
Abstract
In addition to hypercholesterolemia, innate and adaptive immune mechanisms play a critical role in atherogenesis, thus making immune-modulation therapy a potentially attractive way of managing atherosclerotic cardiovascular disease. These immune-modulation strategies include both active and passive immunization and confer beneficial reduction in atherosclerosis. Preclinical studies have demonstrated promising results and we review current knowledge on the complex role of the immune system and the potential for immunization as an immune-modulation therapy for atherosclerosis.
Introduction
Atherosclerotic plaques contain features of an innate and adaptive immune system, such as dendritic cells (DCs), B and T lymphocytes, macrophages, Toll-like receptors, immunoglobulins, inflammatory cytokines and complements. Interested readers can refer to the listed references for an in-depth discussion on the complex role of these immune components in atherogenesis [Andersson et al. 2010; Chyu et al. 2011; Hartvigsen et al. 2009; Lundberg and Hansson, 2010; Yan and Hansson, 2007].
Many reports have described the possibility of active or passive immune-modulation strategy to modulate atherosclerosis. In the English literature, based on a PubMed search using ‘immunization’ and ‘atherosclerosis’ as keywords, the first such possibility was raised by Gero and colleagues in 1959 [Gero et al. 1959]. However, only in the past decade have we seen an explosive increase in the amount of literature published on this subject. This change is most likely due to our better understanding of the role of immune system in atherosclerosis and advances in research tools available to scientists. Some parts of this article were already reported in our previous review [Chyu and Shah, 2013] and are represented here for completeness of this article.
Immunization against atherosclerosis
Immunization, in a classical immunological paradigm, can be classified as active or passive. Active immunization relies on the delivery of antigens in a vaccine platform to induce humoral and cellular immunity against the offending agents in the host. This would involve activation of many arms of the immune system, such as B and T cells, to generate effector cells such as antibody-producing B cells or cytotoxic CD8+ T cells. Passive immunization consists of administration of a preformed antibody such as various antitoxins or immunoglobulin against infectious agents to achieves its effect against offending agents.
Search for antigens involved in atherosclerosis
No matter which immunization approach is used for disease prevention or treatment, the most important element of the immunization approach is to know which antigens are responsible for the disease. Many antigens have been implicated and reported to be associated with atherogenesis. These include endogenous antigens such as low-density lipoprotein (LDL) or its related protein apolipoprotein B-100 (apoB-100) [Ameli et al. 1996; Fredrikson et al. 2003b, 2005; Freigang et al. 1998; Palinski et al. 1995], oxidized phospholipid and its phosphorylcholine (PC) head group [Binder et al. 2003, 2004; Binder, 2010; Chou et al. 2009], heat shock protein 65 (HSP65) [Kilic and Mandal, 2012; Mandal et al. 2004, 2005; Xu et al. 2012] and β2 glycoprotein I (β2-GPI) [George et al. 2000a, 2000b; Matsuura et al. 2005; Shoenfeld et al. 2001]. Exogenous infectious agents such as Chlamydia pneumoniae, periodontal pathogens or cytomegalovirus were also reported to play some role in atherogenesis [Armitage, 2000; Ausiello et al. 2005; Beck et al. 1999; Betjes et al. 2007; Buhlin et al. 2003; Halme et al. 1997; Mayr et al. 2000; Movahed, 1999; Olofsson et al. 2005; Zelkha et al. 2010]. The establishment of these molecules as potential antigens in atherogenesis is usually based on the presence of humoral or cellular immune responses against such molecules in animal or human studies and their presence in atherosclerotic plaques.
Circulating antibodies against low-density lipoprotein in humans
Circulating antibodies against LDL (or its oxidized forms, oxLDL) exist in humans. In a prospective study of 30 men with accelerated progression of carotid atherosclerosis in 2 years, higher autoantibodies to malondialdehyde-modified (MDA) LDL were found compared with age-matched controls [Salonen et al. 1992]. In a case control study, patients with early onset of atherosclerotic peripheral vascular disease had higher levels of autoantibodies against oxLDL in addition to higher levels of total cholesterol, LDL and triglycerides [Bergmark et al. 1995]. Another study revealed a higher level of autoantibodies against copper oxLDL in patients with established coronary artery disease compared with controls without disease [Lehtimaki et al. 1999].
The clinical utility and significance of these antibodies is not clearly known. In an observational study with asymptomatic patients from the Atherosclerosis Risk in Communities study cohort, there was no correlation between MDA-LDL autoantibody and intima-media thickness (IMT) [Iribarren et al. 1997]. However, Fukumoto and colleagues found a modest inverse relationship between oxLDL antibody titers and carotid IMT in healthy Japanese people [Fukumoto et al. 2000]. In another study examining patients with a diagnosis of myocardial infarction, ischemia or undergoing coronary revascularization procedures, there was no relationship between the antibody titer and risk of death and cardiovascular disease events [Erkkila et al. 2005].
Taking these together, these data suggest the presence of autoantibodies against LDL is likely a marker for the presence of disease, indicating an activation of immune response against oxLDL.
Passive immunization
Passive immunization using immunoglobulin can largely be divided into an antigen specific or nonspecific approach. Intravenous administration of immunoglobulin (IVIG) is an example of an antigen nonspecific approach. IVIG has been used in clinical practice to treat immune-mediated diseases such as autoimmune diseases or transplant rejection. Since atherosclerosis is viewed as an autoimmune disease of arterial wall, proof-of-concept preclinical studies testing the efficacy of using polyclonal immunoglobulin to reduce atherosclerosis have reported promising results [Nicoletti et al. 1998; Yuan et al. 2003]. This atheroprotection has been attributed to the ability of IVIG to modulate T-cell activities or antibody production [Nicoletti et al. 1998] and a complement system is required for its full effect [Persson et al. 2005]. Our laboratory recently reported the use of a polyclonal immunoglobulin M (IgM) in a different model of atherosclerosis. We observed that treatment with polyclonal IgM weekly for 4 weeks reduced existing spontaneous and accelerated atherosclerotic lesions induced by periarterial cuff injury in the carotid artery [Cesena et al. 2012]. This protective effect was associated with downregulation of CD4+ T-cell activity and enhancement of oxLDL IgG titers [Cesena et al. 2012]. Taking these together, polyclonal antibodies likely exert their atheroprotective function by modifying the immune system globally, which could also be a potential weakness of this approach.
Passive immunization using monoclonal antibodies against specific antigens has also been reported to confer atheroprotective effects. Monoclonal IgG preparations reactive to cardiolipin or LDL significantly reduced atherosclerotic lesion formation in LDL receptor (–/–) (LDLR(–/–)) mice [Grosso et al. 2008; Nicolo et al. 2003]. Another monoclonal IgG2b antibody against electronegative LDL was also reported to decrease atherosclerosis in LDLR(–/–) mice, possibly by reducing the circulating level of free electronegative LDL and cholesterol oxides in the plasma and liver [Grosso et al. 2008]. Whether these monoclonal antibodies modulate humoral or cellular immune response against atherosclerosis as a potential mechanism of action was not elucidated. Although these antibodies were monoclonal, the exact antigenic epitope in cardiolipin or LDL that these antibodies recognize are not known.
Recently a recombinant human IgG1 antibody against an MDA-modified apoB-100 derived peptide antigen, named p45, was shown to reduced/regress atherosclerosis in animal models [Schiopu et al. 2004, 2007]. This antibody proved to be safe in a phase I human trial and showed anti-inflammatory activity in a primate model [Li et al. 2013]. However, a subsequent phase IIa clinical study, which used an inflammatory index in the arterial wall measured by 18-fluorodeoxyglucose positron emission tomography/computed tomography imaging as an endpoint, failed to achieve the prespecified endpoint (see http://www.news-medical.net/news/20120711/BioInvent-announces-data-from-BI-204-phase-IIa-study-on-stable-atherosclerotic-vascular-disease.aspx). However, there are considerable limitations in the imaging methodology that was used in this study, making it difficult to rule out the possibility that an inappropriate study design may have contributed to the negative results.
IgM antibody preparation was also effective in conferring atheroprotective effects. Natural antibodies, produced by B1 cells, are primarily of the IgM subtype and their production does not require antigen exposure. One such natural IgM antibodies, discovered by Dr Witztum’s group, is EO6, which targets oxidized lipid products, the PC headgroup in phospholipids and apoptotic cells [Binder, 2012]. EO6 is of the T15 idiotype and a monoclonal preparation of IgM against the PC headgroup with T15 idiotype has been shown to reduce accelerated vein graft atherosclerosis [Faria-neto et al. 2006]. Recently another monoclonal IgM antibody with specificity for hypochlorite oxLDL was produced and found to be a natural IgM. Passive immunization with this preparation led to a reduction of pericarotid cuff induced atherosclerotic lesions in LDLR(–/–) mice [van Leeuwen et al. 2013]. The polyclonal IgM preparation also reduced aortic atherosclerotic lesions with concomitant modulation of CD4+ T-cell response [Cesena et al. 2012]
Although these studies suggest the feasibility of passive immunization to modulate atherosclerosis, human application still awaits confirmatory clinical studies. Even with proven clinical efficacy in the future, its clinical application could still be limited due to the following factors: passive immunization lacks memory effect; for a long-term effect, it may require frequent administration of antibody which could be costly; cost and safety of producing such antibody; safety of such an antibody due to frequent administration and many immunosuppressive properties associated with polyclonal immunoglobulin; and lack of knowledge of antigenic epitopes in many of these antibody preparations may hinder the improvement of this strategy.
Active immunization with antigens related to low-density lipoprotein
In the mid 1990s, several publications reported that active immunization using native modified LDL as an antigen reduced atherosclerosis in hypercholesterolemic rabbits [Ameli et al. 1996; Nilsson et al. 1997; Palinski et al. 1995] (Table 1). Several other groups of investigators subsequently reported similar atheroprotective effects by active immunization with cholesterol-rich liposomes in cholesterol-fed rabbits [Alving et al. 1996], MDA-modified LDL in apoE(–/–) mice [George et al. 1998b] or with plaque homogenates or MDA-modified LDL in apoE(–/–) mice [Zhou et al. 2001].
A summary of antigens that have been tested in preclinical active immunization studies and their effects on atherosclerosis.
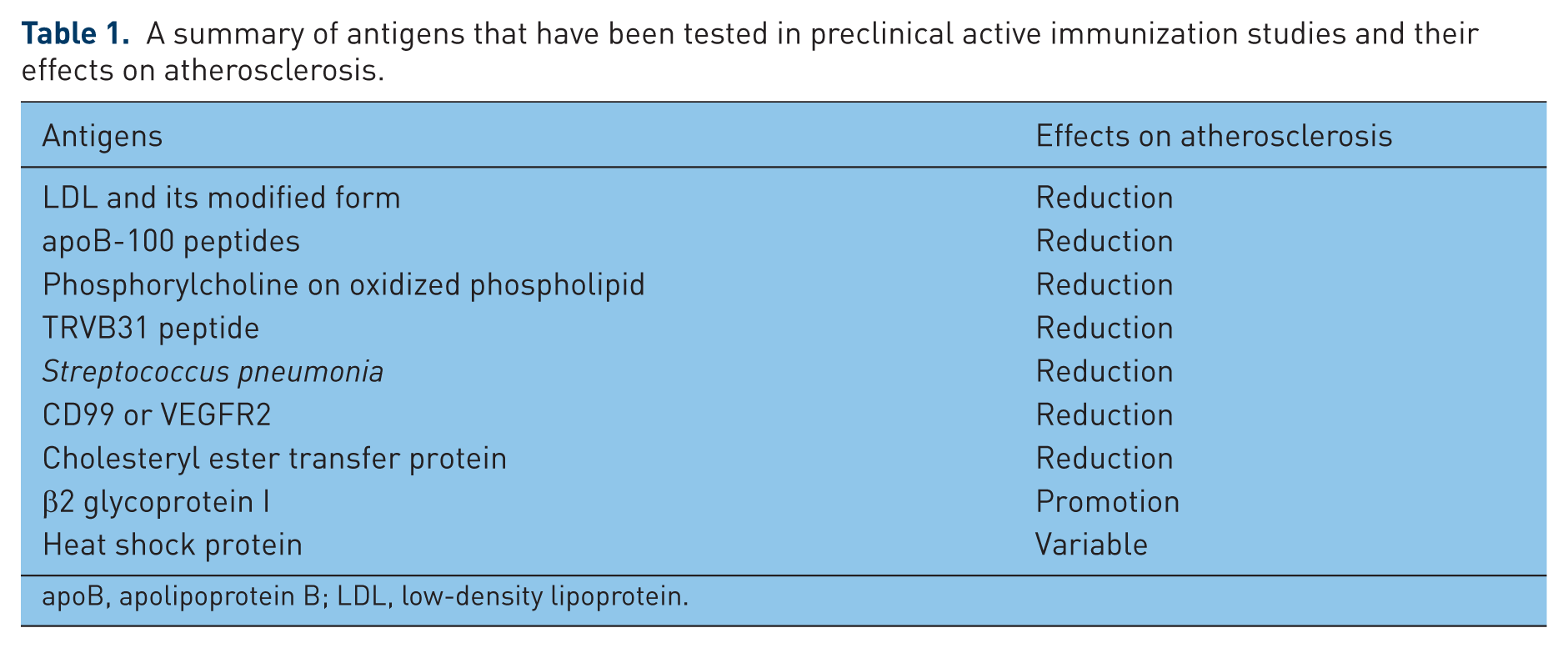
apoB, apolipoprotein B; LDL, low-density lipoprotein.
LDL is not an ideal antigen because of its large size and its heterogeneous molecular contents including apolipoprotein, cholesteryl ester, triglyceride and phospholipids. This complex molecular structure makes it difficult to determine the exact immunogenic epitopes within the LDL molecule. In the early 2000s, our laboratory in collaboration with Dr Jan Nilsson’s laboratory in Sweden launched an extensive effort to identify potential antigenic epitopes within the protein component of LDL, apoB-100, that could be used as antigens to achieve atheroprotective effects via immunization. We first generated a library of 302 peptides (20 amino acids long with a 5-amino-acid overlap with the preceding sequence) using sequences from the human apoB-100 molecule and identified 102 peptides that can be recognized by antibodies in pooled human plasma from healthy control subjects [Fredrikson et al. 2003a]. Active immunization with vaccine formulations using several such peptides, such as p2, p143 and p210, as antigens resulted in a 40–70% decrease in atherosclerosis and reduction in plaque inflammation in hypercholesterolemic mice [Chyu et al. 2005; Fredrikson et al. 2003b].
After successful demonstration of the ability of specific apoB-100 peptides as antigens in vaccine formulation to reduce atherosclerosis, we and other investigators continued to investigate the humoral and cellular mechanisms responsible for the atheroprotective effect of immunization using such peptides. Most of the mechanistic work used p210 as the model antigen in the vaccine formulation.
Humoral immunity was initially speculated to mediate the protective effect of active immunization. However, the atheroprotection of immunization using apoB peptide as antigen occurred without an increase in peptide-specific IgG [Fredrikson et al. 2008]. Klingenberg and colleagues reported that intranasal immunization with p210 elicited IgG titers against p210 but the titers were not correlated with the lesion size [Klingenberg et al. 2010]. We also reported that mice immunized with p210 vaccine developed smaller aortic atherosclerotic lesions with lower titer of circulating p210 IgG compared with mice in control groups. Additionally, adoptively transferring B cells from p210 immunized mice to nonimmunized mice did not convey an atheroprotective effect [Chyu et al. 2012]. Hence the existing evidence does not support humoral immunity as an important mediator for the atheroprotective effect of active immunization with p210.
The focus of mechanistic work then shifted to cellular immunity. Immunizing apoE(–/–) mice with p210 could activate CD8+ T cells with concomitant reduction of DCs at the site of immunization and within the plaques, decrease macrophage immunoreactivity in plaques and significantly reduce aortic atherosclerosis compared with controls. The atheroprotective effect of active immunization could be recapitulated by adoptive transfer of CD8+ T cells from p210-immunized mice into naïve, nonimmunized mice. CD8+ T cells, as effectors, from p210 immunized mice developed a preferentially higher cytolytic response against p210-loaded DCs in vitro. There was no protective CD4+ T-cell response as evidenced by lack of activation of CD4+ T cells and transfer of CD4+CD25+ T cells from p210-immunized donors did not provide atheroprotection in the naïve recipient mice [Chyu et al. 2012].
Immunization with p210 peptide also elicits changes in CD4+ T cells. Using an immunization schedule and preparation similar to ours, Wigren and colleagues reported that male apoE(–/–) mice immunized with p210 generated a functional CD4+CD25+ T-cell response and reduced atherosclerosis. Administration of CD25 blocking antibody ablated the increase of CD4+CD25+ T cells and the associated atheroprotection by p210 immunization [Wigren et al. 2010]. However, the authors acknowledged several limitations in their study, including lack of a control group of mice receiving adjuvant and the possibility of CD25 blocking antibody ablating both CD25+ effector T cells and regulatory T cells together [Wigren et al. 2010]. Klingenberg and colleagues used a different approach to deliver p210 for immunization. They generated a recombinant protein by fusing p210 with cholera toxin B (p210-CTB) and delivered it to female apoE(–/–) intranasally twice weekly for 12 weeks. Mice receiving ovalbumin peptide fused with CTB (OVA-CTB) or phosphate-buffered saline served as control groups. They observed a reduction of atherosclerosis in aortic sinuses in mice receiving p210-CTB treatment compared with the other two groups with no difference in FoxP3, interleukin (IL)-10 or transforming growth factor β (TGFβ) mRNA expression in aorta between p210-CTB and OVA-CTB groups. There was no difference in the numbers of FoxP3+ cells in aortic lesions or CD4+FoxP3+ T cells in lung mucosa. However, there was a higher percentage of IL-10+ subset of splenic CD4+ T cells from p210-CTB immunized mice and they were functional to suppress the effector CD4+ T cells. The authors suggested that these CD4+IL-10+ T cells (called Tr1 type of regulatory T cells) could potentially mediate the beneficial effect of intranasal immunization with p210-CTB [Klingenberg et al. 2010]. Another group of investigators reported that delivering a mixture of apoB-100 peptides (p210, MDA-p210 and p240, 3.3 µg each, total 10 µg) for 2 weeks subcutaneously via an implanted mini-osmotic pump reduced atherosclerosis in aortic sinus compared with control groups of mice [Herbin et al. 2012]. Additional experiments showed that such protection could be achieved by delivering p210 peptide alone, indicating p210 is the major peptide responsible for the atheroprotective effect among the three tested peptides. Such protection was associated with a decreased activation of CD4+ T cells and reduced interferon γ, IL-10 and IL-4 cytokine production upon stimulation ex vivo and increased the CD4+CD25+FoxP3+ subset of T cells in lymph nodes. Ablation of CD25+ T cells by CD25-depleting antibody also abrogated the atheroprotection by apoB-100 peptide infusion.
Taking the above reports together, it is clear that the beneficial effect of p210 immunization relies on cellular immune responses. It is possible that both atheroprotective and atheropromoting T cells exist within the CD4+ and CD8+ T cells. Only through a detailed delineation of subtypes of CD4+ and CD8+ T cells and testing their roles in atherosclerosis by an adoptive transfer strategy can we fully understand and delineate how cellular immune responses after apoB-100 peptide immunization influence atherogenesis. The overall beneficial effect of p210 immunization likely depends on the balance of quantity, strength and timing of appearance of all the elicited immune responses.
There may not be a universal mechanism to explain the effect of immunization using apoB-100 peptides as different apoB-100 peptides could elicit different immune responses. A strong CD4+CD25+FoxP3+ T-cell response can be induced by p2 immunization whereas immunization with p210 induced the least response. Both p2 and p45 elicited a CD8+CD25+FoxP3+ T-cell response compared with the carrier control group but p210 showed the opposite effect [Pierides et al. 2013]. Nevertheless p210 is currently a strong candidate to be developed into future potential human applications given that immunization with p210 consistently reduces atherosclerosis even when it is administered via different routes and in different forms.
Active immunization with antigens unrelated to low-density lipoprotein
A series of publications from Dr Witztum’s group described a natural IgM antibody recognizing the epitopes in oxLDL [Friedman et al. 2002; Horkko et al. 1999] and PC headgroups on the surface of apoptotic cells and inhibits uptake of oxLDL and apoptotic cells in macrophages(Table 1) [Chang et al. 1999; Horkko et al. 1999; Shaw et al. 2000]. Immunization against PC in apoE(–/–) mice elicited antibodies against PC and oxLDL, resulting in reduced atherosclerotic lesions at the aortic root [Caligiuri et al. 2007]. Given that anti-PC antibodies protect against infection from Streptococcus pneumoniae [Briles et al. 1982; Yother et al. 1982], active immunization in LDLR knockout mice with Streptococcus pneumoniae resulted in a modest reduction of atherosclerosis [Binder et al. 2003]. However, human studies failed to show consistent cardiovascular protective effects of pneumococcal vaccine [Hung et al. 2010; Lamontagne et al. 2008; Siriwardena et al. 2010; Tseng et al. 2010].
Dr Göran Hansson’s group described T-cell clones, obtained by immunizing human apoB-100 transgenic mice with human oxLDL, recognizing only native LDL or purified apoB-100. These T-cell clones showed uniform expression of a single T-cell receptor variable β chain, TRVB31. Anti-TRVB31 antibodies generated from immunization with a peptide from TRVB31 blocked T-cell recognition of apoB-100 and reduced atherosclerosis [Hermansson et al. 2010].
Dr Kuiper’s group reported that an orally administered DNA vaccine against CD99 or VEGFR2 generated antigen-specific cytotoxic CD8+ T cells with associated reduction in murine atherosclerosis [Hauer et al. 2007; van Wanrooij et al. 2008].
Cholesteryl ester transfer protein (CETP), a key enzyme involved in high-density lipoprotein (HDL) metabolism, has been used as an antigen in active immunization. Immunization with CETP induced neutralizing antibodies and in turn led to a marked elevation of HDL with concomitant reduction in atherosclerosis in rabbits [Gaofu et al. 2005; Mao et al. 2006; Rittershaus et al. 2000] but human studies were disappointing [Davidson et al. 2003].
HSPs are another groups of proteins that have been implicated in atherogenesis [Almanzar et al. 2012; Grundtman et al. 2011; Grundtman and Wick, 2011; Kilic and Mandal, 2012] but the effect of immunization with HSPs on atherosclerosis has been inconsistent. Immunization with HSP65 induces atherosclerotic lesions in several reports [George et al. 1999; Xu et al. 1992; Zhang et al. 2012]; whereas others reported reduced atherosclerotic lesions [Klingenberg et al. 2012; Long et al. 2012]. Tolerance induction by oral HSP60 or nasal immunization of HSP65 reduced atherosclerosis as well [Maron et al. 2002; van Puijvelde et al. 2007]. Immunization with apoB-100 and HSP60 peptides was also reported to confer atheroprotection [Li et al. 2011; Lu et al. 2010].
β2-GPI, a major target for antiphospholipid antibodies, is another vital molecule that has been delineated in atherogenesis. Active immunization using β2-GPI as antigen enhanced lesion formation and inflammation in atherosclerotic plaques [Afek et al. 1999; Dunoyer-Geindre et al. 2007; George et al. 1998a].
Although anti-CD3 monoclonal antibody is not an atherosclerosis-related antigen, oral administration of low-dose anti-CD3 antibody is known to induce tolerance by eliciting regulatory T cells and anti-inflammatory cytokines [da Cunha and Weiner, 2012]. Sasaki and colleagues reported that such a strategy indeed reduced atherosclerosis with induction of CD4+CD25+FoxP3+ regulatory T cells and anti-inflammatory cytokine TGFβ mediated such an effect in apoE (–/–) mice [Sasaki et al. 2009].
Active immunization with dendritic cells primed with atherosclerosis-related antigens
DCs are ‘nature’s adjuvants’ that can process and deliver antigens to hosts to elicit immune responses [Banchereau and Palucka, 2005; Palucka and Banchereau, 2012]. This approach has been widely used in the field of cancer research and is now being adopted in atherosclerosis research. Dr Kuiper and his group immunized LDLR(–/–) mice with DCs matured with lipopolysaccharide and primed with copper oxLDL and demonstrated reduced carotid artery lesions induced by perivascular collar placement compared with controls [Habets et al. 2010]. Additionally this group transfected DCs with Foxp3 encoding mRNA and injected these DCs into LDLR(–/–) mice and demonstrated that this DC-based immunization strategy resulted in a decrease in FoxP3+ regulatory T cells and an increase in atherosclerotic lesions in the aortic root [van Es et al. 2009]
Conclusion
From a global healthcare point of view, it is extremely appealing to develop atherosclerosis vaccines to prevent and/or treat atherosclerotic cardiovascular diseases. Many different types of antigens have been tested and shown to have great potential to be incorporated into vaccine formulations to reduce atherosclerosis. We and other investigators in this field have accumulated encouraging preclinical data, especially with LDL-related antigens. However, this is only the beginning of the endeavor to advance such knowledge from the preclinical area to clinical application. While advancing this concept to the human arena, many questions, such as vaccine safety and stability, efficacy endpoints, optimal schedule of vaccination regimens and durability of effects, need to be answered in future clinical trials. To do so this requires extensive collaborations among academic investigators, government agencies and the pharmaceutical industry. This will be a costly and long-term task but the effort is worthwhile if it succeeds.
Footnotes
Funding
This work was supported by a research grant from Cardiovax to Cedars-Sinai Medical Center in support of projects related to vaccine research. Additional support from the Heart Foundation and Speilberg Cardiovascular Research Fund are also acknowledged.
Conflict of interest statement
KYC and PKS are coinventors, along with Dr Jan Nilsson, on patents for immune-modulation therapies for atherosclerosis.