
Abstract
Objectives:
Holmium laser enucleation of the prostate (HoLEP) can be used regardless of prostate size and offers durable long-term results for patients suffering from lower urinary tract symptoms (LUTS)/benign prostatic obstruction (BPO), with reduced perioperative morbidity. In most western societies almost half of the population are overweight, and obesity itself is often a risk factor for surgical treatment of patients. We therefore analysed the impact of body mass index (BMI) on outcomes and perioperative morbidity in patients undergoing HoLEP for LUTS at our tertiary referral centre.
Methods:
We retrospectively collected data for 877 patients who underwent HoLEP for LUTS/BPO between 2014 and 2018 and divided patients into group 1 (BMI<25), 2 (BMI 25<30), and 3 (BMI⩾30). We analysed perioperative parameters, safety, and short-term functional outcomes.
Results:
In preoperative patient characteristics we observed a similar LUTS profile throughout our patient cohorts. The highest proportion of ASA score ⩾III was observed in the obese patient cohort. Enucleation time was significantly prolonged in morbidly obese patients and operative speed was significantly slower, without difference in perioperative complications. Functional outcomes were assessed 30 days post-surgery with significant improvement in IPSS, quality of life (QoL) and Qmax for all groups.
Conclusion:
Although operating on overweight and obese patients takes significantly longer, HoLEP is efficient and offers acceptable perioperative complication rates even in morbidly obese patients (BMI⩾30).
Level of evidence:
Not applicable.
Keywords
Introduction
Transurethral resection of the prostate (TURP) and open transvesical prostatectomy (OP) are established surgical methods for treatment of prostate enlargement. Current guidelines on management of non-neurogenic male lower urinary tract symptoms (LUTS) describe TURP as the surgical standard of care for prostates 30-80 ml, and recommend OP or laser enucleation of the prostate for prostates >80 ml. 1 While TURP remains the surgical reference method for medication refractory LUTS secondary to benign prostatic obstruction (BPO), the introduction of holmium laser enucleation of the prostate (HoLEP) added a new and size-independent method of endourological prostate enucleation, and has since become one of the most scrutinized forms of surgical intervention for BPO. 2 HoLEP has been compared with TURP multiple times and accepted as at least equal in efficacy and even superior regarding perioperative morbidity.3,4 HoLEP is fast, efficient and independent of prostate size, and its effectiveness in relief of LUTS is comparable with OP.5-7 Benefits associated with HoLEP, such as less blood loss, shorter catheterization time and hospital stay, seem durable in long-term follow-up. Thus, it has even been considered the “new gold standard” for surgical intervention in LUTS secondary to BPO. 8
Obesity certainly is a risk factor for patients’ health, and it has risen at an alarming speed over the past few years. 9 While only two decades ago, one in six adults in the USA had been considered obese, that number has doubled now. 10 As for Germany, the GEDA 2014/2015-EHIS study showed 54.0% of the German adult population being overweight or obese, according to the definition of the World Health Organization (WHO).9,11 When offering surgical treatment to patients, the risk of developing complications is related to patients’ health status. Among the main goals when treating an overweight and obese population are reducing perioperative morbidity and mortality when offering a safe and functionally efficient endourological treatment. With many different endourological methods to choose from, selecting the optimum treatment option in a highly comorbid patient cohort becomes mandatory.
Therefore, we aimed to analyse the impact of obesity on perioperative morbidity and mortality and evaluate the efficacy of HoLEP in obese patients undergoing minimally-invasive surgery for LUTS/BPO.
Materials and methods
Patient population and study design
We included 877 patients who underwent HoLEP for LUTS/BPO between 2014 and 2018 at our tertiary referral centre and created a computerized database containing clinical and pathological information, perioperative data and follow-up information solely for this study. Patients were included according to the aforementioned criteria and retrospectively analysed. HoLEP for LUTS/BPO was indicated in accordance with the current European Association of Urology (EAU) guidelines on management of non-neurogenic male LUTS. 1
All HoLEPs were performed by two experienced surgeons only, using a VersaPulse® 100W Holmium Laser (Lumenis Ltd., Yokneam, Israel) with a frequency of 53 Hz at a power setting of 1.2 kJ. For morcellation a mechanical tissue morcellator (R. Wolf, Piranha, Knittlingen, Germany) was used. According to our standard protocol, surgery was followed by 12 hours of continuous bladder irrigation with normal saline via a 24 F three-way Foley catheter.
According to the WHO definition of obesity, patients were stratified into three groups. Adults with a BMI of less than 18.5 kg/m2 are considered to be underweight and were included in group 1, with n=6. A BMI between 18.5 kg/m2 and 25 kg/m2 is defined as normal weight (group 1; n=293), a BMI between 25 kg/m2 and 30 kg/m2 as overweight (group 2; n=360) and a BMI of ⩾30 kg/m2 as obese (group 3; n=224). 9
Besides clinical and pathological information, perioperative data was used to describe the cohorts. Additionally, perioperative complications were assessed and defined as any adverse event within 30 days of surgery. Complications were classified using the modified Clavien-Dindo scale for reporting complications in transurethral resection of the prostate. 12
Statistical analysis
Statistical analysis was performed using SPSS V26.0 software (IBM SPSS Statistics, Version 26.0. Armonk, NY). Results are given as a median and interquartile range (IQR) for continuous variables and as a percentage for categorial variables. Univariate analyses were performed using Fisher’s exact test and χ2 test for categorial variables, and a t test and Mann-Whitney U test for continuous variables. For analyses in which three groups were compared, we used univariate analysis of variation (ANOVA). All reported p-values were two-sided and considered statistically significant if p<0.05.
Results
Patient characteristics
Patients’ demographic parameters are displayed in Table 1. In total we included 877 patients, who underwent HoLEP for LUTS/BPO. Preoperative LUTS profiles and patient characteristics were largely comparable between predefined groups (Table 1). As expected, median BMI was significantly different between all three groups with 23.5 (IQR 22.5-24.4), 27 (IQR 25.9-27.9) and 31.6 (IQR 30.5-33.8) for groups 1, 2 and 3, respectively (p<0.001). We observed a statistical difference in preoperative haemoglobin levels between groups, with a median of 14.5 g/dl (IQR 13.7-15.3), 14.9 g/dl (IQR 14.0-15.7) and 15.0 g/dl (IQR 14.1-15.8) for groups 1, 2 and 3, respectively (p<0.01 for group 3 vs group 1 and p<0.03 for group 2 vs group 1). The American Society of Anaesthesiologists (ASA) score ⩾III was assessed in patients before surgery and was significantly more prevalent in the obese (group 3) compared with the other patient groups, with 44.1 % in group 3 and 29.9 % and 32.1 % for groups 2 and 1, respectively (p<0.03). However, we found no statistically significant difference in age, prostate volume (PV) or preoperative functional parameters, i.e. international prostate symptom score (IPSS), quality of life (QoL), maximum flow rate (Qmax), post void residual (PVR), total prostate-specific-antigen (PSA), or the rate of an indwelling urinary catheter (IDC) between all groups prior to HoLEP.
Demographic parameters.
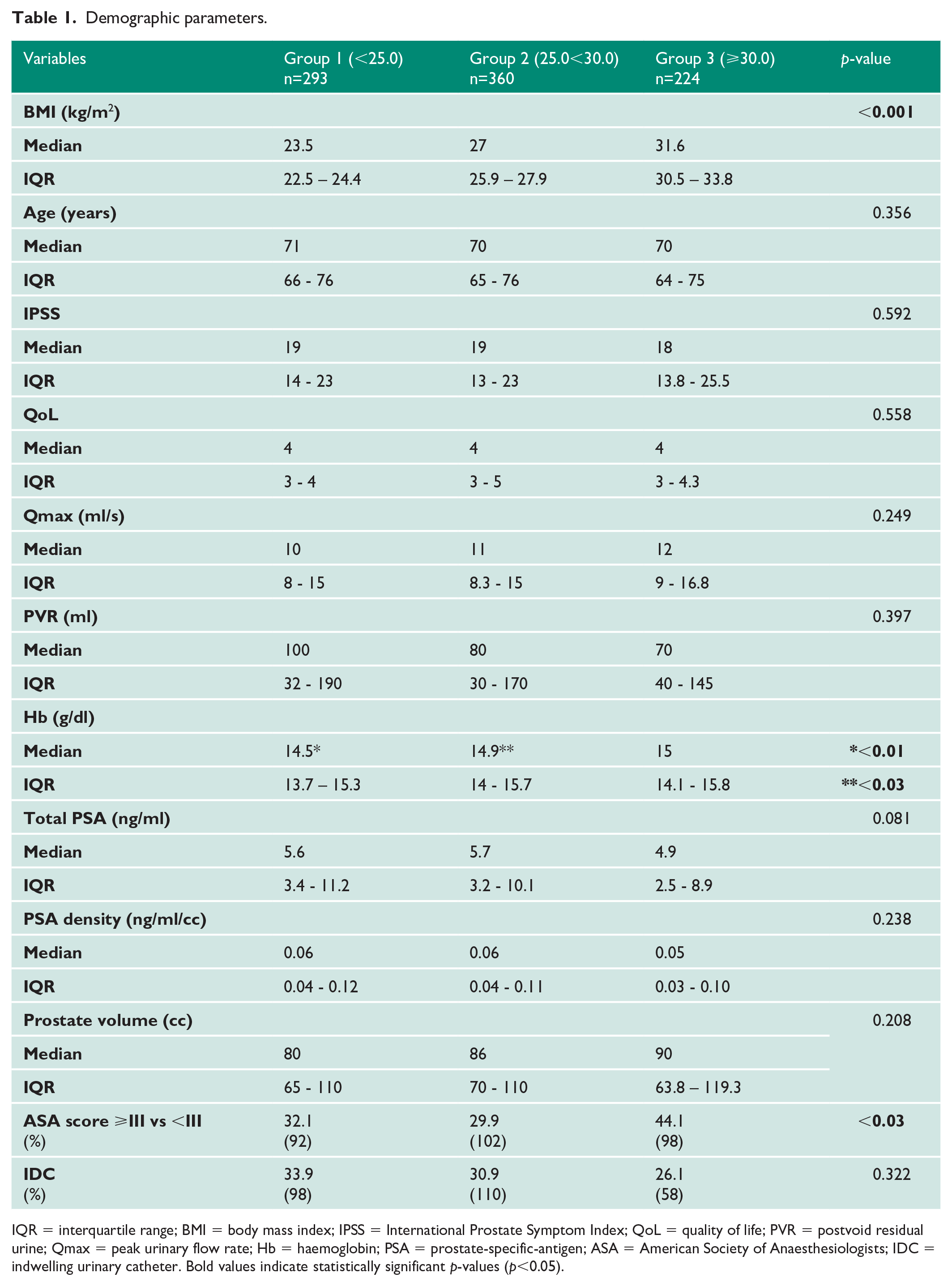
IQR = interquartile range; BMI = body mass index; IPSS = International Prostate Symptom Index; QoL = quality of life; PVR = postvoid residual urine; Qmax = peak urinary flow rate; Hb = haemoglobin; PSA = prostate-specific-antigen; ASA = American Society of Anaesthesiologists; IDC = indwelling urinary catheter. Bold values indicate statistically significant p-values (p<0.05).
Perioperative assessment and functional outcomes
In table 2, analysis of perioperative outcomes showed a statistically significant difference in surgery time with a median enucleation time of 43 minutes (IQR 30.8-60) for the obese in group 3 versus the non-obese patients in group 1 with a median of 31 minutes (IQR 26-42.3; p<0.01). However, there was no statistical difference compared with the overweight patient cohort in group 2 with 35 minutes (IQR 28.3-51.5; p=0.301). Furthermore, we observed a significantly slower operative speed with 1.54 g/min (IQR 0.95-2.23) in the obese versus 1.75 g/min (IQR 1.33-2.63) in group 1 (p<0.02) and 1.60 g/min (IQR 1.03-2.38) in the overweight population (p=0.08). However, groups 1, 2 and 3 showed no statistically significant difference in total resected tissue or tissue retrieval percentage. We could not detect any difference between groups in overall median haemoglobin drop (p=0.504), catheterization time (p=0.588) or hospitalization time (p=0.438).
LUTS were assessed four weeks after surgical treatment during follow-up visits and improved significantly in all three patient cohorts. Median IPSS decreased by 14 points for each group (p=0.596). We observed significant improvement in QoL, albeit without significant difference between all groups (p=0.678). Early functional outcomes four weeks after surgery showed no significant difference between all groups with an increase of median Qmax of 15.0 ml/s (IQR 10.0-23.0), 14.0 ml/s (IQR 8.0-24.0) and 15.5 ml/s (IQR 8.0-20.0) for groups 1, 2 and 3, respectively (p=0.438). A median PVR reduction of 74 ml (IQR 7.5-165.5), 70.0 (20.0-161.0) and 50 (28.8-122.3) was observed for groups 1, 2 and 3, respectively (p=0.515). There was no difference between the three groups in catheterization time or duration of hospital stay (p=0.588 and p=0.438 for both items, respectively).
Perioperative complications
In total, 57 (57/877, 6.1 %) patients from the entire cohort experienced at least one perioperative complication. In group 1, 2 and 3 respectively, 18 (6.1 %), 19 (5.3 %) and 20 (8.9 %) patients had at least one perioperative complication. There was no significant difference in the number of complications between groups (p = 0.646). The groups also did not differ in the severity of their respective perioperative complications (p=0.679). Complications and subsequent clinical management are listed in detail in Table 3. Either of the grade IV complications was evenly distributed between groups 2 and 3, respectively. There was no grade V complication.
Discussion
Many studies show that obesity increases the risk of benign prostatic hyperplasia (BPH).13-15 Giovannucci et al. could show that, of almost 26,000 male participants, those with an obese waist circumference (>109cm) were 38% (OR:1.38, 95% CI:1.01-1.95) more likely to undergo surgery for LUTS secondary to BPO than those with a non-obese waist circumference (<89cm). 13 Zucchetto et al. found that men with a lowest lifelong BMI of ⩾23.7 kg/m2 were 56% more likely to have histological BPH than men with a lowest lifelong BMI of 20.7 kg/m2 or less. 16
As a demographic shift in western societies will lead to an ever-ageing population, benign prostatic diseases such as LUTS/BPO will become more prevalent in patients presenting with obesity posing as an important risk factor when undergoing surgery for LUTS/BPO.1,11
Although many centres have shown that HoLEP for LUTS/BPO is feasible, the influence of obesity on functional outcomes and perioperative morbidity and mortality is of great importance and may even add to the economic impact of obesity on society. HoLEP is the only endourologic procedure for patients with LUTS secondary to BPO whose functional results rival those of open prostatectomy (OP).5,17 Due to increased retropubic and periprostatic fat, obesity already presents a risk factor for perioperative complications in OP and many studies deal with endoscopic alternatives to open surgery in obese patients.18,19 Furthermore, increased abdominal fat can lead to severely altered anatomic conditions in the lower urinary tract and obese patients are already at increased risk of multiple comorbidities, posing a challenging decision even when offering minimally-invasive techniques functionally equivalent to open surgery.19,20
In our study population, HoLEP offered high functional efficacy combined with low perioperative morbidity, regardless of BMI, thus corroborating the favourable risk profile of HoLEP when compared with OP or TURP.5,8 Various studies have demonstrated that obesity in general prolongs operative time and, with that, increases perioperative morbidity and mortality in an already higher risk patient cohort. 21 Obesity is often associated with poor health and in itself is a risk factor for many diseases.11,21 Overall, our patient cohorts were highly comparable, and the median PV or preoperative LUTS profiles did not differ between our patient cohorts, as reported previously in the obese. 22 As anticipated, our patient cohorts significantly differed in ASA score ⩾III with more obese patients in that category. However, the ASA scoring system identifies BMI itself as a risk factor, and thus, includes BMI in its scoring system to determine the risk of medical complications and mortality following surgery. 23 This may explain the higher relative number of obese patients presenting with ASA score ⩾III, irrespective of comorbidities. The overweight and obese patient cohort showed a higher preoperative haemoglobin value, corresponding to the data reported by Akter et al. 24 However, there was no need for perioperative blood transfusion. Also, the median postoperative drop in haemoglobin value was clinically irrelevant and showed no statistically significant difference between all patient cohorts.
As reported by various studies before, we found that obesity correlates with increased operative time. 21 Operative time was assessed as enucleation time and operative speed defined as grams of enucleated tissue per minute. We observed a significantly longer median enucleation time in the obese patient cohort and a significantly slower operating speed than in normal weight patients. However, we report no statistically significant difference in total resected tissue or tissue retrieval percentage. Parsons et al. have shown that obesity is often associated with severity of LUTS. 25 However, prolonged enucleation time, in the absence of higher PVs, may be due to increased retropubic and periprostatic fat, which may alter the anatomy of the lower urinary tract in male patients presenting with obstructive LUTS and pose a more challenging surgical approach. 20 Not only does an increased operative time pose a significant risk of perioperative morbidity and mortality, but it also adds to the significant economic burden of obesity with accumulating operative time and decreasing patient turnover. 26
Gacci et al. reported a correlation between obesity, metabolic syndrome and reduced urinary symptom recovery after prostatic surgery. In patients presenting with a waist circumference of >102 cm, they even reported incomplete recovery of total IPSS and storage of IPSS after OP and TURP.27,28 However, we could not detect any significant difference in recovery of functional urodynamic parameters after HoLEP. We report a constant and strong increase of Qmax, and overall reduction of IPSS and improvement of QoL for each patient group (Table 2). Contrary to the data gathered by Sener et al., we could show that HoLEP is feasible and may be even more effective in overweight and obese patients compared to TURP. 29 Postoperative functional outcomes were assessed 30 days post-surgery, as there is no significant difference in short-term (30 days) postoperative functional outcomes versus long-term follow-up after one year. 30
Perioperative and clinical outcomes four weeks after surgery.
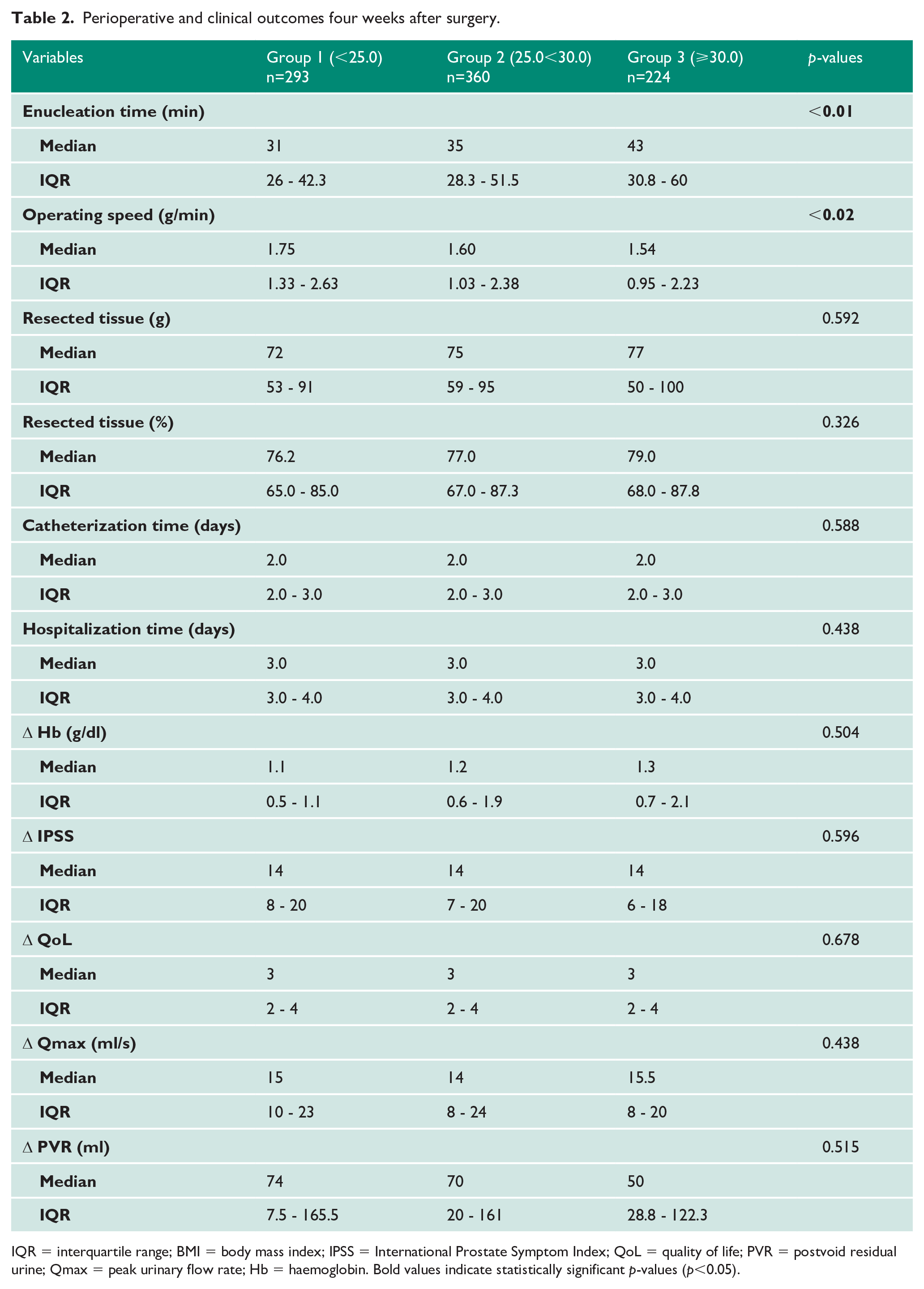
IQR = interquartile range; BMI = body mass index; IPSS = International Prostate Symptom Index; QoL = quality of life; PVR = postvoid residual urine; Qmax = peak urinary flow rate; Hb = haemoglobin. Bold values indicate statistically significant p-values (p<0.05).
Perioperative adverse events according to the Clavien-Dindo classification.
The following adverse events (AEs) were identified as perioperative complications and are listed with their respective clinical management. Bold values indicate statistically significant p-values (p<0.05).
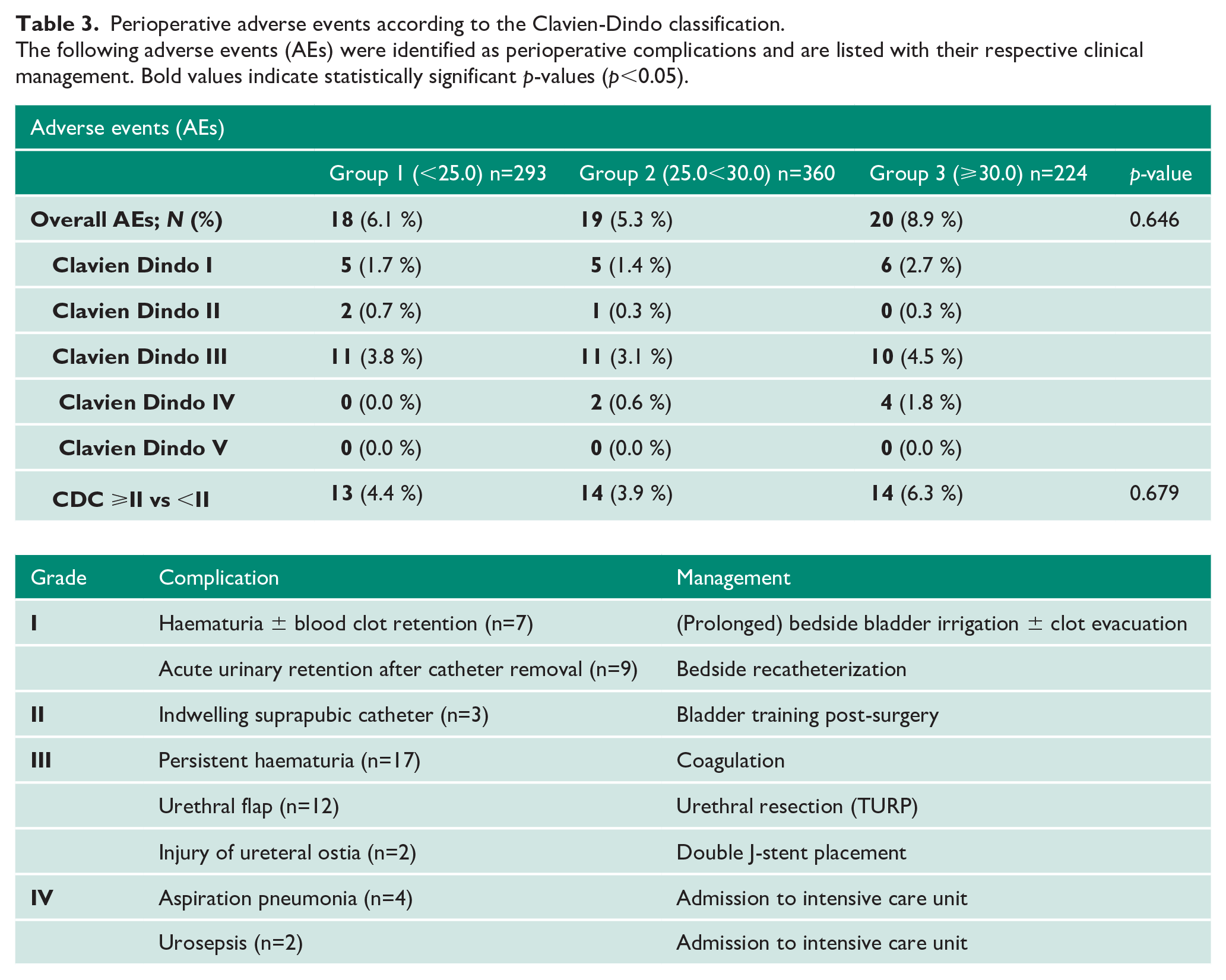
For reporting perioperative complications following transurethral resection of the prostate, the Clavien-Dindo classification (CDC) has been modified by Mamoulakis et al. 12 In total, we observed an overall complication rate of 6.1% (57/877 patients). When compared with the data recorded by Mamoulakis et al., with an overall CDC rate of 15.7%, our population had few perioperative complications. 12 Only 0.7% (6/877 patients) of all complications were CDC grade IV, corresponding well with the complication rate of 0.7% for CDC grade IV reported by Elshal et al. 30 There were no grade V complications and no life-threatening transurethral resection (TUR-) syndrome in our patient cohort.
Based on our data, and corroborating the results of Carmignani et al. on safety and feasibility of thulium laser enucleation of the prostate (ThuLEP), we could show that HoLEP is an effective and safe treatment option in LUTS/BPO in overweight and obese patients and is even superior to TURP.7,29
To the best of our knowledge, this is the first study analysing the clinical value and impact of obesity on feasibility and postoperative functional outcomes of HoLEP in overweight and obese patients in such a large patient cohort (n=877). Obesity defined solely by BMI most certainly poses a limitation of this study. Even though BMI is an accepted measurement of obesity, muscle mass, age, gender and ethnicity may be confounders and other scores may help to assess obesity more accurately.31,32 Nevertheless, BMI is easy to determine and, therefore, a valuable research tool. As ASA includes BMI in its scoring system, the higher relative number of obese patients presenting with ASA score ⩾III may be due to BMI or comorbidities. However, there is a severe lack of information regarding perioperative morbidity and mortality, as well as postoperative outcomes in obese patients treated with endoscopic enucleation or resection of the prostate, and the retrospective study design is a limitation to our study. We did not include patients undergoing other laser treatment options or TURP for LUTS/BPO in our study. We report a longer median operative time in the overweight and obese patient cohort. Even though we think it is feasible that altered anatomy may have led to a prolonged operative time, we cannot be sure of it. However, this study was designed to evaluate feasibility of HoLEP in obese patients, and we are confident in reporting our data. There also was a smaller proportion of patients in the BMI ⩾30 kg/m2 group than in the other groups, which naturally limits the power of our analysis. Being a tertiary referral centre brings with it the problem of following up the patient at home, preventing the complete collection of long-term data for more cases. When accepting a slightly longer operative time and enucleation time, there are no limitations to using HoLEP in an overweight or obese patient cohort with exceptionally low morbidity and sufficient postoperative efficacy. Offering HoLEP as a treatment option for medication refractory LUTS/BPO in overweight and obese patients is safe and feasible with great functional results.
Conclusion
The increasing number of obese patients poses a worldwide health issue of socio-economic relevance. Taking this into consideration, we sought to evaluate the impact of obesity on perioperative morbidity and mortality as well as functional outcomes in patients undergoing HoLEP for LUTS/BPO. In conclusion, HoLEP provides a favourable safety profile, even in the morbidly obese patient cohort (BMI⩾30kg/m2). Therefore, HoLEP for LUTS/BPO can be offered as a viable treatment option to overweight and obese patients.
Footnotes
Conflicting interests
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of ethics and informed consent:
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study formal consent is not required. All data was collected and analyzed anonymously.
Guarantor
A. Tamalunas
Author’s contribution
A. Tamalunas: Project development, Data collection and analysis, Manuscript writing
T. Westhofen: Data collection and management, Data analysis
M. Schott: Data collection and management, Data analysis
P. Keller: Data collection and management, Data analysis
M. Atzler: Data collection and management
CG. Stief: Project development
G. Magistro: Project development, Data collection and analysis, Manuscript writing