
Abstract
Introduction:
This study aimed to describe single-stage urethroplasty and to determine factors associated with urethrocutaneous fistula after the procedure at our institution.
Methods:
All hypospadias patients without any prior surgery who underwent single-stage urethroplasty from July 2010 to January 2018 were included. In total, 179 patients were followed for at least one year postoperatively. Information on types of hypospadias, operation techniques, chordee degree, preoperative pyuria (urine white blood cell count >5/HPF), urethral defect length and urethrocutaneous fistula formation was collected.
Results:
We obtained 103 cases of posterior (57.5%), middle (57 cases) and anterior (19 cases) hypospadias on whom onlay preputial island flap (71 cases), tubularized incised plate (46 cases) and Duckett’s transverse preputial island flap (35 cases) were conducted. After 47.1±25.8 months of follow-up, urethrocutaneous fistula were found in 23 (12.8%) patients associated with posterior hypospadias occurrence (p=0.025), longer urethral defect (p=0.007) and preoperative pyuria (p<0.001). Chordee degree (p=0.886) and age (p=0.187) were not significant factors associated with urethrocutaneous fistula formation.
Conclusion:
Single-stage urethroplasty is a versatile procedure for various hypospadias cases, with a urethrocutaneous fistula rate of 12.8%. Posterior hypospadias, preoperative pyuria and longer urethral defect were associated with urethrocutaneous fistula formation.
Level of evidence
Level 2B.
Keywords
Introduction
Hypospadias is the most common congenital external genital malformation in males, affecting 1/300 live male births globally, with various incidence rates in different countries. 1 Hypospadias is characterized by excess dorsal preputial tissue, ventral tissue hypoplasia, ventral urethral opening and penile curvature. Only 10% of cases occurred posteriorly (the scrotum and perineum), while distal and coronal/sub-coronal hypospadias type were more common. 2 Current recommendations suggest surgical repair to achieve an aesthetically straight penis for penetration, with meatal relocation for a straight urinary stream. 2
Single-stage urethroplasty can be used for anterior to posterior hypospadias. Developed from a simple technique for epispadia by Karl Thiersch in the 19th century, Anger and Duplay used tubularization for hypospadias repair, utilizing urethral plate and ventral penile skin to form the urethral tube. 3 Duckett popularized the one-stage transverse tubularized preputial island flap technique intended for severe chordee hypospadias with a long urethral defect (up to 2–6 cm). 4 Elder et al. described the onlay preputial island flap to overcome the flaws of the Mathieu perimeatal-based flap, demonstrating the use of the transverse preputial island flap as augmentation for the native urethral plate for anterior or middle hypospadias with minimal chordee. 5 In 1994, Snodgrass introduced tubularized incised plate (TIP) urethroplasty technique for anterior hypospadias with minimal chordee. 6 For severe hypospadias, Koyanagi et al. pioneered the use of the meatal-based ‘manta-wing’ and parameatal-based flap with circumferential foreskin flap urethroplasty in a single-stage fashion. 7
Urethrocutaneous fistula is the most common complication of urethroplasty, followed by meatal stenosis, urethral stricture or diverticulum, glans dehiscence and poor cosmetic profile requiring redo surgery.2,8 Fistula rates in single-stage urethroplasty vary from 17% to 20% for TIP and the onlay technique; up to 20–50% in the Koyanagi procedure. 9 Known factors for the occurrence of postoperative fistula include infection, poor surgical techniques, urethral stricture or meatal stenosis. 8 This study aimed to describe our current experience with single-stage urethroplasty and to determine several preoperative factors associated with urethrocutaneous fistula.
Methods
Patients
This study was approved by the Ethics Committee of Cipto Mangunkusumo Hospital – Faculty of Medicine, University of Indonesia (no. KET-1002/UN2.F1/ETIK/PPM.00.02/2019). We included all hypospadias patients without any prior urethroplasty history who underwent single-stage urethroplasty conducted in Cipto Mangunkusumo General Hospital, the national referral hospital in Indonesia, between July 2010 and January 2018, and followed for at least one year postoperatively. Demographic data, information on the type of hypospadias, preoperative urine leucocyte count, operation technique, chordee degree, urethral length defect and urethrocutaneous fistula occurrence were collected. Signs of systemic and localized infection after surgery were also recorded.
The type of hypospadias was classified based on preoperative urethral orifice location using the classification once described by Duckett in 1996. Three classifications were used: anterior (glanular, subcoronal and distal shaft), middle (mid-shaft and proximal shaft) and posterior (penoscrotal, scrotal and perineal). Penile chordee or ventral curvature were assessed preoperatively and classified as mild (<30º), moderate (30–45º) or severe (>45º). After chordee excision and penile curvature correction, urethral defect length was measured. Urinalysis was routinely performed preoperatively at our institution to determine the need for early empiric antibiotic therapy. Preoperative leucocyturia (urine leucocyte >5/HPF) were given broad-spectrum antibiotics (cefotaxime or cefoperazone, therapeutic dose adjusted) 24 hours prior to surgery. Note that patients with symptomatic leucocyturia suggestive of a symptomatic urinary tract infection (UTI) were not candidates for surgery and warranted preoperative therapy until resolved. Unaffected patients were administered prophylaxis antibiotics one hour before the incision. A therapeutic dose of intravenous antibiotics was given during hospitalization, usually until stent removal.
Urethroplasty technique
The urethroplasty technique used varied according to surgeon preference based on preoperative assessment and intraoperative findings, the latter being the paramount factor. Three independent paediatric urologists perform surgery at our institution. After chordee excision, penile curvature was assessed to determine the need for further intervention. Penile curvature of more than 30–40º after chordee excision warrants dorsal shortening (Baskin’s or Nesbit’s dorsal plication) with preserved urethral plate techniques (TIP, Thiersch–Duplay, Mathieu and others.) or even ventral lengthening with transected urethral plate techniques (Duckett and Koyanagi). Most urethral tabularizations were done using 6.0 Polydioxanone (PDS®) and short 6 Fr silastic stents (5–6 cm, depending on the case) as the entubularization guide. The silastic stent was fixed to the glans using 3.0 Prolene®. For older cases, 5.0 Polydioxanone (PDS®) and a 10–12 Fr silicone Foley catheter were used. A second layer, usually from the dartos fascia, was always implemented after tubularization. Urinary diversion using cystostomy (Cystofix®) was used for all urethroplasty techniques involving neo-urethra tubularization (Duckett, onlay island flap, TIP and others). Postoperatively, the wound was treated using an antibiotic dressing, fixed using Elastomull® for five to seven days and treated with chloramphenicol ointment. The silastic stent or silicone catheter was removed after five to seven days, while the cystostomy was kept in place for 14 days.
Data collection
Data were collected through medical records, phone survey and messaging system survey. Urethrocutaneous fistula was chosen as the main outcome, since it is more readily recognizable by both patients and doctors and did not require an additional examination.
Statistical analysis
Data were analysed using IBM SPSS Statistics for Windows v20.0 (IBM Corp., Armonk, NY). All categorical data were analysed using the chi-square test, while numerical data were analysed using an unpaired t-test and Mann–Whitney U-test, and a p-value of <0.05 was considered statistically significant.
Results
A total of 179 patients were included in this study, with a mean follow-up time of 47.1±25.8 months. Posterior hypospadias was the most common type encountered, predominantly penoscrotal cases (45.3%) with severe chordee (45.8%). Preoperative leucocyturia (urine leucocyte >5/HPF) was found in 14 (7.8%) cases. Demographic and characteristic data are shown in Table 1.
Patient demographics and characteristics.
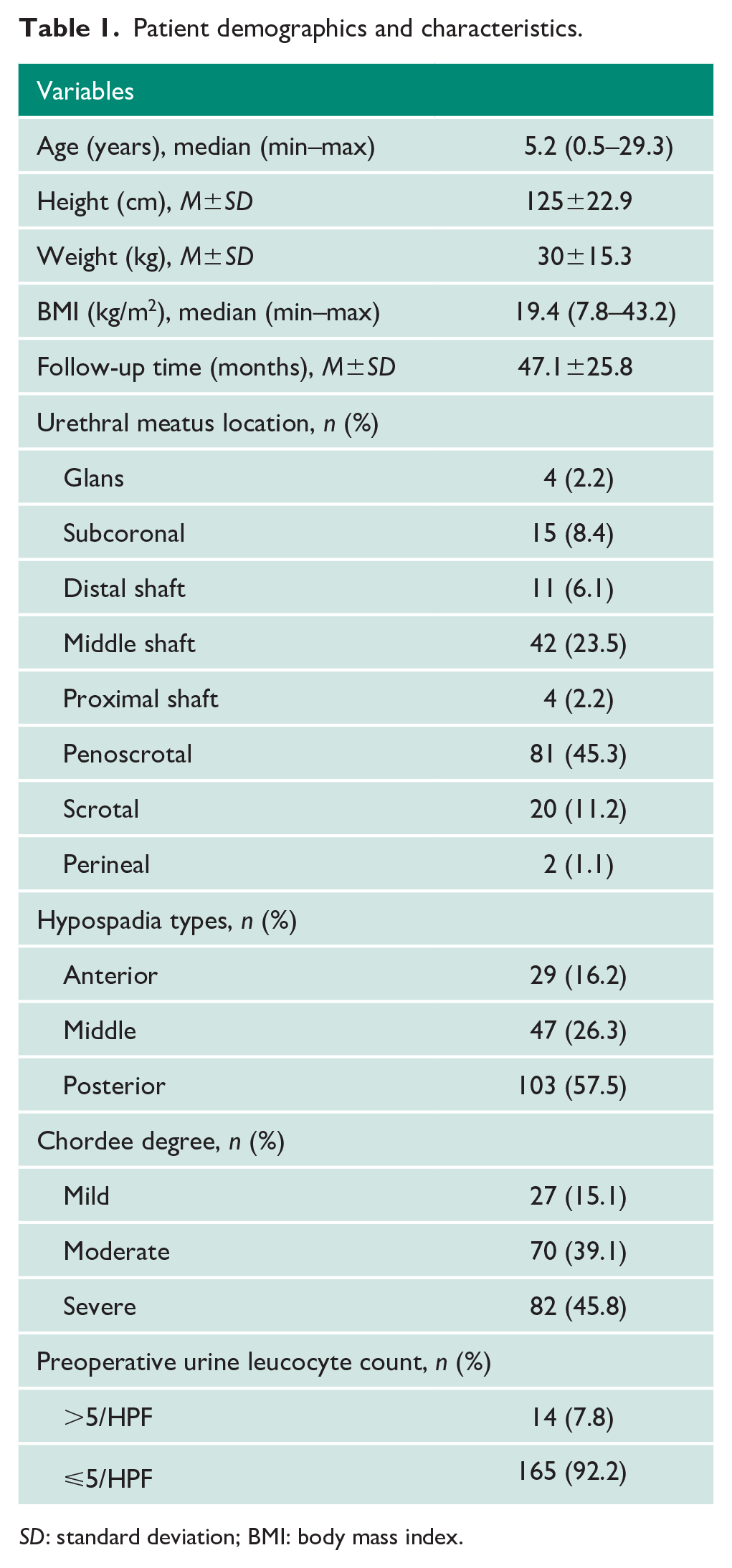
SD: standard deviation; BMI: body mass index.
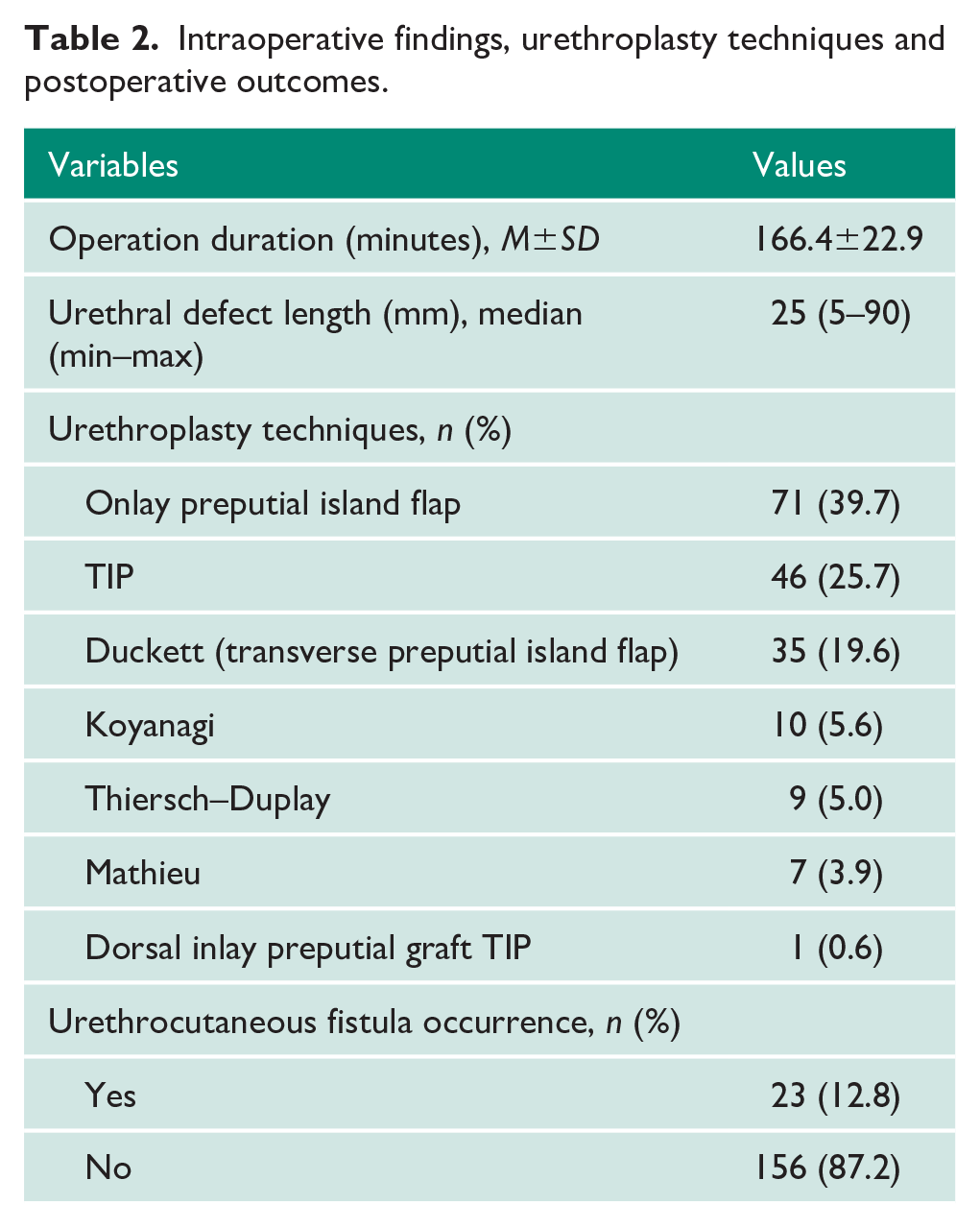
Onlay preputial island flap was the most versatile single-stage urethroplasty technique used at our institution (39.7%), followed by TIP (25.7%) and Duckett (19.6%), as shown in Table 2. Urethrocutaneous fistulas occurred in 23 (12.8%) cases, with most happening in the first months after surgery (5.4±3.3 weeks). Significant systemic or localized infection was not noted in our patients postoperatively. The fistula rate was quite similar between TIP (8.6%), onlay island flap (11.2%), Duckett (11.4%) and Thiersch–Duplay urethroplasty (11.1%). The highest fistula rate occurred in the Koyanagi (40%) and Mathieu urethroplasty groups (28.5%). One successful case of dorsal inlay preputial graft TIP was done in a one-year-old child with distal penile hypospadias, mild chordee and short urethral defect (10 mm).
Intraoperative findings, urethroplasty techniques and postoperative outcomes.
We found that the incidence of urethrocutaneous fistulas varied between type of hypospadias (Table 3). The highest incidence of urethrocutaneous fistula occurred in posterior hypospadias (22.6%), followed by anterior (7%) and middle (4%) hypospadias.
Variables and their association with urethrocutaneous fistula occurrence.
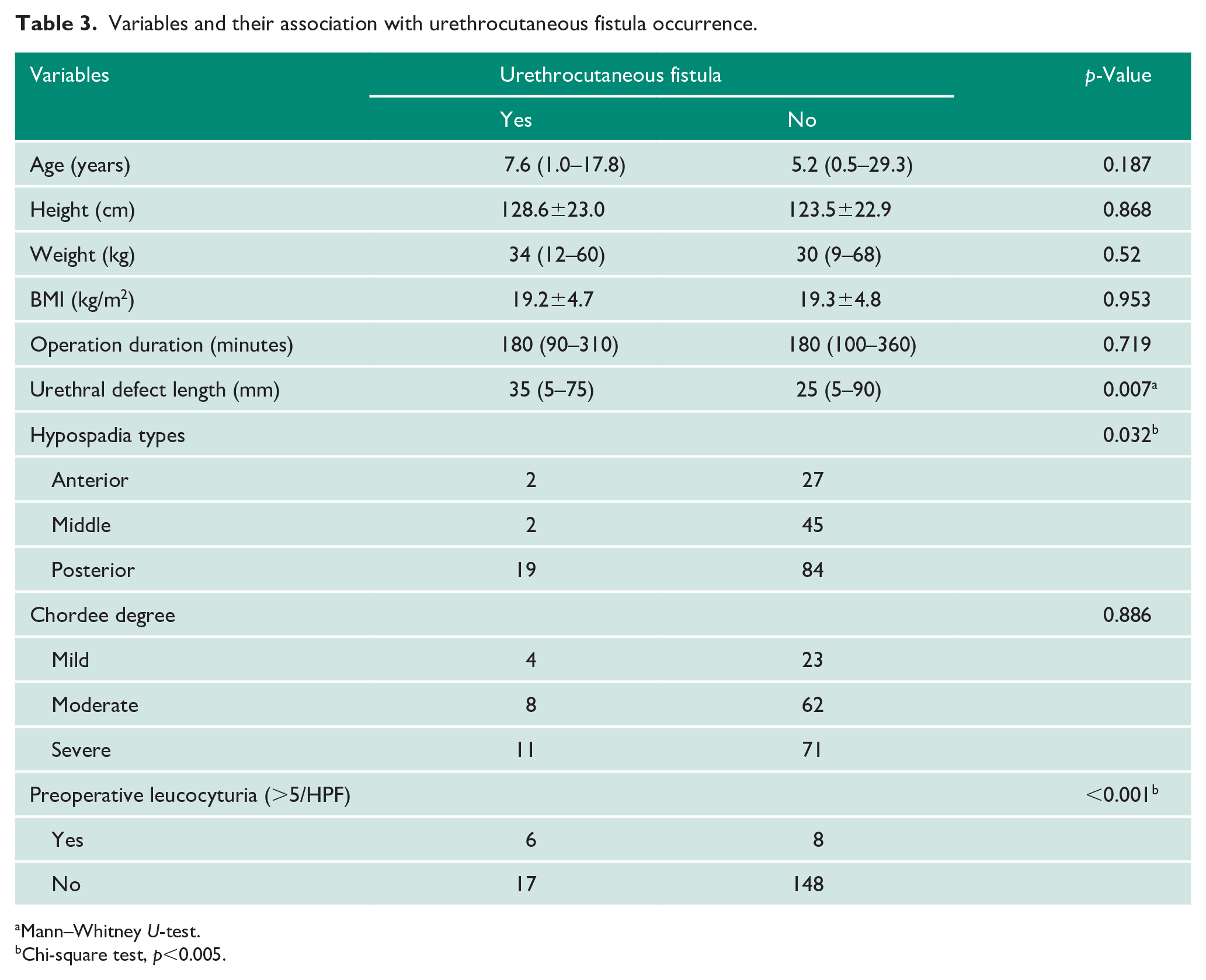
Mann–Whitney U-test.
Chi-square test, p<0.005.
Data analysis showed that a longer urethral defect length, posterior hypospadias and preoperative leucocyturia played a significant role in urethrocutaneous fistula after single-stage urethroplasty, while chordee degree and age were not associated with urethrocutaneous fistula occurrence (Table 3).
Discussion
Hypospadias is hypoplasia of the ventral penile tissue beyond the division of the corpus spongiosum with an abnormal meatus position and penile ventral deviation (chordee) and/or ventral prepuce deficit with abundant dorsal prepuce. Recent guidelines propose simpler classifications of mild (glanular or penile hypospadias without concomitant chordee, micropenis or scrotal anomaly) and severe (penoscrotal or perineal hypospadias with concomitant chordee and scrotal anomalies). 10 However, we adopted Duckett’s hypospadias classification preoperatively which has been satisfactory for decades.
Urethrocutaneous fistula is the most common complication following urethroplasty, and often emerges early (<12 months) at the coronal-subcoronal level with/without glans dehiscence or late (>12 months) after urethroplasty.2,11–13 In our study, urethrocutaneous fistula occurred after 5.4±3.3 postoperative weeks (1.3±0.8 months). This is comparable to previous studies by Snodgrass2,14 and Faase 15 which discovered that urethrocutaneous fistula could occur three to six months postoperatively.
Overall, the fistula rate in our study was considerably lower (12.8%) compared to other studies, which reported a 31–32.5% risk of fistula.1,8,13,16 This might be explained by our strict study criteria, with surgeries undertaken by expert consultants, and is similar to the rate observed by Khan et al. (19.6%).1,17 A study by Chung et al. reported a higher fistula rate (21.4%) in 294 boys who underwent single-stage urethroplasty. 18 However, a recent systematic review showed that the fistula rate was much lower (7.5%), which could be explained by a large proportion of anterior hypospadias (82.1%). 19
In contrast to previous studies,15,18 we utilized a short 6 Fr silastic stent inside the pendulous urethra, since regular urethral stents or catheters may suffer from blockages, kinking and knotting, which complicates the stent-removal process. 12 Due to the ‘cuffing’ phenomenon, a silicone catheter with no more than 2 mL balloon inflation is recommended rather than standard latex. 20 Additionally, suprapubic drainage might divert urine from the neourethra and aids fistula healing after two to three weeks of usage. 12 The most recent study by Duarsa et al. also concluded that percutaneous cystotomy could decrease the risk of urethrocutaneous fistula (odds ratio=2.963, p=0.014). 21
Our study suggests that posterior hypospadias, longer urethral defect and preoperative leucocyturia played a significant role in the formation of urethrocutaneous fistula. Similar to previous studies, posterior hypospadias was associated with urethrocutaneous fistula and reoperation after urethroplasty.16,18,20,22 Hardwicke et al. and Lu et al. also reported that posterior hypospadias had a higher risk of urethrocutaneous fistula compared to anterior hypospadias (17–25% and 5.8–8%, respectively). Moreover, according Sheng at al., a longer urethral defect was associated with a higher risk of urethrocutaneous fistula, which is similar to our result. 8
We found that preoperative leucocyturia had a statistically significant association with the incidence of urethrocutaneous fistula. However, studies on this particular topic are limited. Although the exact mechanism is unknown, the study by Sheng et al. is the only known study clearly reporting that preoperative leucocyturia is associated with fistula incidence. 8 Previous studies have indicated that UTI and local flora contamination could increase the risk of fistula formation.12,23 However, using leucocyturia as a sign of UTI is still debated. The study by Yanagahira reported that false positives are common in leucocyturia examination using a dipstick. 24 Another study reported that postoperative bacteriuria was a common phenomenon found in up to 51% cases, and thus broad-spectrum prophylaxis and postoperative antibiotics were recommended in order to decrease the risk of UTI which may contribute to fistula formation. 23 Other studies reported that pre- and postoperative positive swab results may contribute to wound infection and suggested antibiotic therapy based on the preoperative perimeatal swab.25,26 Our study did not show significant local or systemic infection postoperatively, with a relatively low overall fistula rate, which we considered to be a result of the use of prophylaxis or early antibiotics in patients with leucocyturia followed by postoperative maintenance antibiotics.
In this study, onlay preputial island flap and TIP were most suited for anterior-middle (42.3–56.5%) to posterior (43.5–57.5%) hypospadias, with a low fistula rate (8.6% and 11.2%, respectively). Initially utilized for mid-distal hypospadias, onlay island flap and TIP have been adopted for proximal and complicated hypospadias with a similar fistula rate (7.6–21%) and complication occurrence.5,6,17 Pfistermuller et al. reported that 4675 patients underwent TIP with a low fistula rate on primary distal hypospadias repair compared to primary proximal and secondary repair (5% vs. 10.3% vs. 15.5%, p<0.005). 27 Xiao et al. 28 demonstrated that onlay island flap and TIP had a similar complication rate (14–47% vs. 13.5–60%) and better cosmesis for proximal hypospadias repair.28,29 We found that Duckett techniques were primarily used for posterior hypospadias (85.7%), with a fistula rate of 11.4%. As we adopted the classical suprapubic diversion and urethroplasty technique, the complication rate was similar (7.5–10%) to the ones reported by Duckett.4,30
Our study has several shortcomings, since retrospective studies might pose selection bias. Most patients in this study might have educational and economical limitations which contribute to poor treatment compliance. As a result, data were procured from past medical records and surveys. Further prospective studies with strict periodical follow-up are needed to record the complication rate after single-staged urethroplasty.
Conclusion
Single-staged urethroplasty is a versatile procedure for various hypospadias cases, with an overall urethrocutaneous fistula rate of 12.8%. Posterior hypospadias, preoperative pyuria and longer urethral defect were associated with urethrocutaneous fistula formation.
Footnotes
Acknowledgements
The authors would like to thank Cipto Mangunkusumo Hospital for the support in finishing this article.
Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical approval
This study has been approved by Ethics Committee of Cipto Mangunkusumo Hospital – Faculty of Medicine University of Indonesia (No. KET-991/UN2.F1/ETIK/PPM.00.02/2019).
Informed consent
Written informed consent was obtained from the patients for their anonymized information to be published in this study.
Guarantor
A.D.S.
Contributorship
A.D.S. was responsible for ethical approval, data collection, researching the literature, writing the draft and finalising the manuscript. G.R. was involved in protocol development, administration of the study, data analysis, manuscript writing and manuscript finalization. I.R. contributed to the conceptualization, administration of the study, funding, data analysis and manuscript editing and finalization. A.R. was involved in protocol development, study conceptualization, patient recruitment and manuscript editing and finalization.