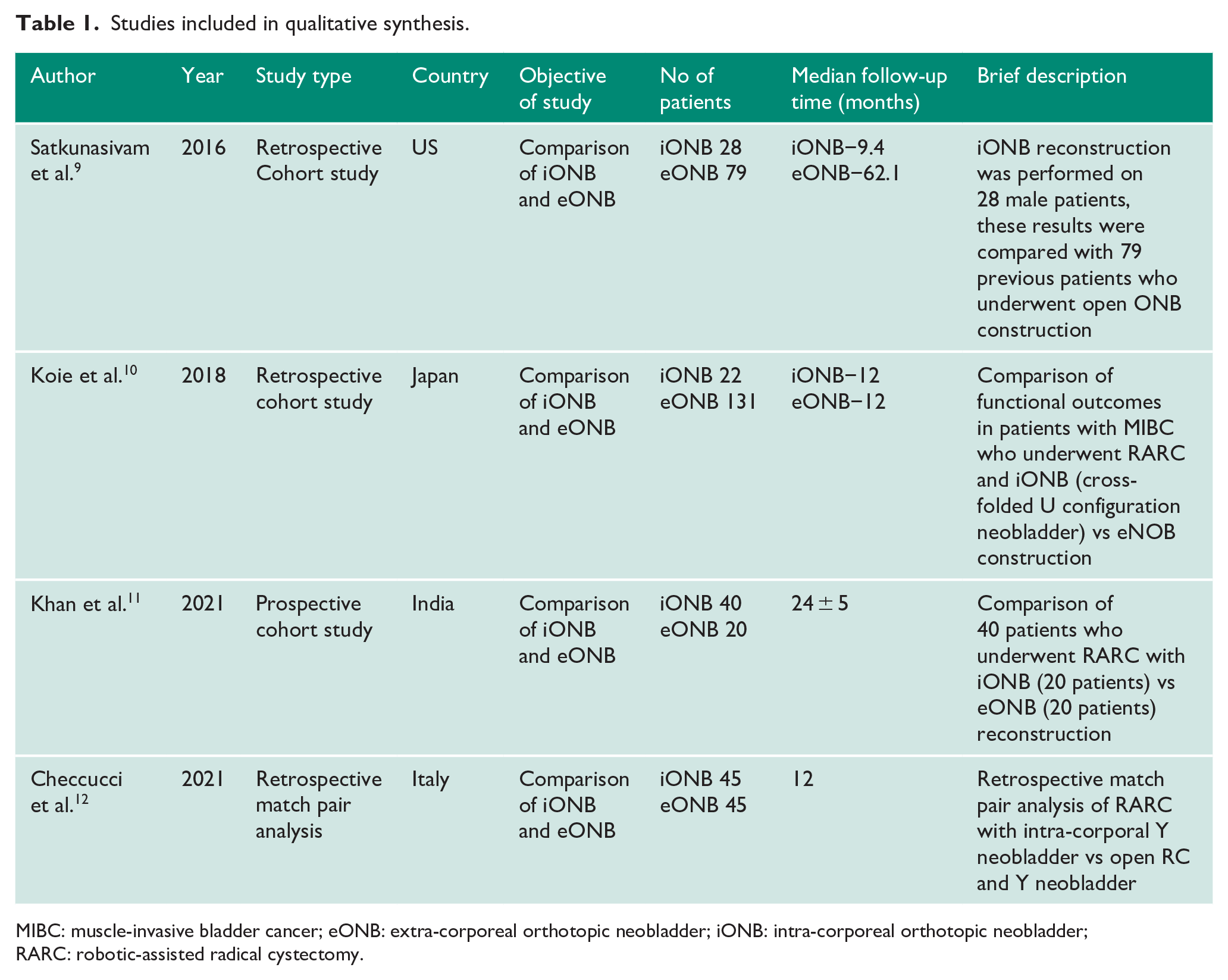
MIBC: muscle-invasive bladder cancer; eONB: extra-corporeal orthotopic neobladder; iONB: intra-corporeal orthotopic neobladder; RARC: robotic-assisted radical cystectomy.
Patient characteristics are displayed in Table 2. Limited data were available for ASA grade. Across the studies that reported on male-to-female ratios, the majority of patients were male (55.6%). The baseline characteristics in all studies did not show statistical significance between groups for age or body mass index; however, there was a significant difference in gender favouring males. Quality assessment using the NOS for assessing the risk of bias is available in Appendix 1. A score with a range of 0–9 was allocated to each study, and those with a score of 7 or more were considered to be higher-quality studies.
Patient characteristics.
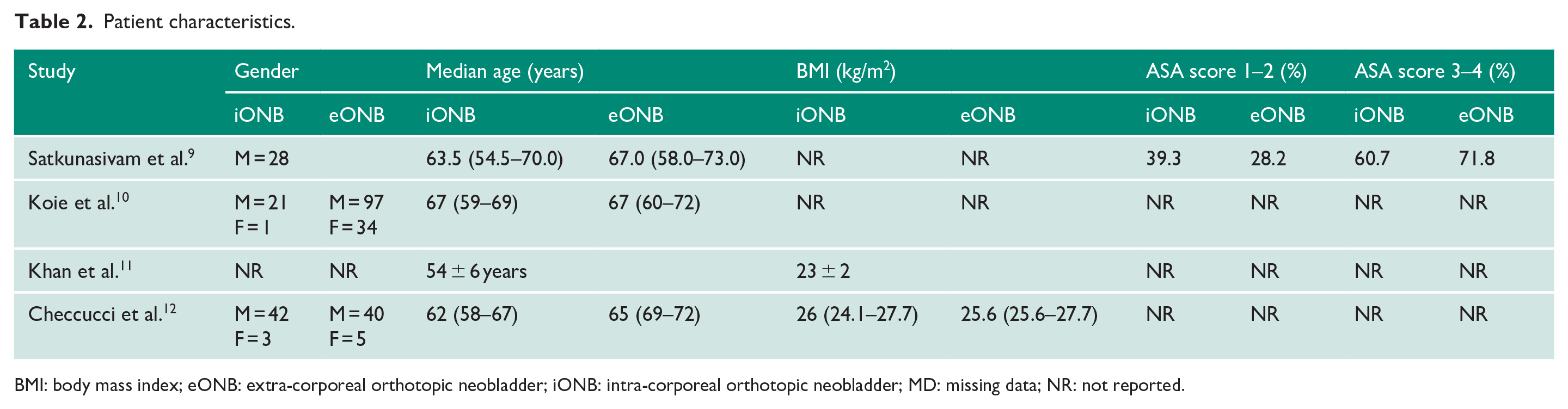
BMI: body mass index; eONB: extra-corporeal orthotopic neobladder; iONB: intra-corporeal orthotopic neobladder; MD: missing data; NR: not reported.
Neobladder reconstruction technique
Most iONBs were constructed using the Studer method, as reported by Khan et al., 11 who used this method for both approaches. A Y neobladder was constructed intra- and extra-corporeally in Checcucci et al. 12 Other techniques, for instance, the University of Southern California (USC) method, were adopted by Satkunasivam et al. 9 for both approaches, and Koie et al. 10 used the U-shaped neobladder technique for both approaches.
It is possible that the method of construction could have led to subtle differences in outcomes and could have impacted the accuracy of analysis due to variability in the type of neobladder constructed.
Functional outcomes
Most studies analysed, performed UDS on patients to assess the neobladder capacity. The results have been collated in a table for comparison and analysis (Tables 3–5). The UDS parameters included were mean bladder capacity, maximum flow rate and post-voiding residual volume (PVR).
UDS outcomes and continence rates of patients who underwent iONB reconstruction.
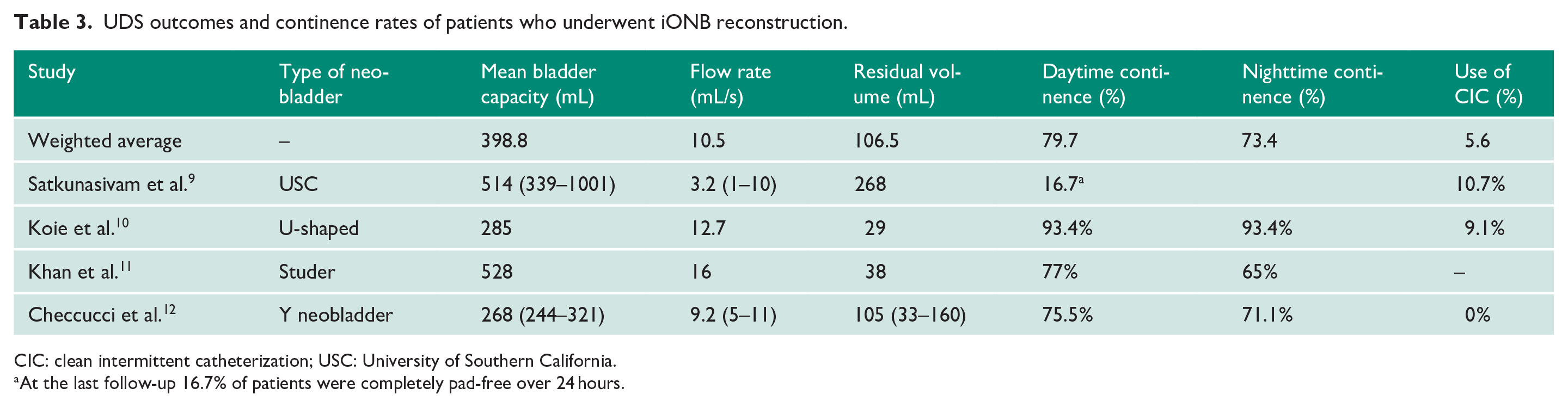
CIC: clean intermittent catheterization; USC: University of Southern California.
At the last follow-up 16.7% of patients were completely pad-free over 24 hours.
UDS outcomes and continence rates of patients who underwent eONB reconstruction.
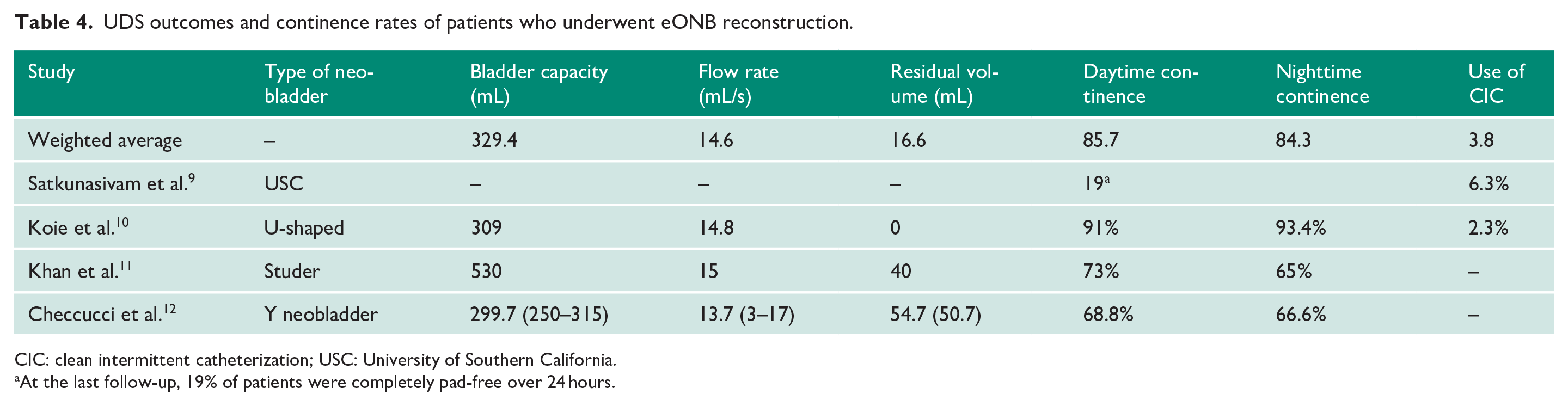
CIC: clean intermittent catheterization; USC: University of Southern California.
At the last follow-up, 19% of patients were completely pad-free over 24 hours.
UDS outcomes of papers comparing the iONB and eONB.
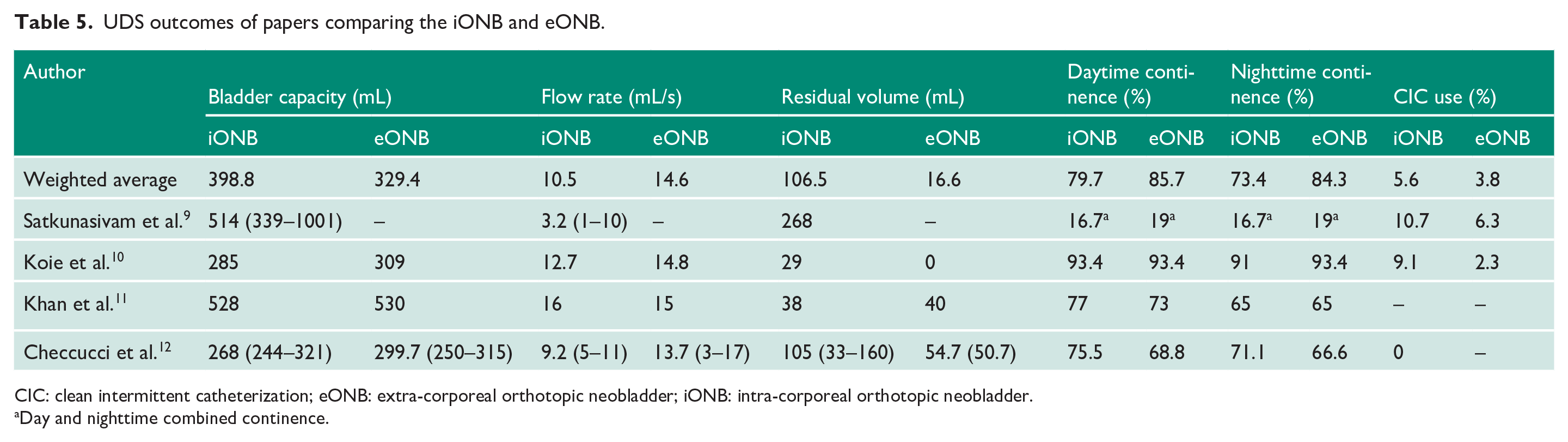
CIC: clean intermittent catheterization; eONB: extra-corporeal orthotopic neobladder; iONB: intra-corporeal orthotopic neobladder.
Day and nighttime combined continence.
Bladder volume
The mean iONB bladder volume was reported as 514 mL (range 339–1001) by Satkunasivam et al. 9 eONB outcomes were not discussed.
Koie et al. 10 reported the median capacity was higher with iONB than in the eONB cohort at 6 months (276 vs. 274 mL, respectively). However, the median capacity increased in both groups 12 months post-operatively (285 vs. 309 mL) with the higher capacity in the eONB study arm. These differences did not prove to be statistically significant.
UDS was performed one-year post-operatively in the study by Khan et al., 11 which showed that the eONB group had a higher bladder capacity of 530 versus 528 mL in the intra-corporeal group. Checcucci et al. 12 showed similar results with eONB reconstruction reporting a higher average capacity of 299.7 mL as compared to iONB with 268 mL (p = 0.049).
The weighted average calculated across studies showed that iONB had a higher bladder capacity of 398.8 versus 329.4 mL in eONB.
Flow rate
Satkunasivam et al. 9 reported a flow rate of 3.2 mL/s for the eONB cohort, a comparison to the open cohort was not made in this study. Koie et al. described peak flow rates of 12.7 m/s in the iONB group and 14.8 mL/s in the eONB group; however, the difference was not statistically significant. Khan et al. 11 showed no statistically significant difference in the flow rate between the eONB and iONB cohorts (15 vs. 16 mL/s, respectively). Checcucci et al. 12 reported higher flow rates in the eONB cohort (13.7 mL/s) compared to the iONB cohort (9.2 mL/s) (p = 0.002).
The weighted average of flow rate was lower in the iONB group 10.5 mL/s as compared to 14.6 mL/s in eONB.
Post-voiding residual volume
Satkunasivam et al.’s, 9 reported a mean PVR of 268 mL in the iONB cohort, results were not reported for the eONB cohort. Koie et al. 10 demonstrated the superiority of the eONB cohort with a median residual volume of 0 mL compared to the iONB cohort which was 29 mL at 12 months. Checcucci et al. 12 similarly illustrated superior results in the eONB cohort with a PVR of 54.7 mL compared to the iONB study arm which reported almost a 2-fold increased residual volume at 105 mL (p = 0.01).
Khan et al. 11 demonstrated similar results in both cohorts with residual volumes reported as 38 and 40 mL for the iONB and eONB cohorts, respectively.
The weighted average of residual volume in iONBs was higher 106.5 mL when compared to eONB 16.6 mL.
Day and nighttime continence
The day and nighttime continence rates were measured individually and compared. Incontinence was more likely to be seen in the nighttime, and this result was observed in all papers and both approaches.
Satkunasivam et al. 9 showed that 16.7% of iONB patients achieved full continence both day and night at the last follow-up, whereas 19% of eONB patients achieved the same result. These results were not statistically significant (p = 0.10). Conversely, Koie et al. 10 reported that iONB daytime versus nighttime continence was 97% versus 95%, whereas the eONB cohort showed 95% versus 94% continence, respectively. These results were not statistically significant.
Khan et al. 11 demonstrated in iONB patients that daytime continence was higher as compared to nighttime with 35% of patients needing pads at night (25% of which needed more than one pad in a night). Continence rate improved considerably as time passed, with 77% and 65% of iONB patients and 73% and 65% of eONB patients, using no pads (day and nighttime, respectively) one-year post-operatively. In addition, this study also reported that iONBs tend to achieve continence a lot quicker post-operatively. Checcucci et al. 12 also proved that iONB showed higher continence rates, in both daytime 75.5% versus 68.8% (p = 0.63) and nighttime 71.1% versus 66.6% (p = 0.81).
The weighted average of all the studies also demonstrated daytime continence of 79.7% and nighttime continence of 73.4% in iONB when compared to eONB counterparts having 85.7% and 84.3%, respectively.
Use of CIC
Satkunasivam et al. 9 reported that eONBs showed a lower (6.3%) percentage of CIC use as compared to iONB (10.7%) (p = 0.27); however, no difference was reported in the frequency or time from cystectomy to CIC use in either cohort. Koie et al. 10 reported similar results with 2.3% using CIC in the eONB cohort and 9.1% in the iONB cohort. Checcucci et al. 12 reported CIC use in none of their patients undergoing iONB; however, the rate of CIC use was not reported in the eONB cohort. No data were reported in the study by Khan et al. 11
A weighted average done across studies showed the opposite results with higher CIC use in eONB group 3.8% versus 5.6% in iONB.
Perioperative outcomes
Operative time was significantly longer in the iONB cohort compared to patients undergoing eONB, whereas estimated blood loss was more than two-fold higher in the eONB cohort. This was illustrated by a 9% rate of transfusion intra-operatively in this cohort compared to a 0% rate in the iONB cohort. Reoperation rates were not reported in those undergoing iONB; however, a rate of 13.7% was seen in those patients undergoing eONB. Length of stay was unfortunately only described in the iONB cohorts who reported a mean length of stay of 17 days (Table 6).
Perioperative outcomes of iONB versus eONB.
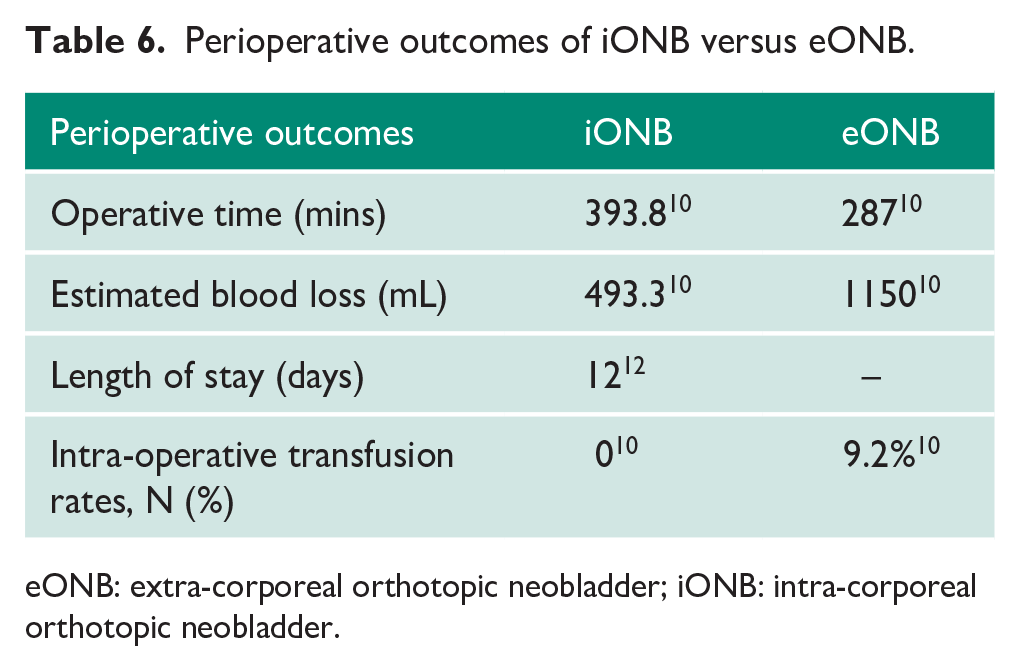
eONB: extra-corporeal orthotopic neobladder; iONB: intra-corporeal orthotopic neobladder.
Complications
Rates of ileus, surgical site infection and urinary leak were significantly lower in the iONB cohort. Rates of neobladder vaginal fistula, however, favoured the open method of neobladder construction. Rates of Urinary Tract Infection (UTI) were not reported in the iONB cohorts; similarly, rates of sepsis were not reported in the eONB cohorts (Table 7).
Complications of iONB versus eONB.
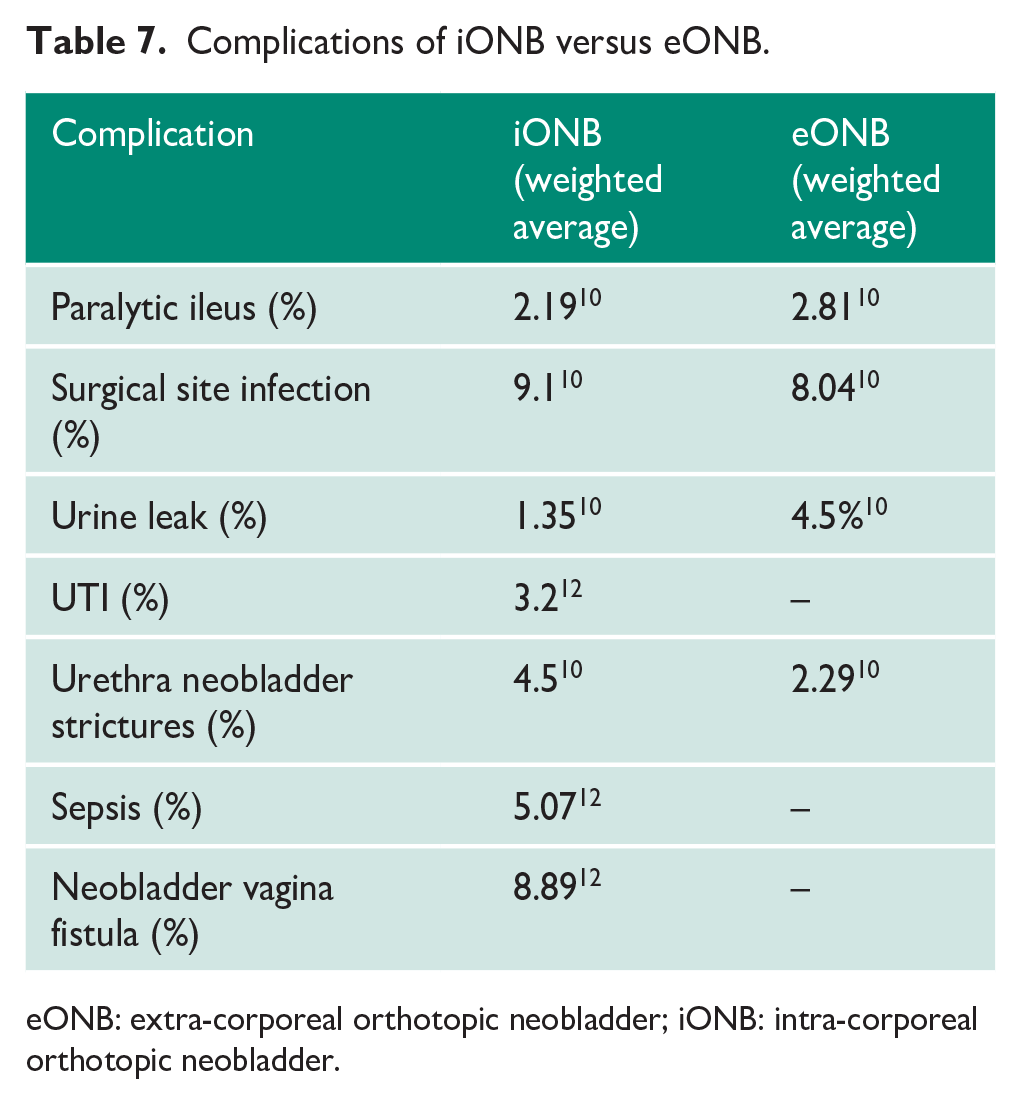
eONB: extra-corporeal orthotopic neobladder; iONB: intra-corporeal orthotopic neobladder.
Discussion
This systematic review summarised and compared the functional outcomes and complications of patients undergoing eONB and iONB utilising 4 studies reporting on a total of 410 patients. To the best of our knowledge, this is the first systematic review which has identified all relevant studies reporting on patient outcomes up until July 2022.
The main goal of ONB reconstruction surgery is to create an artificial bladder with an acceptable capacity, low-pressure intra-luminally and preserve the spontaneous voiding function of the patient while maintaining continence during the day and night. 5 Erectile function in the younger males is also vitally important. As the intra-corporeal technique gains popularity, it is vital to be able to adequately assess and evaluate the long-term functional and perioperative outcomes associated with the robotic construction of an ONB.
Our analysis has shown that eONBs tend to perform better functionally, showing lower residual volumes and higher flow rates. iONB, however, often achieved a higher mean bladder capacity; achievement of higher bladder capacity could theoretically translate into a reduced rate of lower urinary tract symptoms. This could be explained by the fact that this approach allows greater visibility, more manoeuvrability and better bowel exposure. However, it is important to consider that performing eONB is the traditional surgical technique of neobladder construction, and it is highly likely that surgeons have more experience in this method, translating into superior performance. This is furthermore reiterated by the shorter duration of surgery for the eONB approach. The novelty of robotic surgery and the learning curve associated with complex skills needed for the same also brings into question the experience of surgeons involved in the iONB studies and its subsequent impact on results. Only one study presented in our review reported the surgeon’s level of experience who reported them as being among the first cases in their institution. 9 The method of construction could also influence these results with varied techniques being used in the study making direct comparison difficult.
Current methods used for the urodynamic assessment of neobladders are identical to those used for patients with native bladders. This seems to be unsuitable given the use of bowel as a bladder substitute alters the normal storage and voiding mechanism. Variations in the urodynamic result and continence can be the result of the amount and type of bowel used as well as the method of construction. As the popularity of the neobladder approach increases a new criterion should be developed to assess the same. 11
Daytime and nighttime continence rates are great indicators of the functional outcomes of neobladders. Continence evaluation should be done at around 12 months post-operatively as studies have shown that neobladder maturity and optimum capacity are achieved at approximately 8 months. 13 Most studies selected in our review carried out UDS assessment of neobladder function at 3-month intervals, leading up to 12 months. Some studies only assessed the same at 12 months, whereas others continued to evaluate the same beyond the 12 months as well. These results should thus be interpreted with caution as the data were not recorded at the same time intervals. Our review demonstrated that iONBs had a higher rate of continence both during the day and night; they also seemed to achieve full continence a lot quicker than their eONB counterparts. This could be explained by the variation in the robotic technique itself, where the posterior wall of the neobladder is reconstructed and then the anastomosis between the urethra and bowel segment is made prior to the actual bladder construction, unlike the open technique. 14 Better visualisation in the robotic approach improves the accuracy of the anastomosis, ensuring a water tight seal. This often is supplemented by the ability to better preserve urethral length and the pelvic floor. 5
The possible utilisation of a nerve-sparing approach when performing radical cystectomy has desirable effects both for erectile function and continence. The selection of such patients for a nerve-sparing approach ultimately depends on both oncological factors and desired functional outcomes.
Another key point to consider is that the number of pads does not always reflect the degree of continence. This also fails to consider the discomfort or the satisfaction experienced by the patient and the effect it has on their QoL. A more wholistic measure would not only assess number of pads but also include details of the frequency and number of episodes of incontinence, size of pads used, weight of pads, and the inconvenience caused to the patient. 3 Thus, the development of a questionnaire to assess patient QoL would be an appropriate solution for future reference and aid in guiding patient treatment and comfort.
The rates of CIC among patients undergoing iONB were conflicting and no correlation was seen between residual volume and need for CIC. This may be explained by the practise that some surgeons constructing neobladders advise CIC regardless of residual volume.
There are several studies reporting case series for iONB and eONB techniques separately. These studies demonstrated similar results as that of our study. Obrecht et al. 15 also reported lower bladder capacities at 403.5 mL for iONB. In comparison, Lee et al. reported marginally higher bladder capacities for the eONB at 413.2 mL. Analysis of the eONB and iONB average flow rates showed mixed results3,15,16 but ultimately the figures were comparable. eONBs demonstrated a higher PVR3,16 as compared to iONBs. 15 A higher overall continence rate was seen in iONB as compared to eONB.3,13,15–17 When considering CIC use, iONBs13,15 reported a lower CIC rate as compared to eONB.4,16,17
Although limited data were available, it was clear in this review that both perioperative outcomes and complications favoured the iONB technique. The minimally invasive nature of the robotic approach no doubt helps minimise blood loss, need for transfusion and 30-day readmissions. Although length of stay was not reported across any of the studies reporting eONB outcomes, it is likely that this would be significantly higher in this cohort.
Although the conclusion of this review represents the best piece of evidence available in the literature, overall the evidence is moderate to weak. Some potential drawbacks must be taken into consideration. The most critical issue remains the impossibility of controlling for surgical skill and individual-related factors in determining outcomes following neobladder surgery. There were only 4 comparative studies which were all non-randomised, and although they were rated as either satisfactory or good, these study designs are susceptible to bias. This was the main reason for downgrading the quality of evidence. We accept that the low number of studies in this review limits the strength of our results.
This review has identified that there is no standardised technique for neobladder construction, with different periods of follow-up and varied reported outcome measures which makes comparison difficult. It is essential that more prospective randomised control trials are performed with an adequate follow-up time, more clearly defined outcomes and an established criterion for assessment. A consensus must be reached in the way studies report their results in a standardised fashion as this would no doubt address the importance of patient specific outcomes, allowing patients to make a more informed decision about the surgical approach.
Conclusion
Although the robotic technique is still relatively new, it is being adopted rapidly at specialist centres due to the perceived advantages of lower complication rate and better continence. It is, however, essential that patient follow-up is continued, and more neobladder-specific criteria for urodynamic assessment are developed to be able to adequately assess and compare long-term outcomes with this method.
More randomised control trials comparing the two techniques are vital to assess long-term outcomes and provide an evidence-based decision-making tool for better patient care.
Footnotes
Appendix 1
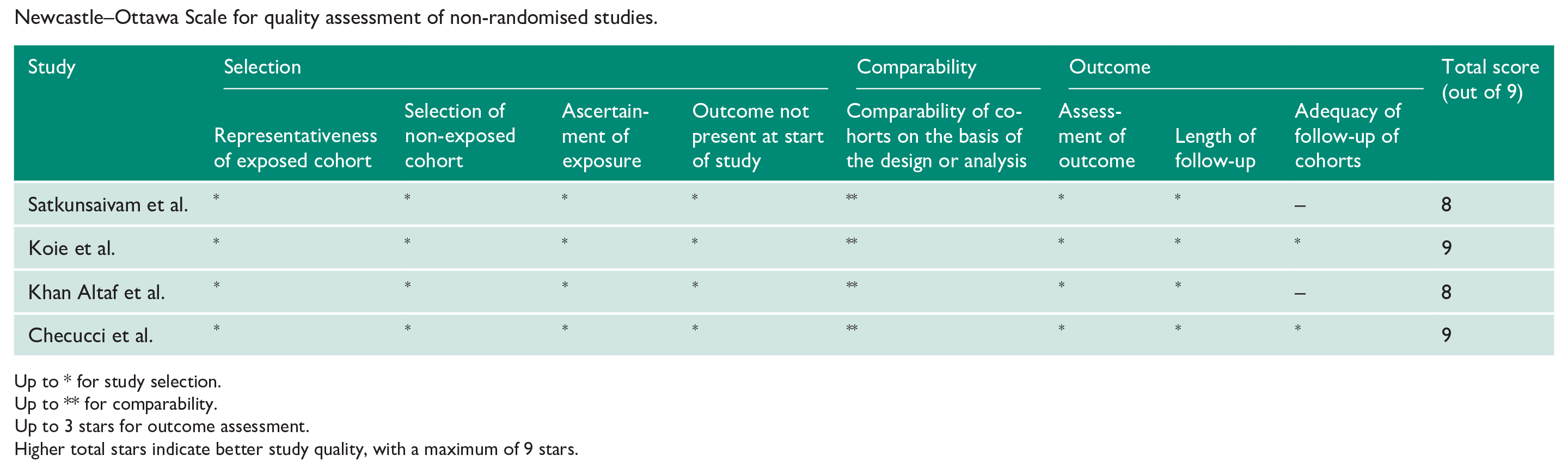
Newcastle–Ottawa Scale for quality assessment of non-randomised studies.
| Study | Selection | Comparability | Outcome | Total score (out of 9) | |||||
|---|---|---|---|---|---|---|---|---|---|
| Representativeness of exposed cohort | Selection of non-exposed cohort | Ascertainment of exposure | Outcome not present at start of study | Comparability of cohorts on the basis of the design or analysis | Assessment of outcome | Length of follow-up | Adequacy of follow-up of cohorts | ||
| Satkunsaivam et al. | * | * | * | * | ** | * | * | – | 8 |
| Koie et al. | * | * | * | * | ** | * | * | * | 9 |
| Khan Altaf et al. | * | * | * | * | ** | * | * | – | 8 |
| Checucci et al. | * | * | * | * | ** | * | * | * | 9 |
Up to * for study selection.
Up to ** for comparability.
Up to 3 stars for outcome assessment.
Higher total stars indicate better study quality, with a maximum of 9 stars.
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent and ethical approval
Since this paper is an analysis of retrospective data, patient consent or ethical approval was not required.
Guarantor
V.H.
Contributorship
All authors contributed to planning of the study. Suitable studies were selected by M.B. and O.E.-T. Any disagreement in study selection was resolved by V.H. Data collection was performed by M.B. Data presentation, quantification and analysis were performed by all authors. The first draft of the manuscript was produced by M.B. Following drafts were discussed and edited by all authors. All authors are in approval of the final manuscript.