
Abstract
Objective:
Developing a simple, user-friendly objective severity scoring system for symptomatic benign enlargement of prostate (BEP) and comparing with International Prostate Symptom Score (IPSS).
Subjects and Methods:
In this prospective study, patients with BEP completed IPSS proforma. A grading system was developed for peak flow of urine (Qmax), transitional zone index (TZI), detrusor wall thickness (DWT) and intravesical prostatic protrusion (IPP). Prostate Disease Severity Score (PDSS) was developed as sum of the variables.
Results:
Among 115 patients, obstructive voiding (70.43%) was predominant symptom followed by storage symptom (10.44%). Among predominant obstructive voiders, grades 1–3 TZI was common (97.53%), followed by IPP (64.19%) and DWT (62.96%) of varying grade. IPP, DWT, TZI and Qmax proved to be strong determinants of obstructive voiding (p < 0.05). The components of PDSS correlated well with total score (p < 0.05), positively correlated with IPP, DWT and TZI, and negatively with Qmax (p < 0.05); correlation with IPSS was statistically significant (p < 0.05). According to PDSS, 92.5% (37/40) patients with severe, 73.02% (46/63) with moderate, 8.33% (1/12) with mild degree of obstruction needed surgical intervention.
Conclusion:
The objective nature, comparable correlation with IPSS, potentiality to predict future need for surgical intervention, makes PDSS, a potential user-friendly assessment tool in management of BEP.
Level of evidence:
Not applicable
Keywords
Introduction
Benign prostatic hyperplasia (BPH) is a common ailment in ageing men. Presently, bothersomeness of symptoms in benign enlarged prostate (BEP) or BPH dictates its management. The International Prostate Symptom Score (IPSS) is a subjective severity score, which depends on the threshold of an individual to perceive the bothersomeness. The IPSS is not used for the diagnosis of BPH, but as a tool to categorise baseline symptom severity, to determine treatment response, or disease progression during follow-up of patients either on treatment or watchful waiting. Disadvantages of IPSS include mathematical calculation, recall of symptoms of 4 weeks. 1 Besides, misreporting is frequent (≈58%) in patients with <9 years of schooling. 2
The Visual Prostate Symptom Score (VPSS), a validated tool 3 has pictorial representation of symptoms and used for subjective assessment. The New upgraded VPSS, on par with IPSS, has potential to replace IPSS as a simple symptom assessment tool due to ease of applicability. 4 However, both IPSS and VPSS are entirely based on patients’ perception of symptoms and bothersomeness.
Hence, understanding the need for an objective assessment tool for guidance in planning appropriate management by identifying the beneficiaries from surgical intervention we attempted to develop and validate an objective severity grading system comparable and on par with IPSS, but address the limitations of subjective bias of the latter.
Subjects and methods
This prospective study was conducted by the Department of Urology of a Tertiary Care Teaching Hospital in South India, during July 2013 to July 2016, after obtaining approval from the Institutional Ethics Committee. Pro-spective patients were screened from the patient pool attending the out-patient department, after obtaining written informed consent.
The aim of the study was to develop and validate an assessment tool for BEP using objective parameters, peak urine flow rate on uroflowmetry (Qmax), 5 intravesical prostatic protrusion (IPP), 6 transitional zone index (TZI) 7 and detrusor wall thickness (DWT). 8 Developing and validating objective Disease Severity Score as an objective assessment tool for BEP was the primary objective; to develop a grading system and a scoring system for symptom variables of BEP, categorising the patients as per scoring system and comparing with IPSS grading were the secondary objectives.
All patients with symptomatic BEP were included. Those with urethral stricture, previous urethral/prostatic surgery, pelvic irradiation, neurological causes of bladder outlet obstruction (BOO), serum prostate-specific antigen (PSA) >4 ng/mL, voided volume of urine <150 mL, vesical calculus, cystitis/urinary tract infection, diabetes mellitus and known case of bladder carcinoma were excluded.
After obtaining detailed medical history, clinical examination along with digital rectal examination (DRE) was carried out in all and IPSS charts were provided to the patients, which were assessed by the same urologist. Apart from the routine haematological and biochemical investigations, serum PSA, uroflowmetry, ultrasound abdomen and pelvis for prostate volume (PV), IPP, DWT, post-void residual urine volume (PVR), trans rectal ultrasound (TRUS) for TZI were performed. Magnetic resonance imaging (MRI) was not used to estimate prostate size.
Obstruction was defined as Qmax of <15 mL/seconds, when taken into consideration along with raised IPP, TZI and DWT. Mariappan et al. 6 had described grading for IPP. Building upon this, we propose grading to Qmax, TZI and DWT.
Prostate Disease Severity Score
We designed a new scoring system with four components – IPP, Qmax, DWT and TZI. Total severity score varied from 0 to 12 with each component of scoring system having a score of 0–3 (Table 1). BEP was categorised into mild (score 0–2), moderate (score 3–6) and severe (score 7–12) obstruction (Table 1).
New grading system for variables in PDSS.
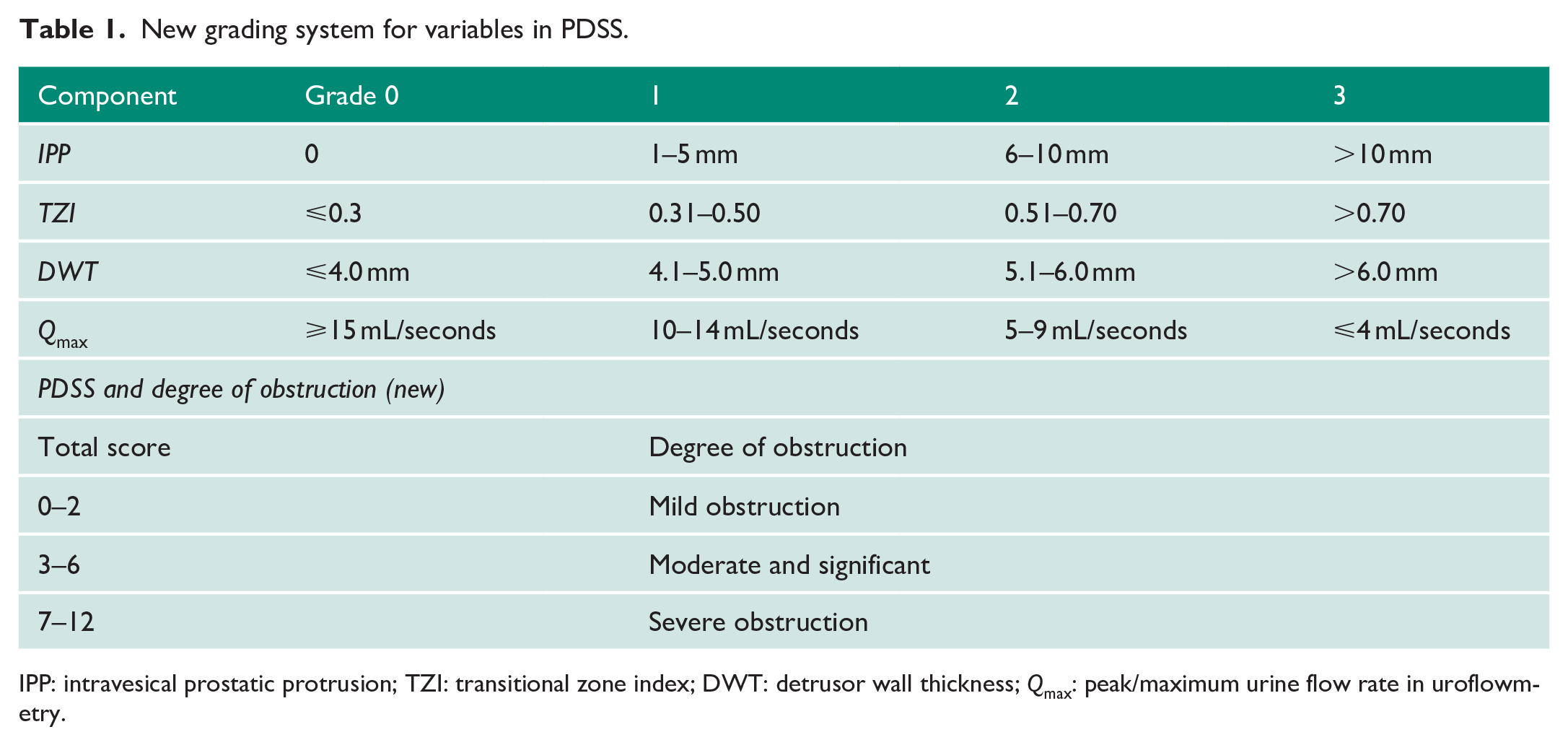
IPP: intravesical prostatic protrusion; TZI: transitional zone index; DWT: detrusor wall thickness; Qmax: peak/maximum urine flow rate in uroflowmetry.
Statistical analysis
Pearson’s correlation coefficient and Student’s t-test (paired) were used. p-value of < 0.05 was considered significant. Descriptive statistics (mean values, standard deviation (SD), median, percentage and range), tables and figures were used as appropriate. Statistical package for social science (SPSS) V17.0 was used for analysis.
Results
One hundred fifteen males with symptoms attributable to BEP, meeting the selection criteria, were included. Forty-nine (42.60%) were aged 61–70 years, 33 (28.69%) were aged 51–60 years (28.69%) and 24 (20.87%) were aged 71–80 years. The details of age, clinical assessments and laboratory parameters are provided in Table 2.
Demography, relevant clinical and laboratory investigations.
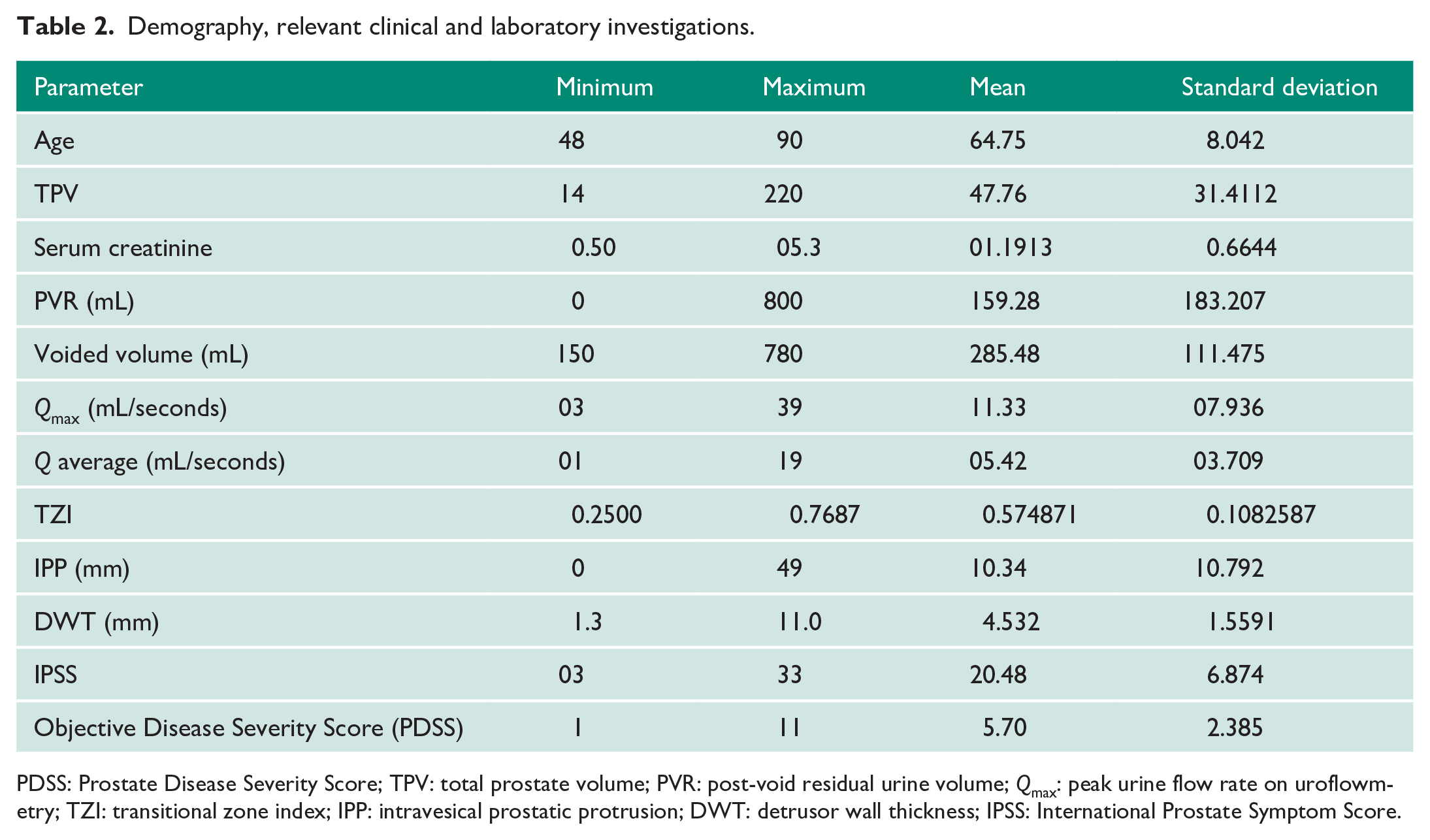
PDSS: Prostate Disease Severity Score; TPV: total prostate volume; PVR: post-void residual urine volume; Qmax: peak urine flow rate on uroflowmetry; TZI: transitional zone index; IPP: intravesical prostatic protrusion; DWT: detrusor wall thickness; IPSS: International Prostate Symptom Score.
Eighty-one (70.43%) patients had predominant obstructive voiding symptoms, 12 (10.44%) had predominant irritative/storage, and 22 (19.13%) had both irritative and obstructive voiding symptoms. Among those with predominant obstructive voiding, 97.53% (79/81) had grades 1–3 TZI, 64.19% (52 of 81) had IPP of varying degree and 62.96% (51/81) had grades 1–3 DWT.
Both IPSS and Prostate Disease Severity Score (PDSS) were applied to categorise the patients to three categories. In IPSS group, 60.87% (70/115) of patients had severe symptom score, 32.17% (37/115) with moderate severity and 6.96% (8/115) with mild symptom score. In the same set of patients, after applying PDSS, 34.78% (40/115) belonged to the severe disease severity score category, 54.78% (63/115) in moderate and 10.44% (12/115) in mild severity category.
The IPSS being subjective symptom score, higher the score of daytime frequency and nocturia, more was the total score which placed the patients in severe symptom category. However, in PDSS, due to objective parameters, only those patients with obstructive voiding got higher score. Of 115 patients, 84 (73.04%) needed surgical intervention; as per IPSS, 50% (4/8) in mild severity, 59.45% (22/37) in moderate and 81.69% (58/70) in severe symptom category required surgical intervention (monopolar transurethral resection of prostate (TURP)); as per PDSS, 08% (1/12) in mild, 73.02% (46/63) in moderate and 92.5% (37/40) with the severe disease severity score needed surgical intervention. Table 3 compares the assessment of severity grading by IPSS and PDSS.
Severity grading and requirement of surgery as assessed by IPSS and PDSS.
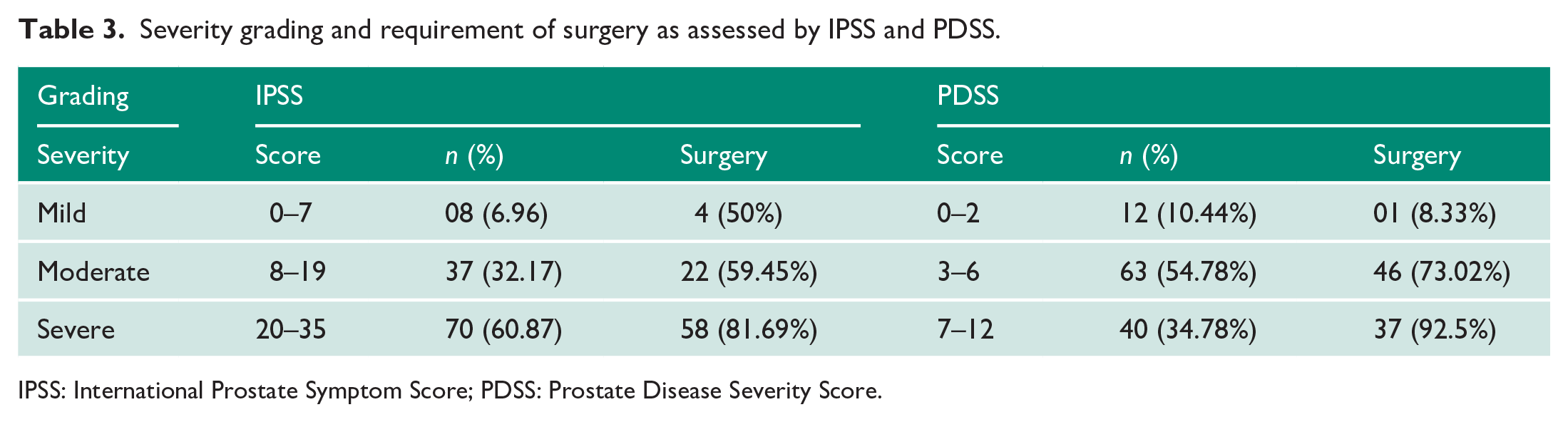
IPSS: International Prostate Symptom Score; PDSS: Prostate Disease Severity Score.
In patients who underwent TURP, success was measured by reduction in IPSS, improvement in Qmax component of PDSS, pre- and post-operatively and the mean difference was statistically significant (p = 0.000) (Table 4).
Comparison of the pre-operative and post-operative IPSS and Qmax..
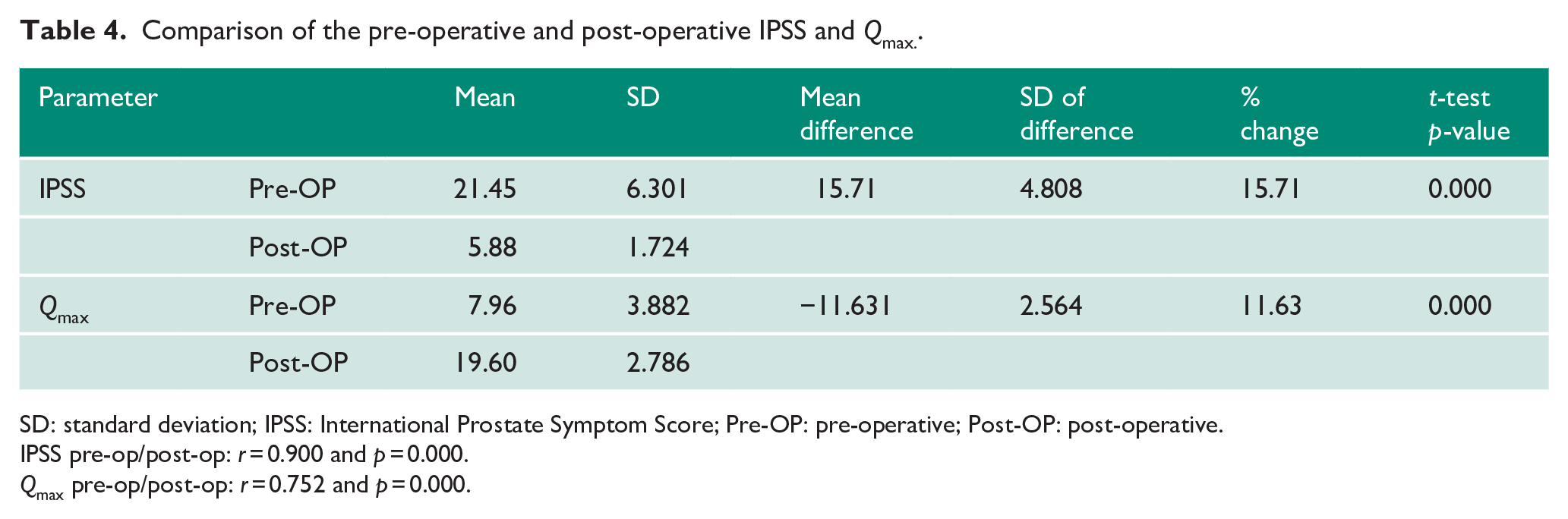
SD: standard deviation; IPSS: International Prostate Symptom Score; Pre-OP: pre-operative; Post-OP: post-operative.
IPSS pre-op/post-op: r = 0.900 and p = 0.000.
Qmax pre-op/post-op: r = 0.752 and p = 0.000.
Correlation (Pearson’s correlation, r) of PDSS with IPP (r = 0.712, p = 0.000) and IPSS (r = 0.230, p = 0.013) was statistically significant. Figure 1 shows the correlation between PDSS and IPSS. Negative correlation was noted between PDSS and Qmax. Of the four variables, Qmax is the most important determinant in the new PDSS (Table 5).
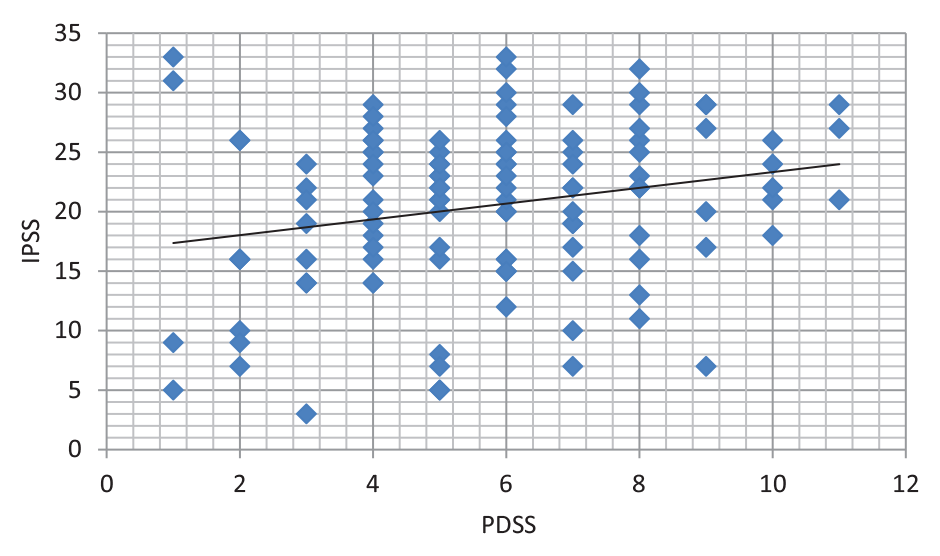
Correlation between PDSS and IPSS.
Correlation of PDSS and Qmax with various parameters.
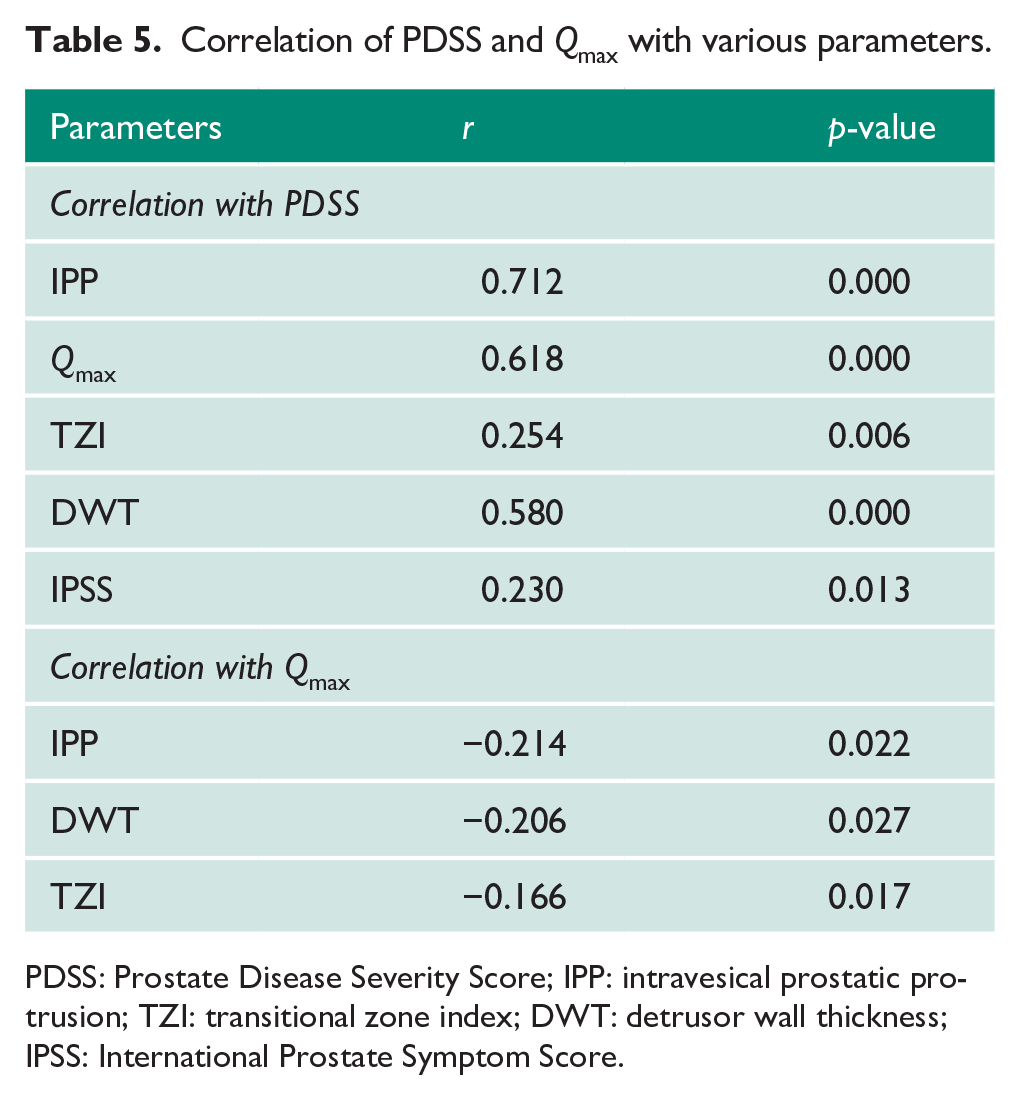
PDSS: Prostate Disease Severity Score; IPP: intravesical prostatic protrusion; TZI: transitional zone index; DWT: detrusor wall thickness; IPSS: International Prostate Symptom Score.
IPSS was completed without assistance by only 16.52% (19/115) patients. All these patients had education of ⩾10th grade. Remaining 83.48% (96/115) needed assistance either from the clinical assistant or attendees to complete the questionnaire.
Discussion
Of the various symptom scores available for BEP, IPSS, American Urological Association (AUA) Indices are used routinely in clinical practice. Scoring systems including IPSS, AUA indices use questionnaires which are often reported to be difficult to complete by patients without assistance. 9 Urodynamic studies and uroflowmetry give concrete evidence of the degree of severity of underlying pathology. Uroflowmetry is recommended by the AUA only as a specialist investigation and not for routine use; European Association of Urology (EAU) recommends its use before invasive treatment for BEP. However, none singly do aid in judging the requirement of surgery or predict the success of treatment in these patients, are not recommended alone in deciding the severity and the need for surgical intervention. 10
There were a few scoring systems developed to predict obstructive voiding and BOO but with limitations. Of the non-invasive scoring systems currently followed to predict obstruction include the clinical prostate score (CLIPS), 11 the BOO number (BOON), Modified BOON 12 and a clinical prostate score. 13
CLIPS 11 had a superior correlation with BOO with urodynamical objective than with isolated parameters. Other scores combined a few parameters with the existing indices; Schacterle et al. 5 combined the maximal urinary flow rate and the AUA symptom index; Steele et al. 14 combined the symptom score, maximal free flow rate and PV for predicting BOO. Ockrim et al. 15 developed a BOO index based on the maximal free flow rate and PV. Kuo 13 established a clinical prostate score by summing the scores of seven prostate and uroflowmetry items. The BOON is calculated using a formula composed of parameters: PV, maximal urinary flow rate and mean voided volume estimated from frequency-volume charts.
CLIPS consider total prostate volume (TPV) which may not provide the actual clinical stage as demonstrated by Hirayama et al. 16 that significant obstruction can be seen even in persons with 20 mL of PV. Hence, TPV can lead to a fallacious interpretation. BOON, in addition to the limitation of using TPV, has complexity of calculating relative PVR. 17 Scoring system developed by Schacterle et al. 5 requires AUA symptom index (AUA-SI). Filling up of the AUA-SI warrants good memory, certain level of education and understanding for interpretation. Studies have shown AUA-SI/IPSS could be misinterpreted by patients with lower grade of education.1,2 Steele et al.’s 14 scoring has the limitation of using IPSS and total PV. Scoring system developed by Ockrim et al. 15 has the limitation of using TPV. Clinical prostate score by Kuo 13 uses PV with voided volume, which can be less because of low-capacity bladder or due to significant PVR. Modified BOON 12 has the complexity of formula.
Bother score introduced in 2005 18 although correlated well with IPSS19–21 too considers subjective evaluation. It is a simple, patient-oriented tool, considers patient’s perception of symptoms, 22 (which being subjective, cannot be totally relied upon) and correlated with clinical grading. Barqawi et al. 23 proposed a modified AUA symptom score. UWIN (Urgency, Weak stream, Incomplete Void, Nocturia) Score recently developed for the Assessment of Lower Urinary Tract Symptoms (LUTS), although proposed to replace AUA-SI as correlated well with the latter, simple to use in patients with lower education levels, high patient preference, but it uses subjective parameters.24,25 Use of these subjective symptoms needs up-keeping of patient diary to document these parameters, which is not feasible in many patients.
Requirement of the PDSS
The complexities and the limitations of the current scoring systems to predict BOO prompted us to propose an alternate tool that is newer, simpler, and easy to use, which can predict severity of BOO and the need of surgical intervention based on the objective parameters. It takes into consideration Qmax, IPP, TZI and DWT. The PDSS is a simple calculation of addition of grade of all four variables to get a total score.
We have attempted to precise the IPSS using objective components in patients with obstructive voiding. Accordingly, objective assessment was made, and a new grading and scoring system was developed. The scoring system is proposed to differentiate obstructive voiders who may benefit from surgery as opposed to those with storage symptoms predominantly who would be better treated with medical therapy. This will also avoid unnecessary surgical intervention just because IPSS is high due to high score of storage components. We christened this new objective scoring system as ‘Prostate Disease Severity Score (PDSS)’.
Parameters used in PDSS have shown to correlate well with severity and in predicting the disease progression. Predictive value of TZI and IPP in assessing the severity and progression of BPH were reported to be reliable and favourable. 26 TZI of >0.5 has 90% sensitivity and is a significant predictor of BOO. 7 Significant correlation between IPP, PV and BOO is documented. 27 IPP is considered a better indicator than PV in predicting symptom severity and treatment outcome in patients on Tamsulosin for LUTS due to BPH. 28 IPP and bladder wall thickness are better predictors of BOO with an accuracy of 87% when used consecutively. 8 IPP as better predictor of BOO than PSA and PV. 29 Significant IPP is observed in severe BOO, impaired detrusor function and suggestive of possible benefit from surgery as in those presenting with acute urinary retention (AUR) with significant IPP. Besides, IPP is a predictor of success in Trial without Catheter in AUR. Failure rate of the voiding trial based on grades 1–3 IPP was 36%, 58% and 67%, respectively. 30 After weighing the limitations, we zeroed in on these (Qmax, IPP, TZI and DWT) objective parameters.
The PDSS has shown internal consistency in this study setup and was validated. A score of 0–2, 3–6 and >6 correlated well with mild, moderate and severe obstruction, respectively.
The PDSS can objectively differentiate pure obstructive voiders from others and is a better predictor for requirement of surgical intervention. In this study, 73.04% patients needed surgical intervention (TURP), due to failed medical therapy, symptom progression and poor urinary stream leading to a reduction in quality of life. These were the patients with moderate or high IPSS and with predominant obstructive voiding as suggested by PDSS.
An important point to note is in mild severity category, 50% needed surgical intervention in IPSS group on contrary to 8% in the PDSS group. There was a proportionate increase in the need in surgical intervention as severity score moved from mild (8%), moderate (73.02%) to severe degree (92.5%) in PDSS. However, same was not true in IPSS group, wherein patients with obstructive voiding also had low score as they did not have much daytime frequency and nocturia. On the contrary, even those with minimal obstructive voiding were placed in high severity group of IPSS due to predominant overactive bladder like symptoms and they did not need surgical intervention. Also, need of surgical intervention in IPSS group was not proportionate as per the severity grading. These data clearly show superiority of PDSS in differentiating patients with obstructive voiding who suit surgical intervention from those with overactive bladder type, who are best treated medically.
In this study, that IPP, DWT, TZI and Qmax proved to be strong determinants of obstructive voiding (p = 0.000). The PDSS objectively validated obstruction, as indicated by component parameters showed a statistically significant correlation with IPSS (r = 0.23 and p = 0.013). Patient’s perception of treatment outcome/success being subjective, success was objectively measured and correlated using pre- and post-operative IPSS and Qmax component of PDSS, which was statistically significant (Table 4).
The PDSS is a promising symptom severity score that uses reliable objective parameters in evaluating symptomatic BEP. It is the outcome of our effort to derive a simple tool to overcome the difficulties/limitations associated with completing IPSS proforma by minimising bias and also to objectively grade severity along with ability to predict need for surgical intervention. Being objective, it will help in avoiding over-treatment and under-treatment. In addition, it will guide in administering tailored, individualised, customised treatment. We noted that PDSS is devoid of subject bias and interpretation error of IPSS. The PDSS is primarily designed to help in making management decision in those who are unable to complete IPSS and predict the need for surgical management. It can also be used in those who can complete IPSS because, unlike IPSS, PDSS is purely an objective score and a better indicator of disease severity. Although PDSS can predict the requirement of surgical intervention, particularly in those with severe obstruction, further studies are needed to for external validation of this novel objective scoring system.
Conclusion
The objective nature of the PDSS, comparable correlation with the IPSS, ability to predict the need for surgical intervention in patients with BEP and ease of application makes the PDSS a potential user-friendly system in the management of patients with BEP. It will help in avoiding over-treatment, under-treatment, administering tailored and individualised treatment option. It overcomes the subject bias and errors in interpretation of the IPSS.
Footnotes
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical approval
The ethical approval for this study was obtained from the Institutional Ethics Committee.
Consent to participate
Prospective patients were screened after obtaining written informed consent.
Guarantor
Dr K.N.S.
Contributorship
All authors contributed towards the conception of the idea, preparation of protocol, conduct of study, data collection, analysis and manuscript preparation. All authors have reviewed the manuscript. K.N.S. contributed to concept, conduct and patient management including surgical management, interpretation of analysis, manuscript preparation and guarantor. S.P. contributed to clinical evaluation, patient management including surgical management, data collection, interpretation of analysis and review of manuscript. G.G.L.P. contributed to idea and conceptualisation, study supervision, clinical evaluation, patient management including surgical management, review of manuscript and approval of the final manuscript. R.S. contributed to patient management including surgical management and review of manuscript. P.V. contributed to overall guidance, study supervision and subject expert in patient management.