
Abstract
Objective:
We assessed the safety and feasibility of minimally invasive robot-assisted surgery for horseshoe kidney (HSK).
Method:
A prospectively maintained data set for consecutive patients undergoing robotic kidney surgery was reviewed for patients with HSK. Cases were performed by experienced robotic surgeons, across two high-volume centres between 2016 and 2020.
Results:
Seven patients underwent robotic surgery for HSK, comprising three partial nephrectomies for renal masses, one nephroureterectomy and three benign nephrectomies for non-functioning kidneys. The median age was 53 (interquartile range (IQR) = 47–60) years and median body mass index (BMI) was 25 (IQR = 25–26.5). Median console time was 120 (IQR = 118–215) minutes and median estimated blood loss was 150 (IQR = 125–250) mL. The median pre- and post-operative estimated glomerular filtration rate (eGFR) was 76 (IQR = 72–90) and 71 (IQR = 60–81), respectively. There were no higher-grade complications (Clavien–Dindo III–IV) and one Clavien–Dindo grade II complication (wound infection treated with IV antibiotics). Median length of stay (LOS) was 2 days and there were no 30-day readmissions. Negative margins were achieved in 75% of tumour resections.
Conclusion:
We report one the largest series of robot-assisted surgery on HSK. Robotic surgery is safe and feasible for HSK in centralised high-volume centres with acceptable perioperative outcomes. Established benefits of minimally invasive surgery, such as reduced LOS and low complication rates, were demonstrated.
Level of evidence:
4
Introduction
Genitourinary tract abnormalities are one of the most common birth defects, affecting as many as 10% of births. 1 Of this cohort, horseshoe kidneys (HSKs) represent the most common fusion abnormality of the urinary tract (90%). 2 The incidence of HSK is reported as 1 in 400–600 individuals and it is present twice as frequently in men.1,3
Due to the anatomical and procedural complexity, surgery has traditionally been performed through an open approach. Laparoscopy has offered a minimally invasive approach; however, due to aberrant vasculature, the parenchymal isthmus and abnormal location, 4 this remains a technically challenging operation. The advent of robotics has allowed operating on patients with HSK via a minimally invasive approach while reducing some of the technical difficulty associated with laparoscopic surgery. Robotic surgery has been widely adopted in the field of urology and has shown superior perioperative outcomes compared with open surgery for operations on the kidney, bladder and prostate. 5 Robotic surgery has also been shown to improve perioperative outcomes in complex urological surgery due to better vision, enhanced dexterity and better tissue handling. 6 However, due to the technical complexity and rare nature of HSK abnormalities, outcomes for robotic surgery for patients with HSK have not been described.
The aim of this study was to assess the safety and feasibility of robot-assisted surgery for HSK, describing procedural and post-operative outcomes.
Methods
Study design and data collection
We interrogated a prospectively maintained data set of patients undergoing robot-assisted surgery in two high-volume centres in the United Kingdom between May 2016 and February 2020 to identify patients with HSK. All operations were carried out by three high-volume robotic surgeons.
Demographic data collected included age, body mass index (BMI), sex and indication for surgery. Perioperative data included American Society of Anaesthesiologists (ASA) physical status score, pre- and post-operative estimated glomerular filtration rate (eGFR), conversion status, estimated blood loss (EBL), operative time, console time, length of stay (LOS) and 30-day Clavien–Dindo complication rate. 7 Oncological data, where indicated, included histology, tumour location, maximum diameter of lesion, tumour grade and surgical margin status.
Surgical technique
All patients were assessed using renal protocol triple-phase computed tomography (CT) and the images were used to produce three-dimensional (3D) reconstructions (Figure 1) to aid in pre-operative planning and identification of vasculature and tumour location, where appropriate.
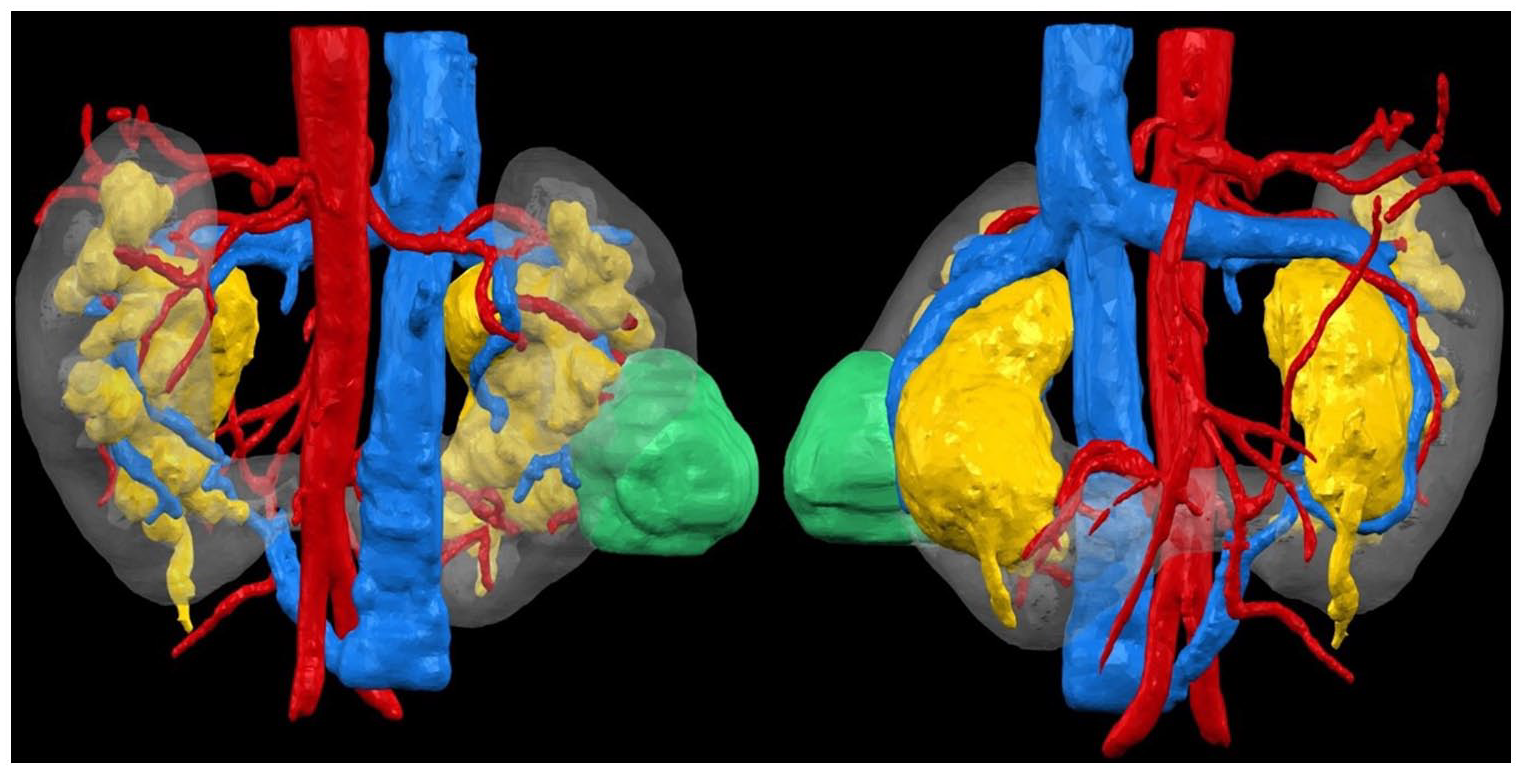
Three-dimensional reconstruction using renal protocol triple-phase CT in a patient with a right lower pole tumour. (Left) posterior view; (right) anterior view.
All operations were performed using the Intuitive da Vinci Xi surgical robotics system. Patients were placed in a lateral flank position, with a 10° table flexion at the level of the umbilicus.
A pneumoperitoneum was achieved using a Veress needle, with the position of the robotic and assistant ports subsequently marked out in a standard configuration. The camera port was inserted first via an 8 mm incision and the remaining robotic ports (8 mm) and assistant port (12 mm) were placed under vision. On the right side, an additional 5 mm port was used to allow liver retraction if necessary (Figure 2). Insufflation pressures were maintained at approximately 12 mmHg, with a trend towards lower pressures when using the Airseal system. HSKs present as unique cases of complex anatomy with characteristic abnormalities in ectopia, malrotation (ventrally opening hilum and ventrally descending ureters) and vasculature.3,8 In addition, the isthmus can be a fibrous band, dysplastic or of functional parenchyma, which makes division more difficult and limits mobility during surgery. 8 Scanlon robotic vascular clamps were used where necessary and an early de-clamping technique used as the default with two-layer renorrhaphy. All the surgical specimens were bagged and the bag was removed from the umbilical extraction port site.
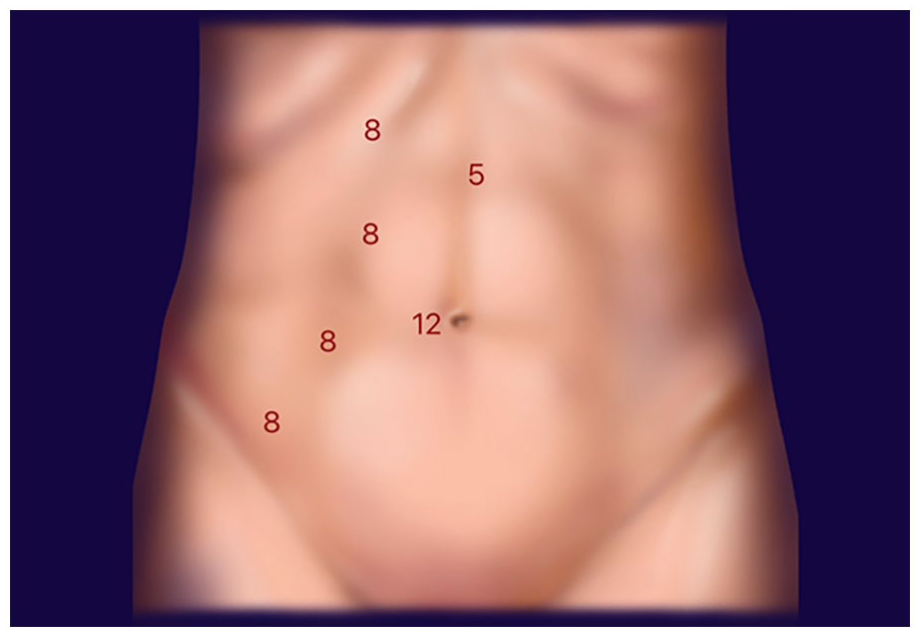
Standard robotic port placement for a right-sided HSK operation, with four 8 mm ports for the Da Vinci Xi’s four arms, a 5 mm port for a liver retractor and a 12 mm assistant port.
Statistical analysis
Data collection, tables and figures were completed using Microsoft Excel 2019. Statistical analysis was done using SPSS 26th 168 Edition, IBM. Descriptive data are reported as median and interquartile range.
Results
Patient characteristics
Across two centres, a total of seven (four females and three males) patients were operated on between May 2016 and February 2020 (Table 1) by three experienced robotic surgeons. The median age at surgery was 53 years with a median BMI of 25.0 kg/m2 and median ASA score of 2. Full patient characteristic data are presented in Table 1.
Patient and oncological characteristics.
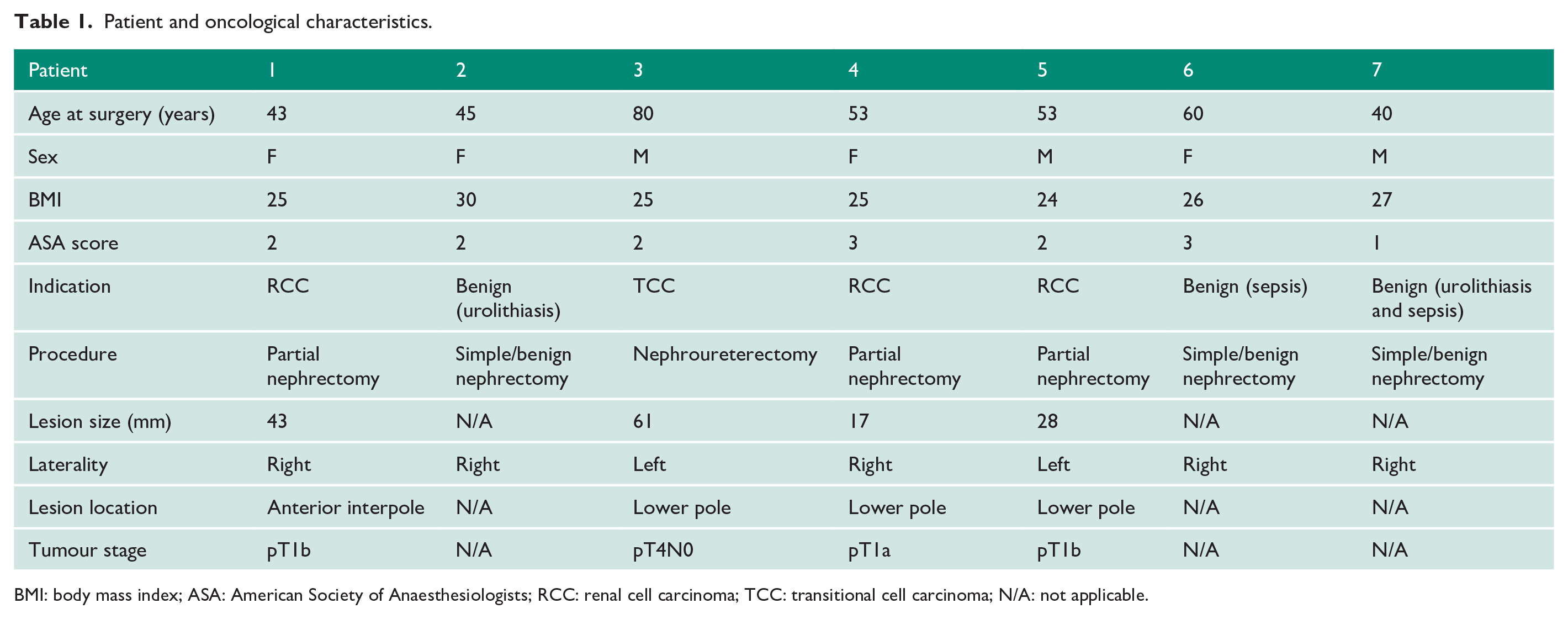
BMI: body mass index; ASA: American Society of Anaesthesiologists; RCC: renal cell carcinoma; TCC: transitional cell carcinoma; N/A: not applicable.
Surgical management
Decision for surgical management was ratified for all patients in a dedicated specialist renal tumour board meeting. Surgical planning took place in a dedicated planning meeting using a 3-dimensional (3D) reconstruction of the HSK (Figure 1). ‘Innersight labs’ use software to generate 3D images with vascular and lesion details from a standard renal protocol CT negating the need for the additional radiation of a CT angiogram. 9 The 3D imaging allows planning for surgical approach, resection and reconstruction strategies, accurately mapping the aberrant vasculature as well as tumour location and depth. It also allows planning for mobilisation of the lesion having mapped the surrounding important structures such as major vessels and the ureter. All patients underwent robot-assisted surgery, with three partial nephrectomies for renal masses, one nephroureterectomy for suspected urothelial cancer and three benign nephrectomies for non-functioning kidneys (secondary to urolithiasis or recurrent urinary tract infection (UTI) and sepsis).
Perioperative outcomes
Robot-assisted surgery was technically feasible in all cases. No cases required open conversion. The median operative time was 170 minutes, with a median console time of 120 minutes (Table 2). The median warm ischaemia time (WIT) was 25 minutes. Median EBL was 150 mL. No patients required blood transfusion. One patient had a Clavien–Dindo grade II complication (soft tissue wound infection treated with intravenous antibiotics); they were discharged on day 5 post-operatively. There were no higher-grade Clavien–Dindo complications. The median LOS was 2 days, with no readmissions within 30 days. All operations were deemed a technical success.
Perioperative and oncological outcomes.
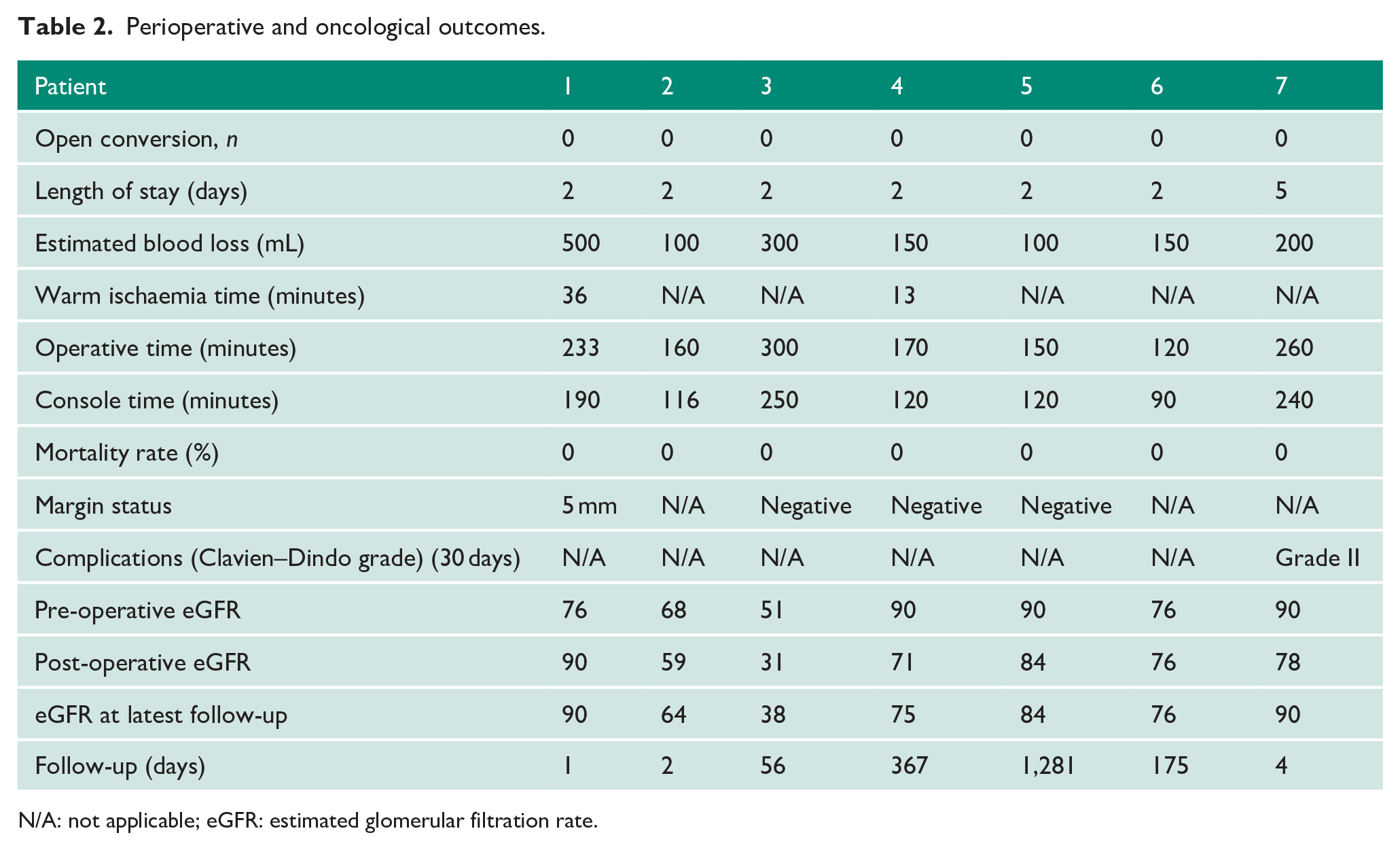
N/A: not applicable; eGFR: estimated glomerular filtration rate.
Oncological outcomes
Final histology for all patients demonstrated three clear cell renal cell carcinomas (RCCs) and one transitional cell carcinoma (TCC). Negative surgical margins were achieved in three of four patients. One patient had a positive surgical margin (PSM) of 5 mm after resection for clear cell RCC with a Leibovich score of 2 (low risk). At last follow-up, 6 months post-operatively, there was no recurrence or metastases. Full perioperative and oncological data are presented in Table 2.
Physiological outcomes
For patients undergoing nephrectomy for non-functioning kidneys, median pre- and post-operative eGFR was 76 and 76 mL/min/1.73 m2, respectively. For patients undergoing nephrectomy or nephroureterectomy for renal masses, median pre- and post-operative eGFR was 83 and 78 mL/min/1.73 m2, respectively. The greatest immediate post-operative decline in eGFR was 20 mL/min/1.73 m2 for the patient who underwent nephroureterectomy. Median decline in eGFR for patients with renal masses went from 5 mL/min/1.73 m2 immediately post-operatively to 1 mL/min/1.73 m2 at last follow-up (median: 212 days).
Discussion
Traditionally, due to the complex anatomy of a HSK, operating on HSK has been through the open approach. 10 Limitations with laparoscopic equipment and set-up, and tumours that are large, in an unfavourable location within the HSK and in an unclear location with respect to vasculature and the renal collecting system have meant that open surgery has largely been used 11 and still remains the gold standard in the management of renal tumours. 12 Previous series mainly report surgery in groups of patients undergoing open surgery.13,14 In this study, we report on a contemporary cohort of patients undergoing robotic surgery in two high-volume institutions.
In a comparative study between open partial nephrectomy (OPN), laparoscopic partial nephrectomy (LPN) and robot-assisted partial nephrectomy (RAPN) in anatomically normal kidneys, Porpiglia et al. found that while OPN had the shortest WIT, RAPN had significantly shorter WIT compared with LPN and showed significantly lower EBL compared with OPN and LPN. RAPN was significantly less morbid than OPN with regard to intra-operative and post-operative complications, and there was a non-significant decrease in PSM compared with OPN. 15 Porpiglia et al. 15 defined trifecta in partial nephrectomy as the absence of perioperative complications, negative surgical margins, and ischaemia time < 25 minutes, and reported that this occurred in 62.4%, 63.2% and 69.0% for OPN, LPN and RAPN, respectively.
With the successful outcomes associated with RAPN, complex cases are no longer being left for open surgery. More complex cases, such as HSKs, are being performed robotically (Supplementary Table 1). Petros et al. 16 reported a series of 101 robot-assisted laparoscopic nephrectomies and found that outcomes were consistent regardless of the complexity of the procedure. Completion of the procedure without the need for open conversion was possible even in the most complex procedures involving vascular and organ invasion. 16
Since the first report of robotic surgery in HSKs in 2005, 17 there have been increasing reports of this approach in HSKs (Supplementary Table 1). To our knowledge, this is one of the largest reported case series of robot-assisted surgery in HSKs. Roussel et al. 18 in a multi-centre collaboration reported management and outcomes of renal tumours in 40 HSK patients, 7 of which were managed using robotic assistance. Among their minimally invasive surgery (MIS) cohort (laparoscopic: n = 1, robot-assistance: n = 7), they report similar maximum tumour diameter and operative time, shorter WIT, but greater EBL and LOS to our data.
The largest series of laparoscopic surgery for renal masses in HSKs also report complications no greater than Clavien–Dindo grade 2. 19 While the first laparoscopic nephrectomy was reported as early as 1991, only a handful of LPN in HSKs has been reported.10,19–22 While LPN has been shown to be as effective as OPN, by offering comparable long-term oncological and functional outcomes,23,24 its use in HSKs is limited due to the aberrant vasculature and parenchymal isthmus, making attaining haemostasis a major complication during surgery and also leading to longer WIT. 25
The lack of collateral blood supply and aberrant nature of HSK vasculature increases the likelihood of surgical complications. 26 Following the initial report of the vascular anatomy of HSKs by Graves in 1969, it is accepted that the aberrant vasculature of HSKs compared with anatomically normal kidneys makes accurate identification difficult. 27 Three-dimensional reconstructions (Figure 1) aided our pre-operative understanding of vasculature through easy visual interpretation, eliminating any error-prone cognitive reconstruction of CT scans (Figure 3), and allowed for enhanced pre-operative planning to avoid any vascular injuries. In a multi-centre analysis of 886 RAPN patients by Tanagho et al., 28 it was identified that intra-operative and post-operative haemorrhage occurred in 1.0% and 5.8% of patients, respectively, with 4.6% of patients requiring a post-operative blood transfusion. In our series, we report zero vascular complications. In addition, a recent multi-centre review by Roussel et al. 18 suggested that advanced imaging techniques utilising 3D reconstruction may help with the need for meticulous pre-surgical planning when operating on HSK. In their series of 40 patients, only 2 had 3D reconstruction. In our series, we have demonstrated that 3D reconstruction can be a useful adjunct to help with pre-operative planning and lead to acceptable complication rates comparable with published literature.
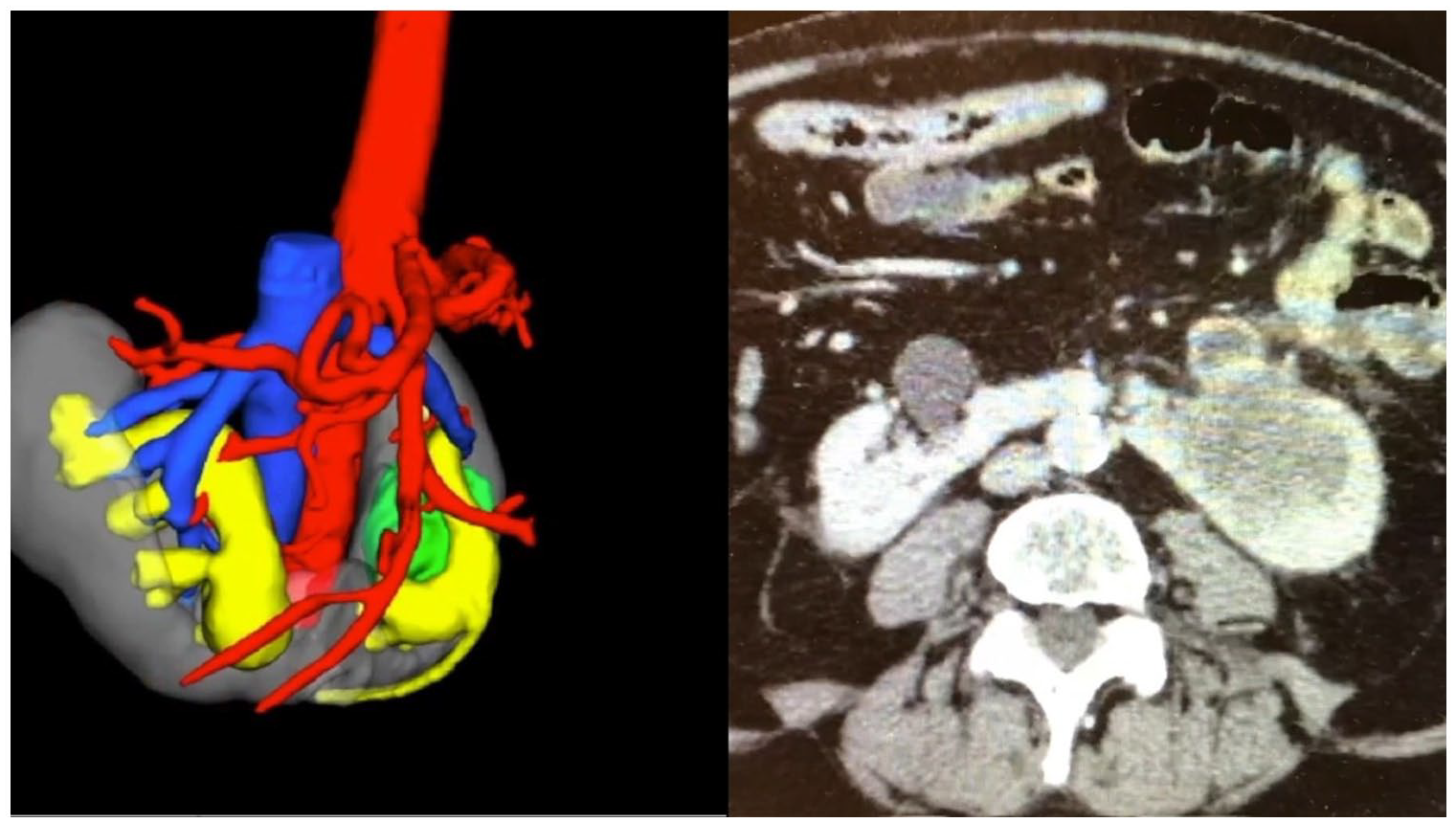
Comparative illustration in a patient with a left lower pole tumour. (Left) 3D reconstruction using renal protocol triple-phase CT; (right) CT.
Our series shows comparable perioperative results to similar studies reporting robot-assisted nephrectomy (partial or heminephrectomy) and nephroureterectomy (Supplementary Table 1). In addition, our complication rate and median LOS are comparable with the reported literature – only one patient suffered a complication which was reported as a Clavien–Dindo grade II and our median LOS was 2 days; there are only two complications reported in the literature, a Clavien–Dindo grade II and grade IIIb complication18,29 and the reported median LOS reported in the literature is 2 days (Supplementary Table 1).
Acknowledging that this is a heterogeneous cohort of patients with HSK, our median operating and console time of 170 and 120 minutes, respectively, are shorter and in keeping with the median operating and console times of 177 and 157 minutes, respectively, as reported in the literature (Supplementary Table 1). The use of 3D reconstruction in all our patients may have contributed to this shortened duration, which enabled pre-operative planning and less time for intra-operative vessel and lesion identification and dissection. One patient however had a PSM of 5 mm after resection for clear cell RCC with a Leibovich score of 2 (low risk).
Our study is not without its limitations, with the small sample size being the foremost. However, HSKs have a reported frequency of 1 in 400–600 individuals. There is a higher risk of developing UTIs and urolithiasis in HSK due to poor drainage and these conditions are adequately managed medically or endoscopically. Although nephroblastoma and TCC are reported more commonly, the incidence rate of RCC is comparable with the general population. 30
In addition, surgery has traditionally been through the open approach and subsequently performed laparoscopically. In addition, the uptake of robotic surgery limits the number of cases performed robotically. Proven its safety and feasibility, we hope that more series like ours will support robot-assisted surgery in HSKs in preference to the open approach.
The retrospective nature of our data interrogation would carry an inherent bias; however, the databases in our institutions are maintained prospectively. In addition, discharge summaries, clinician follow-up letters and investigations reported on Electronic Patient Records were sourced to complete the outcome data. Furthermore, our intension was not to compare the current standard (open surgery) against robot-assisted surgery, as this would require a multi-centre endeavour to sufficiently power such a study. On the other hand, the strength of the study is that the operations were performed by high-volume robotic surgeons, all of whom are beyond their learning curve for robot-assisted renal surgery.
Conclusion
Robotic surgery in HSK is both safe and feasible in high-volume tertiary referral centres. The use of a robot provides all benefits of MIS to the HSK patients maintaining good functional and oncological outcomes. This technically challenging procedure due to vascular and anatomical variations can be accurately planned and precisely executed with a combination of 3D reconstruction and robotic interphase.
Supplemental Material
sj-docx-1-uro-10.1177_20514158221088451 – Supplemental material for Robot-assisted surgery in horseshoe kidneys: A safety and feasibility multi-centre case series
Supplemental material, sj-docx-1-uro-10.1177_20514158221088451 for Robot-assisted surgery in horseshoe kidneys: A safety and feasibility multi-centre case series by Alexander Ng, Arjun Nathan, Nicholas Campain, Mariella Fortune-Ely, Siddhant Patki, Yuigi Yuminaga, Faiz Mumtaz, Aziz Gulamhusein, Maxine Tran, Senthil Nathan, Ravi Barod, Axel Bex and Prasad Patki in Journal of Clinical Urology
Footnotes
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical approval
All patients were registered as part of an institutional department audit at both the Royal Free Hospital and University College London Hospital. As a registered audit, NHS Research Ethics Committee (REC) was not required. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000.
Informed consent
All patients gave informed signed written consent as best known at the time of intervention after discussion with the relevant surgeon and multi-disciplinary team to undergo the operation.
Guarantor
P.P.
Contributorship
A.Ng was involved in protocol/project development, data collection or management, data analysis, and manuscript writing. A.N. was involved in data collection or management, manuscript writing and editing. N.C. was involved in manuscript writing and editing. M.F.-E. was involved in data collection or management, and data analysis. S.P. was involved in data collection or management, and data analysis. Y.Y. was involved in protocol/project development. F.M. was involved in protocol/project development. A.G. was involved in protocol/project development. M.T. was involved in protocol/project development. S.N. was involved in protocol/project development. R.B. was involved in protocol/project development. P.P. was involved in protocol/project development, manuscript writing and editing. A.B. was involved in protocol/project development, manuscript writing and editing.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.