
Abstract
Background:
A 76-year-old male presenting with macroscopic haematuria was found to have a lobulated mass infiltrating along the urothelium at the site of insertion of the upper moiety of a complete duplex right kidney. Suspected of being upper tract urothelial carcinoma, cystoscopy, bilateral retrograde pyelograms and transurethral resection of bladder tumour were attempted. Intra-operative findings revealed no tumour burden in the bladder or left ureter. The insertion of the upper pole moiety of the right ureter was not identified intra-operatively. Pelvic MRI demonstrated a markedly dilated upper pole moiety of the right ureter with a soft tissue mass in its distal aspect. Interestingly, the distal portion of the ectopic upper pole moiety was found to insert into the bladder neck.
Objective and Methods:
We report on an unusual case of upper tract urothelial carcinoma arising from the upper moiety of a complete duplex kidney. Our aim was to demonstrate the importance of thorough investigation of suspected urothelial carcinomas occurring in association with variant upper tract anatomy.
Results and Conclusion:
This case demonstrates the importance of thorough radiological and endourological investigation of suspected upper tract urothelial carcinoma and the various congenital abnormalities that may complicate the surgical management of this common malignancy.
Level of evidence:
4 (case report)
Case
The case is of a 76-year-old man with multiple comorbidities including severe COPD secondary to his extensive smoking history and atrial fibrillation (AF) treated with a DOAC who was referred by his GP with two episodes of self-limiting macroscopic haematuria and a CT urography (CTU) suggestive of urothelial carcinoma within the bladder.
The CTU reported a complete duplex system on the right side, with a significantly dilated upper pole moiety. At the site of the insertion of the accessory ureter, there was a lobulated mass infiltrating along the urothelium measuring 36 mm in length, highly concerning for upper tract urothelial carcinoma (UTUC). Figure 1 shows the images identifying the suspicious mass as well as a partially contrast filled bladder to show distinction between the dilated ureter and bladder.
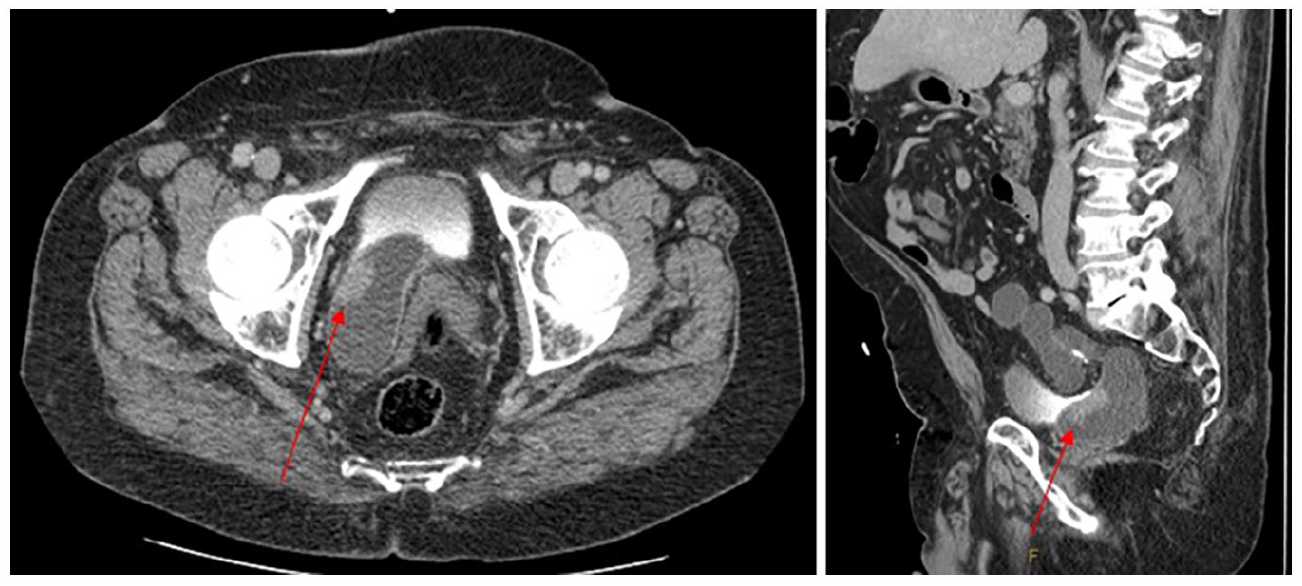
CT urography showing significantly dilated upper pole moiety and a lobulated mass at the site of the insertion of the accessory ureter.
He underwent a cystoscopy, bilateral retrograde pyelogram and attempted transurethral resection of bladder tumour (TURBT). Intra-operatively bilateral retrograde pyelograms were performed revealing a normal left ureter and right lower pole moiety. No mass was found within the bladder and, despite an extensive search, the upper pole moiety ureteric insertion was not identified.
After discussion at the urology multi-disciplinary team (MDT) meeting, he was further investigated with a pelvic MRI to assess the presence of any extra-ureteral/rectal involvement. The MRI (Figure 2) revealed a markedly tortuous and dilated upper pole moiety with a distinct soft tissue mass in the distal ureter without evidence of local invasion. Following the findings of the MRI, and given the presence of several significant co-morbidities and the presence of a normal contralateral kidney, it was decided that the patient should undergo radical nephroureterectomy with resection of both duplicated ureters. Intra-operatively, the distal portion of the ectopic upper pole ureter was found to insert into the bladder neck.
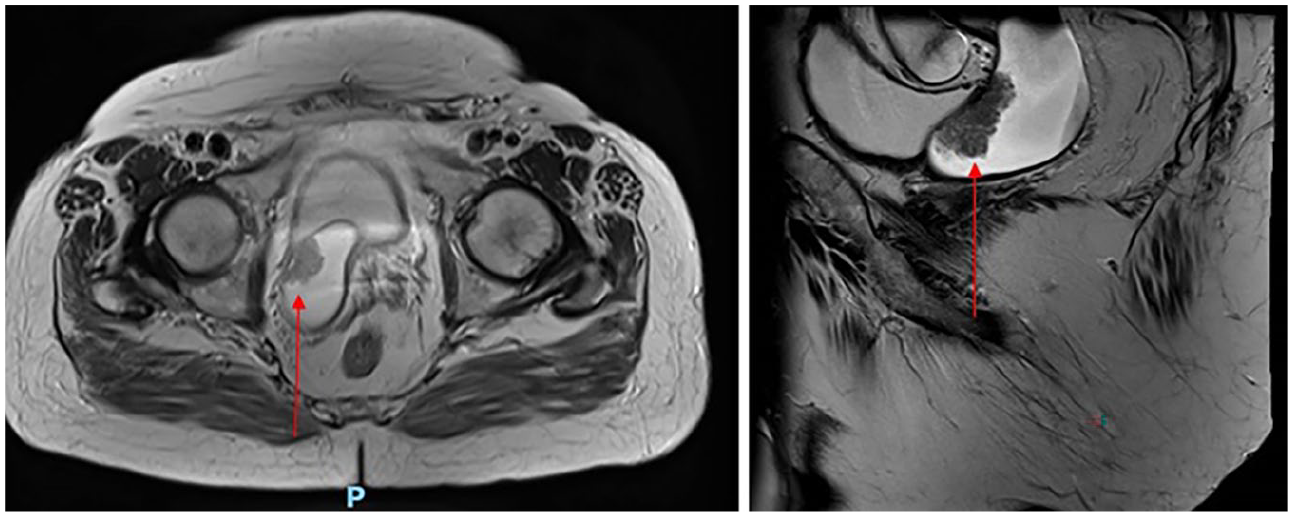
MRI T2 weighted images of the pelvis with gadolinium enhancement displaying the urothelial carcinoma in greater detail.
Histopathological analysis revealed two ureters: a normal lower pole ureter and a markedly dilated upper pole ureter (the size difference between these ureters is readily appreciable in Figure 3), with an isolated fibrotic distal end that contained a 35-mm papillary lesion within the lumen. The distal portion of this ureter was seen to communicate with the prostatic urethra which is the likely cause of his self-limiting haematuria. The majority of the papillary urothelial carcinoma was non-invasive low grade; however, there were areas of focal high grade and carcinoma in situ (CIS). There were some areas displaying invasion of the tumour 0.5 mm into the lamina propria but the surgical margins were clear.
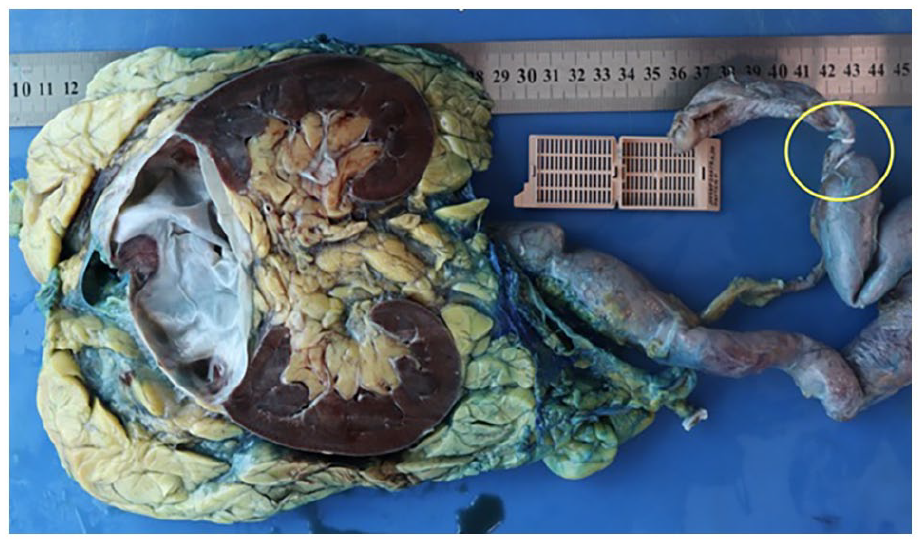
Macroscopic dissection of the entire kidney and ureter showing the dilated ureter and a burnt out upper pole.
To our knowledge, there have been only four cases described of urothelial carcinoma arising in ectopic or duplex systems. This is the fifth case of such described, and the second case describing insertion into the prostate.
Discussion
This case was an interesting mix of pathology and congenital abnormality, combining upper tract urothelial carcinoma, ureteric ectopia, as well as ureteric duplication.
Complete or partial duplication of the renal collecting system is the most common congenital abnormality of the urinary tract and has a reported incidence of 0.8–5%. 1 However, the true incidence is difficult to determine due to its frequently asymptomatic nature. 1
Ectopic ureteric insertion occurs along the path of the developing mesonephric system. 2 The posterior urethra is the most common insertion point of ureteric ectopic in men and accounts for half of all cases 1 with one-third of cases inserting into the seminal vesicles. The vas deferens, bladder neck, prostate and epididymis make up the rest of the usual ectopic insertion points. 2
Ectopic ureters are frequently associated with duplex kidney, with some reports suggesting concurrence in up to 75–90% of ectopic ureters, and approximately 10% of cases of ureteric ectopia are bilateral.2 –4 Females are more commonly affected than males, at a ratio of around 6:1.3,4
In contrast, urothelial carcinoma is the ninth most common malignancy worldwide, and the fourth most common in developed countries. 5 It is the only cancer of the 15 most common malignancies in Australia for which the survival rate is decreasing. 6 Urothelial carcinoma accounts for 90% of bladder cancers worldwide, with a reported incidence of between 140 and 300 per 100,000 in men, depending on their age. 7
Tumours of the upper urinary tract occur more frequently in men compared to women at a ratio of almost 2:1, and the average age at diagnosis is 73 years. 8 The incidence of upper urinary tract tumours has slowly increased over the past few decades; however, there has been an associated shift towards earlier stage disease. 6
In all, 70–80% of patients with upper urinary tract malignancy present with haematuria, and ureteric obstruction causing flank pain in 20–40%.5,8 Other urinary tract symptoms, such as irritative lower urinary tract symptoms, and constitutional symptoms of malignancy occur in less than 10% of cases. 5
There are multiple risk factors that have been associated with the development of urothelial carcinoma, such as chemical carcinogenesis from smoking or occupational exposures. Occupational carcinogen exposure is thought to account for approximately 10–20% of bladder cancers. 9 However, in Western countries, smoking is the most prevalent and worrisome risk factor.7,9 A study of 740 patients over 22 years has shown that patients with heavier smoking histories were more likely to have higher grade tumour and muscle invasive disease at their original presentation. 7
A number of environmental and genetic causes have been associated with the preferential development of UTUC including Chemical carcinogenesis (cigarette smoking, occupational exposure), Balkan endemic nephropathy, Lynch syndrome (lifetime risk for urologic cancer estimated at 8%), arsenic exposure, analgesic abuse, and Chinese herb nephropathy.5,8,10 The incidence of UTUC is between 0.91 and 1.15 per 100,000 in the United States between 1997 and 2005 and accounts for between 5% and 10% of all urothelial carcinomas.5,7,8
Of the patients with UTUC, 17% have concurrent bladder tumours and thus the entire urinary tract should be visualised to ensure synchronous disease is managed appropriately. 5 Between 40% and 50% of cases of UTUC have a history of bladder cancer, or will develop subsequent bladder involvement, and thus ongoing monitoring for patients with UTUC is mandatory.5,8 Due to the significant risk of recurrence of urothelial carcinoma, the gold standard treatment of upper tract urothelial carcinoma is total ureterectomy and nephrectomy for high-risk disease, regardless of location. 5
There is no conclusive evidence to attest to the safety of a partial nephrectomy in suitable candidates who present with UTUC isolated to a single moiety of their duplex renal system. There are concerns that disruption to the integrity of the collecting system and shared vessels that occurs during partial nephrectomy can cause seeding of tumour cells downstream. 11 There is also reported UTUC found in both moieties of a duplex collecting system, highlighting the possibility of radiologically undetectable tumour being present in both moieties, which would render single-moiety excision ineffective. 12
Conclusion
This case highlights the importance of multidisciplinary approach to urothelial carcinoma. It is a disease that has multiple risk factors, presentations and treatments and is an area of interest with an increasing body of research being performed – which is particularly relevant to the Australian population due to the increasing mortality from urothelial cell carcinoma. This is a highly unusual case of a complete duplex ureter with a distal ureteric carcinoma with associated ectopia insertion at the bladder neck.
Footnotes
Acknowledgements
We would like to thank the patient for their permission to produce this case report. We would like to thank A.R. for his guidance and support in writing this article.
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical approval
Hunter New England Health does not require ethical approval for reporting individual cases.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.
Guarantor
A.R.
Contributorship
B.S. and V.T. researched literature and conceived the study. B.S. and V.T. wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.