
Abstract
Objective:
This study aimed to investigate the association between Photodynamic Diagnosis (PDD) with hexaminolevulinate (HAL) and the rate of complete resection and disease persistence at first follow-up cystoscopy for non-muscle-invasive bladder cancer (NMIBC) in UK real-world practice.
Methods:
Audit data were pooled from six UK centres where HAL PDD was used in patients with a new NMIBC diagnosis undergoing transurethral resection of bladder tumours (TURBT) since 2008. Patients received adjunctive intra-vesical therapy and surveillance in line with European and UK guidelines, including early re-resection in high-grade NMIBC.
Results:
PDD-assisted TURBT was done in 837 patients with new NMIBC. The detrusor muscle was present in 69.4% of cases. At early re-TURBT in 207 high-risk patients, 13.0% had residual disease. Multifocal disease was the most significant factor in increasing the rate of residual disease (odds ratio excluding cases of CIS=4.1; 95% confidence interval 1.5–11.3). The recurrence rate at first follow-up cystoscopy (RRFFC) was 10.6% (8.9% in patients with complete initial TURBT). In the historical cohort undergoing good-quality white-light TURBT, RRFFC was 31%; 40.5% of high-risk patients had residual disease at early re-TURBT.
Conclusion:
HAL PDD may increase the rates of complete resection, reducing the risk of early recurrence and the need for routine re-resection in high-grade NMIBC.
Level of evidence:
2b.
Keywords
Introduction
Transurethral resection of bladder tumours (TURBT) is the mainstay of treatment for non-muscle-invasive bladder cancer (NMIBC). However, although the intention of such treatment is curative, recurrence rates are high, necessitating regular and often prolonged follow-up. 1 As a result, bladder cancer places a heavy and long-term burden on health-care resources and on patients. 2
The European Association of Urology recommends repeat TURBT after two to six weeks for patients at high risk of recurrence. 1 For example, the prevalence of tumour persistence in patients with Ta and T1 tumours has been reported at approximately 39–47%.3,4 However, a blanket policy of early re-resection is burdensome for service providers and patients alike. We believe that the rate of residual disease after initial resection could be reduced by emphasising better-quality initial TURBT, thus obviating the need for default early re-resection in every high-risk case.
Clinical trials and real-world experience show that use of photodynamic diagnosis (PDD; also known as fluorescence cystoscopy) increases detection of tumours, especially carcinoma in situ (CIS), compared to white-light cystoscopy (WLC) alone and improves clearance of tumour margins.5–7 Long-term follow-up of the largest randomised clinical trial of hexaminolevulinate (HAL) indicates that this improved detection translates into a clinically significant reduction in recurrence-free survival (p=0.04), 8 with a trend towards reduced progression rates compared to WLC. 9
To date, there is limited evidence on the role of HAL PDD in reducing residual disease at early re-TURBT, with one single-centre study (N=446) indicating a significant reduction in recurrence rate at the six-week re-TURBT from 31.2% with WLC to 11.1% with PDD (p=0.0001). 10 The objective of the present analysis was to describe residual disease rates and recurrence in a large population of patients, using pooled audit data from an ongoing collaboration between urological teams at seven centres across the UK.
Methods
Data were collected as an audit of outcomes/quality prospectively (Edinburgh) or retrospectively (Barnet, Middlesbrough, Exeter, Bridgend and Basingstoke) on all new NMIBC patients receiving HAL PDD-guided cystoscopy or TURB-T from 2008 until May 2011 in the participating centres, with analysis focusing on risk of residual disease at early re-TURBT in patients with high-grade NMIBC, recurrence rate at the first follow-up cystoscopy (RRFFC) and comparison of the above end points between TURBT guided by PDD (PDD-TURBT) and TURBT performed under white-light (WL-TURBT) in a historical cohort from Edinburgh.
Medical procedures
Mitomycin C was given to all patients within 24 hours of initial resection in most centres unless contraindicated or if it was felt inappropriate by the clinician. Further intra-vesical instillation of mitomycin C or bacille Calmette–Guérin (BCG) in line with European and UK guidelines was dependent on local policy following discussion at the multidisciplinary meeting. None of the patients received BCG prior to the early re-TURBT, and a six-week course of mitomycin C was used in only one centre for 16 patients with intermediate-risk NMIBC.
In patients with high-grade NMIBC, re-TURBT was performed within six weeks of initial TURBT, and cystoscopy+biopsy was performed at three months where re-TURBT was felt inappropriate by the local team. High-grade NMIBC was defined according to the World Health Organization 1973 and 2004 classifications as high-grade (anaplastic) CIS or papillary urothelial carcinoma (PUC). All patients with low- to intermediate-risk NMIBC had the first check cystoscopy at three months. Completeness of resection post TURBT was assessed visually by the consultant carrying out the TURBT or by the supervising consultant if the TURBT procedure was carried out by a trainee.
Data collection
To ensure uniform data reporting and minimise bias across centres, a standardised pro forma based on bladder mapping and tumour features (Figure 1) was used to collect specific information, including tumour size, number, appearance, completeness of resection, use of mitomycin C, clinical stage, presence or absence of detrusor muscle in the resection specimen and surgeon experience. Residual or recurrent disease was defined as histologically proven cancer on resection or biopsy. RRFFC was used as a measure of the quality of TURBT and therefore included results from early re-TURBT for high-grade NMIBC, as well as data from the three-month follow-up visit in patients with low- or intermediate-risk disease.
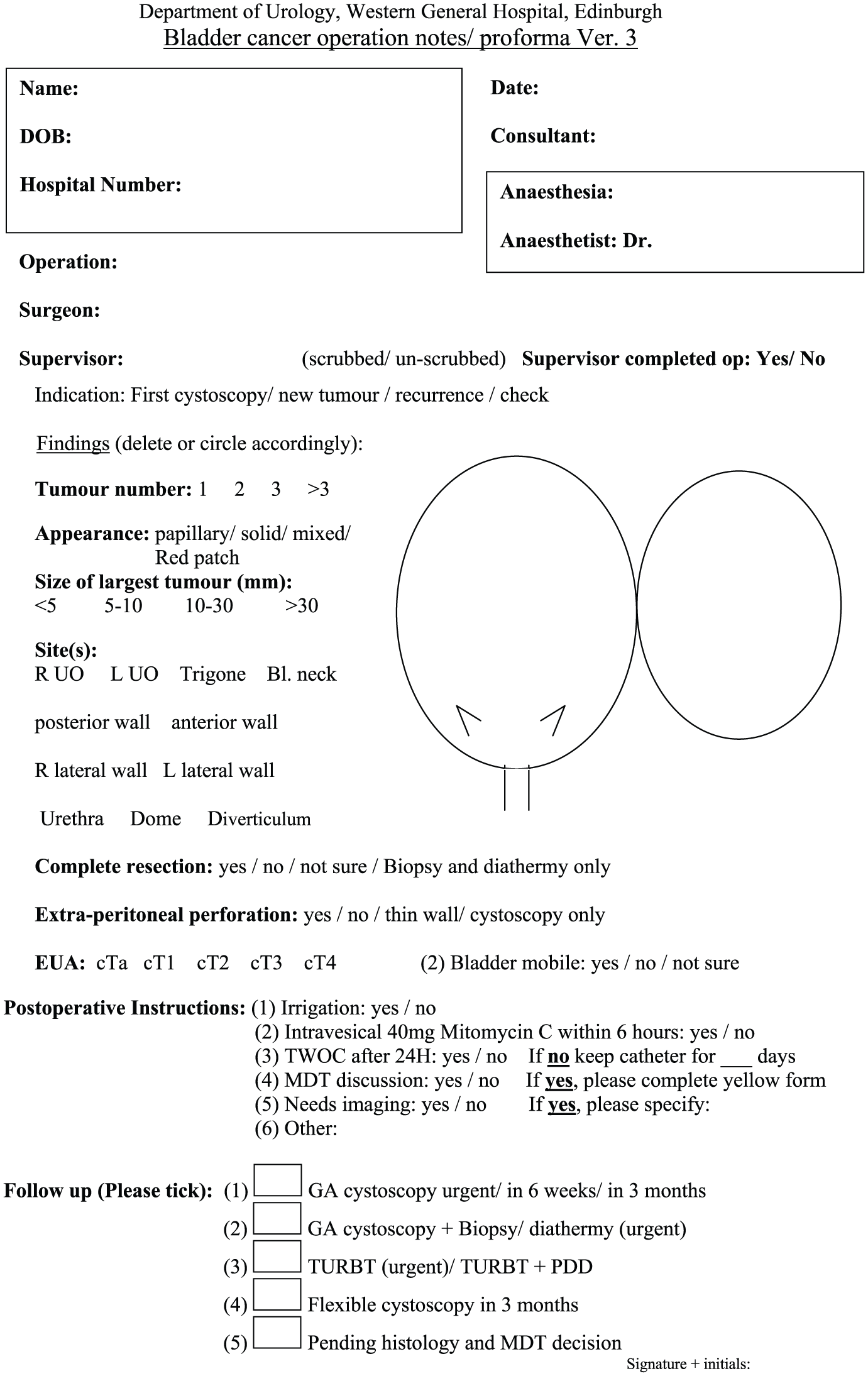
Bladder cancer operation notes/pro forma v3.
As this was a single-arm analysis of routinely collected data, no sample size calculation was performed. Multivariate logistic regression analysis was carried out where appropriate. Statistical analysis was carried out using SPSS for Windows v16 (SPSS, Inc., Chicago, IL). To provide a real-world context in which to assess the impact of PDD, early recurrence rates in patients undergoing PDD-TURBT were also compared informally to those in a control group of patients from one of the centres (Western General Hospital, Edinburgh, UK) who had received good-quality WL-TURBT (GQ-WLTURBT) involving (a) cystoscopic mapping using a bladder diagram, (b) documented complete resection of the tumour, (c) resection performed or supervised by an experienced surgeon (consultant or trainee at year 5 or beyond), (d) presence of detrusor muscle in the specimen and (e) mitomycin C instillation within 24 hours after the resection. Detailed findings for this control group have been published previously.6,11
Results
In total, PDD-assisted surgery was carried out in 1127 patients, of whom 1008 had new bladder cancer of any stage (including stages T2–T4). The present analysis focuses on the 837 patients with new NMIBC, comprising 295 from Edinburgh, 192 from Basingstoke, 163 from Barnet, 85 from Middlesbrough, 64 from Exeter and 38 from Bridgend. The mean age of patients with newly diagnosed NMIBC was 70.5 years. Baseline demographics are described in Table 1.
Patient demographics, tumour characteristics and surgeon category at first transurethral resection of the bladder for all patients with newly diagnosed NMIBC.
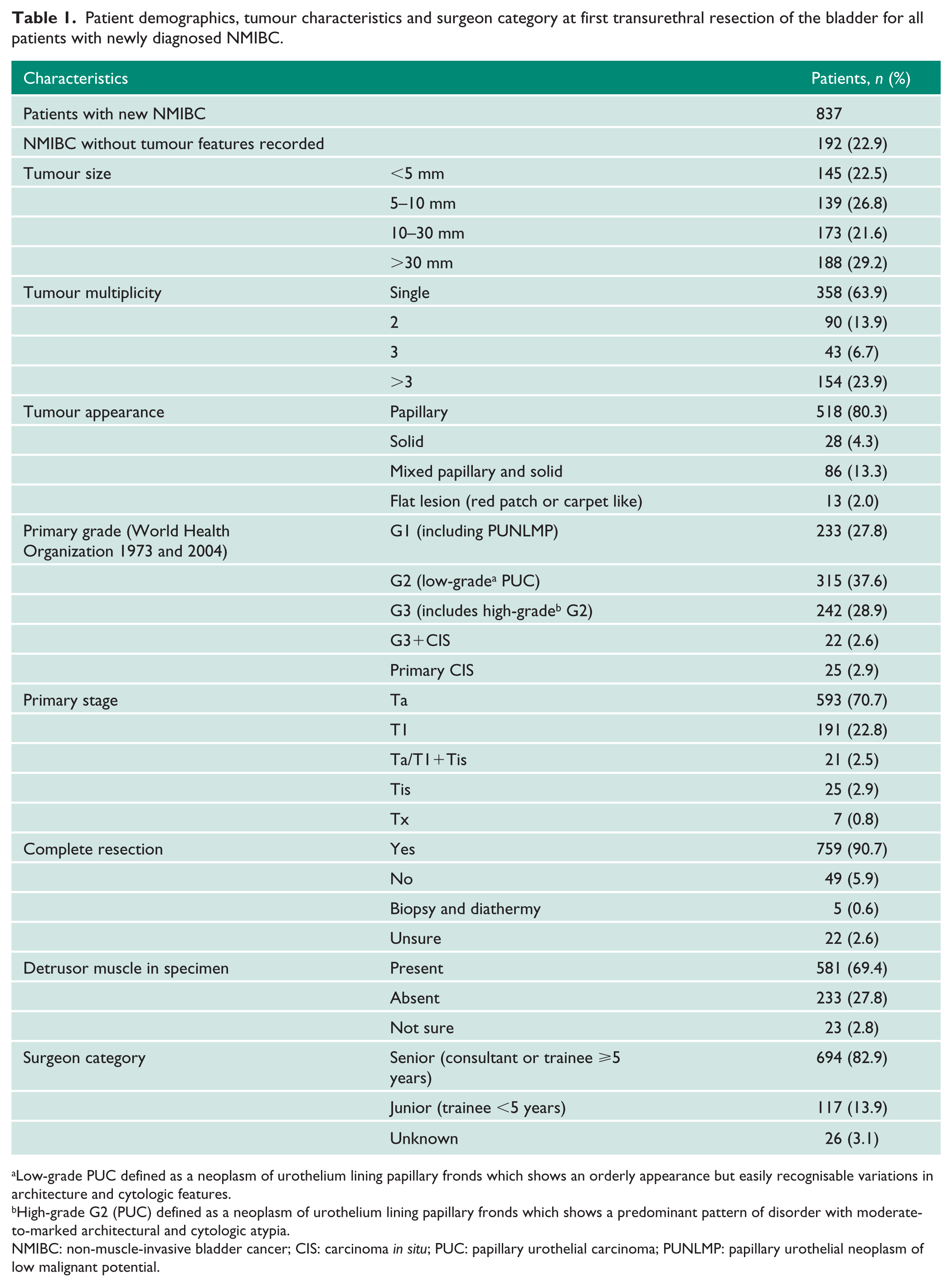
Low-grade PUC defined as a neoplasm of urothelium lining papillary fronds which shows an orderly appearance but easily recognisable variations in architecture and cytologic features.
High-grade G2 (PUC) defined as a neoplasm of urothelium lining papillary fronds which shows a predominant pattern of disorder with moderate-to-marked architectural and cytologic atypia.
NMIBC: non-muscle-invasive bladder cancer; CIS: carcinoma in situ; PUC: papillary urothelial carcinoma; PUNLMP: papillary urothelial neoplasm of low malignant potential.
Overall, 759 (90.7%) patients with new NMIBC were deemed by the surgeon to have had a complete initial PDD-TURBT; the remainder had incomplete resection, were managed with biopsy and fulguration or the completeness of resection was uncertain. The detrusor muscle was present in 581 (69.4%) NMIBC cases.
At early re-TURBT, residual disease was found in 27 (13.0%) of 207 cases of high-grade NMIBC, with upstaging to T2 cancer in three (1.5%) cases. Table 2 describes the association between primary tumour features and residual disease in patients with high-grade NMIBC, excluding those with CIS (n=167). Patients with multiple tumours, solid- or mixed-appearing tumours and T1 tumours appeared more likely to have residual disease following complete PDD-TURBT for high-grade NMIBC compared to the historical control group. 6 Residual cancer was found in 22 (17.6%) of 125 patients with the detrusor muscle present in the specimen and in eight (19.1%) of 42 patients when the detrusor muscle was absent.
Univariate and multivariate regression analysis to determine association between primary tumour features and risk of residual disease following initial complete PDD-TURBT for high-grade NMIBC.
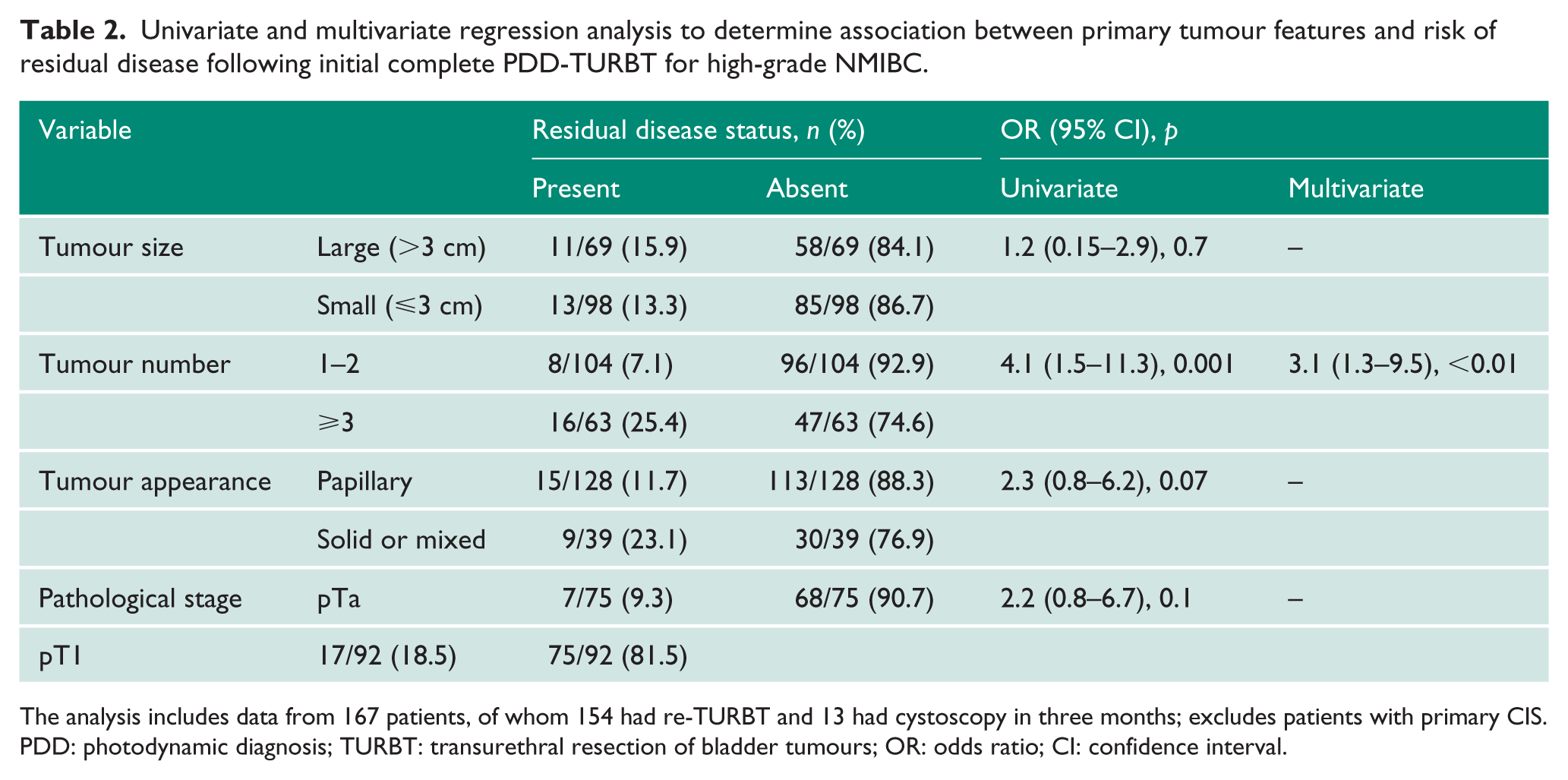
The analysis includes data from 167 patients, of whom 154 had re-TURBT and 13 had cystoscopy in three months; excludes patients with primary CIS.
PDD: photodynamic diagnosis; TURBT: transurethral resection of bladder tumours; OR: odds ratio; CI: confidence interval.
The overall RRFFC (including early re-TURBT for high-grade NMIBC) following complete PDD-TURBT was 8.9%. Table 3 describes RRFFC and recurrence rates at one year stratified by baseline recurrence risk groups.
Recurrence rates at first follow-up cystoscopy (RRFFC) and at one year (RR-1y).
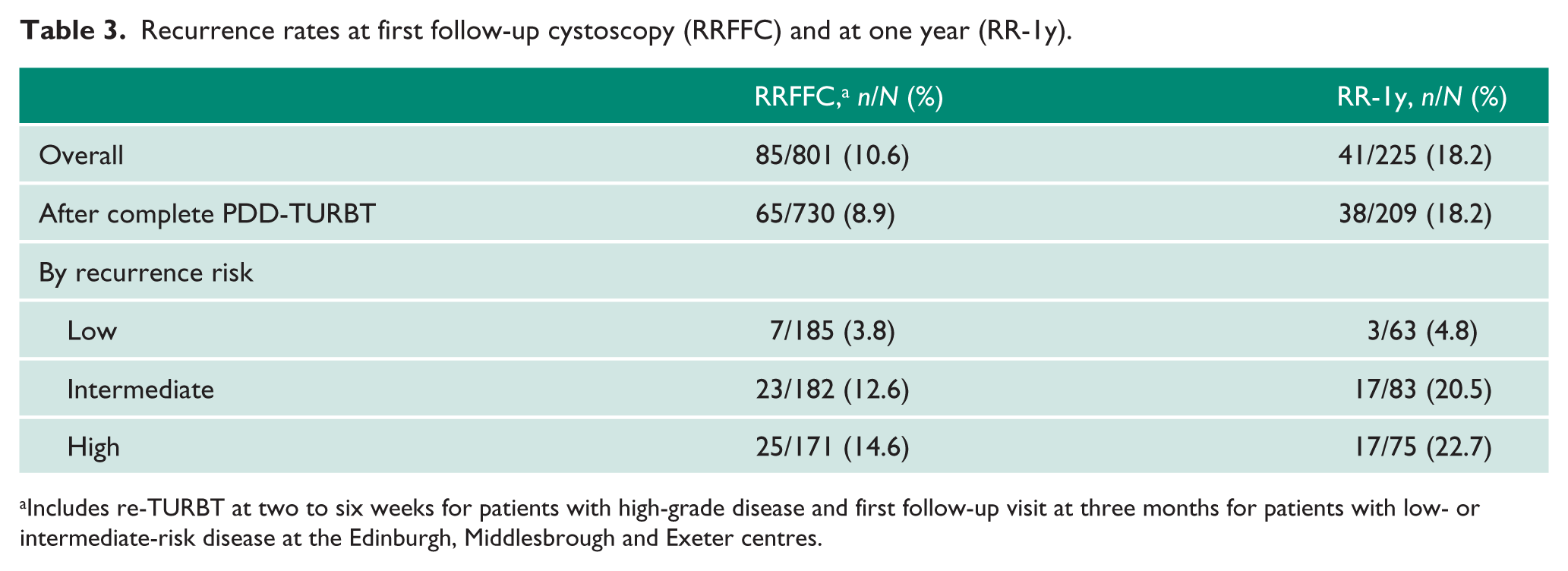
Includes re-TURBT at two to six weeks for patients with high-grade disease and first follow-up visit at three months for patients with low- or intermediate-risk disease at the Edinburgh, Middlesbrough and Exeter centres.
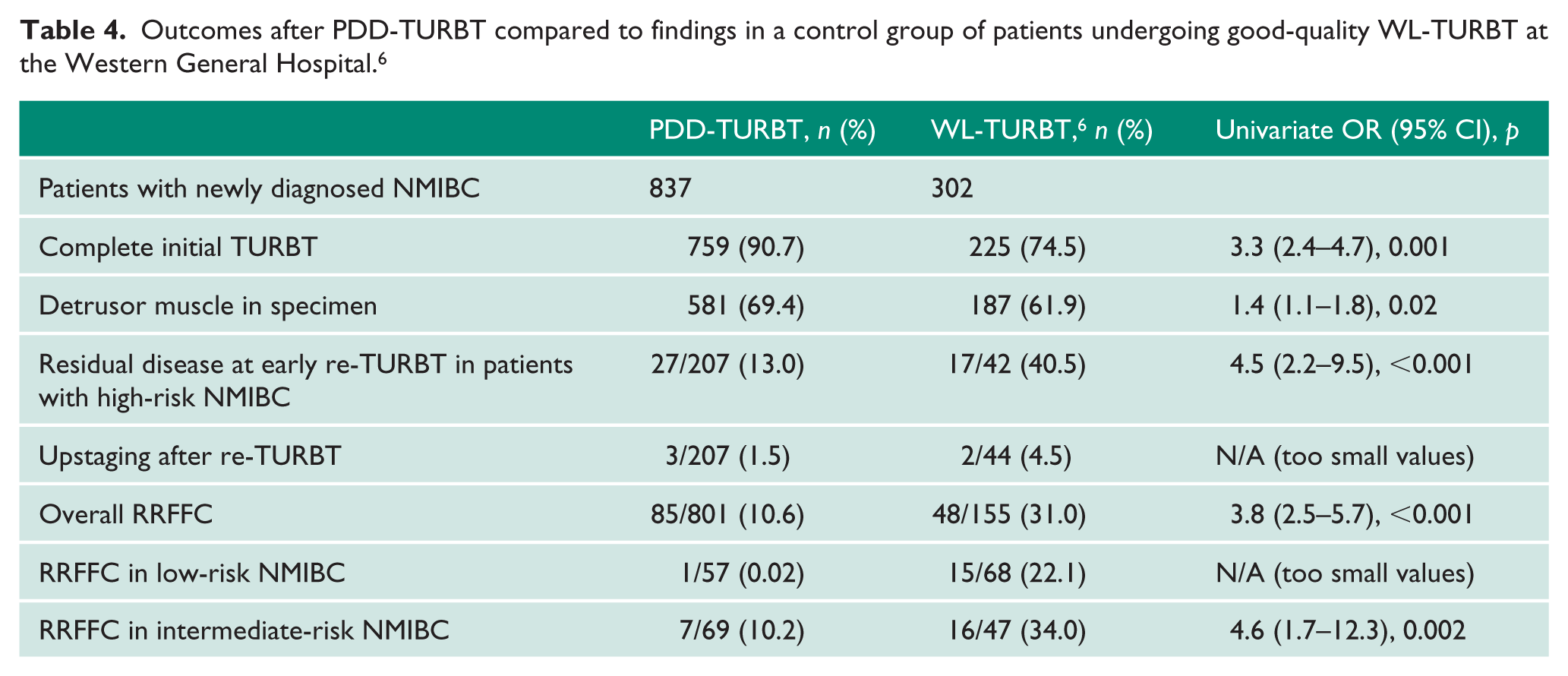
Respective end points in the historical control group of patients undergoing GQ-WLTURBT are shown in Table 4. 6
Outcomes after PDD-TURBT compared to findings in a control group of patients undergoing good-quality WL-TURBT at the Western General Hospital. 6
Discussion
This audit by the UK PDD Users Group has collected records from more than 1000 patients to date, providing the largest evidence base for HAL and for PDD in the UK, as well as being one of the largest patient pools globally. This collaboration represents the first multi-centre study in the UK to collect real-world data on recurrence/residual disease rates with HAL PDD.
In our study, RRFFC with PDD was 11%, the detrusor muscle was absent in only 31% of specimens and the residual disease rate was only 13% of high-grade NMIBC cases. This is in line with the 11% residual disease rate observed with the use of advanced optical imaging tools in the study by Geavlete et al. 10 and appears favourable in comparison to historical studies of early re-TURBT, where residual disease rates of up to 76%12,13 and rates of complete resection (including muscle) of 20–84%14–16 were observed.
This analysis is a single-arm audit, without a contemporary control group. However, the results can be considered in light of experiences at one of the centres (Western General Hospital), which offers a historical control group of patients managed by experienced urologists who were also involved in the present audit. Despite the GQ-WLTURBT, the RRFFC was 31%, with 40.5% residual disease at early re-TURBT in high-risk patients, and the detrusor muscle was absent in almost 40% of specimens. 6
The reduction in residual disease and recurrence rates could be attributed to: the high level of experience of the surgeons performing TURBT; good-quality training, with overall improved attention to detail and close supervision; dedicated lists for TURBT at participating centres; including the detrusor muscle in the specimen11,17; state-of-the-art cystoscopes and video equipment; and use of advanced optical imaging tools such as PDD. In addition, the number of incorrectly staged patients was minimal (1.5% in our study compared to up to one third in historical TURBT series13,15,16). This means that appropriate treatment is initiated without delay.
With such potential to improve detection and resection with PDD in the majority of patients, we hypothesise that the number of cases requiring early re-TURBT could be substantially reduced, allowing resources to be prioritised in the subgroups most likely to benefit. One such subgroup is those with multifocal disease, which was found to be the most significant factor in increasing the residual disease rate. Another subgroup that could benefit is those where the muscle is absent from the specimen. Indeed, in a large multi-centre cohort, Gontero et al. found that re-TURBT had no impact on recurrence, progression, cancer-specific survival or overall survival in cases where the muscle was present in the initial resection specimen. 18 This has been shown to be an indicator of high-quality resection. 19 The use of PDD could potentially reduce the burden of repeat surgery and its possible complications, including the risk of tumour seeding and spread, in other patient subgroups such as those with large lesions or only one or two stage T1 lesions. 20 This approach would currently be at odds with international guidelines1,21 but, if validated by further research, could represent a new direction of travel to reduce the burden of NMIBC management on patients and health-care services.
We believe that we have provided an important foundation on which to build a long-term evidence base for the use of HAL PDD in the management of NMIBC. Our aim in the future is to try to standardise prospectively collected information on each PDD case across centres, so that, in time, we can undertake high-quality analyses of consistent data from as large a pool of patients as possible. We encourage all centres using HAL PDD to join this initiative, regardless of how much experience they currently have, as one of our aims is to show the increasing benefit of PDD over time, not just in terms of improving results versus WLC, but also because we believe that PDD can improve our surgical technique overall.
Limitations
The audit results that we present here come from both prospectively and retrospectively collected data from different centres, with varying levels of experience using HAL PDD and with, in some cases, restrictions on the patients in whom HAL PDD is used. In addition, each centre initially set up its own methods of recording details for each patient. The heterogeneity of the data and limited information available for some of the factors that potentially influence outcome need to be borne in mind when considering our results. For example, data on the use of mitomycin C are only available from the Edinburgh centre, where 74% of patients received a single mitomycin C instillation within 24 hours of initial cystoscopy. Such challenges with data collection from multiple UK centres in relation to bladder cancer were also experienced in the BAUS radical cystectomy audit, where only 37% of in the Hospital Episode Statistics data were entered into the database with significant data heterogeneity. 22
Conclusion
In conclusion, our audit data suggest the use of HAL PDD may improve bladder visualisation, thereby increasing the probability of complete resection and reducing the risk of recurrence. This was evident in this multi-centre audit across all risk groups, including those with high-grade or multifocal tumours or CIS. Further high-quality, prospective data collection across UK centres is needed to confirm this.
Footnotes
Acknowledgements
We would like to thank OPEN Health Medical Communications for assistance with the preparation of the article.
The initial meetings of members of the UKPDD Users Group were made possible through financial support from GE Healthcare, Amersham, UK. The authors thank Sarah Etheridge PhD of Open Health Medical Communications, London, UK for providing medical writing support, which was funded by Ipsen SA in accordance with Good Publication Practice Guidelines. The authors retained editorial control over the content.
Conflicting interests
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: this collaboration was supported by Ipsen.
Ethical approval
This is an audit of practice and outcomes.
Informed consent
This is an audit of practice and outcomes.
Guarantor
All authors.
Contributorship
P. M. conceived the study and designed the pro forma for data collection, in collaboration with all authors. All authors were involved in data collection. P.M. carried out data analysis. P.M. wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.