
Abstract
The European Society of Gastrointestinal Endoscopy (ESGE) has developed performance measures and established a framework for quality assessment for gastrointestinal endoscopy in Europe. Most national societies actively undertake initiatives to implement and explicitly endorse these quality indicators. Given this, the ESGE proposes that, at a national level, strong leadership should exist to disseminate and implement quality parameters. Thus, understanding the potential barriers that may vary locally is of paramount importance. The ESGE suggests that each national society should prioritise quality and standards of care in gastrointestinal endoscopy in their activities and should survey/understand which measures are a local priority to their members and make measuring quality intrinsic to daily endoscopy practice.
Keywords
Introduction
Five years ago, the European Society of Gastrointestinal Endoscopy (ESGE) and United European Gastroenterology (UEG) initiated the ESGE quality improvement committee (QIC). The aims of this project were: (a) to improve the global quality of gastrointestinal endoscopy in Europe and to deliver a patient-centred service in the field of endoscopy; (b) to promote a unifying theme of quality in endoscopy within different activities of the societies; (c) to create a clear quality improvement framework; and (d) to assist all endoscopy units and endoscopists in achieving these standards. 1
From 2015 to 2019, the ESGE developed performance measures that allow the assessment of the overall quality of endoscopy in Europe within the various aspects of endoscopy, including the endoscopy service itself.2–11 During every UEG week and ESGE meeting over the past 4 years, the theme of quality was further addressed, and the work of the different working groups was explained to the members and attendees. Finally, the framework for quality assessment and improvement was established and the bar was set. Now it is time for dissemination and implementation of these quality indicators. There are several barriers preventing the immediate adoption of performance measures in daily routine endoscopy, including lack of motivation, resources and/or leadership. Such barriers may be successfully overcome by a directed and thoughtful dissemination of the performance measures, as well as by the use of educational or technological interventions.
The aim of this position statement by the ESGE and UEG is to address those barriers that may prevent acceptance and implementation of performance measures in our endoscopy centres and to suggest possible interventions to overcome such barriers.
Methods
This position statement is based on expert opinion owing to the of the lack of evidence-based data on the topic of dissemination of performance measures. To address the interest in quality in endoscopy and the possible barriers to implementation, the ESGE conducted two surveys among its 49 member societies in 2017 and again in 2019. Responses were received from 32 member societies (27 European and five non-European). This position statement addresses both possible barriers to the adoption of performance measures and interventions to overcome these barriers.
Acceptance of quality assessment and barriers to implementation
RECOMMENDATION
Endoscopy societies should take a leading role by endorsing, adapting, translating (if deemed necessary), and assisting local health authorities in the implementation of ESGE performance measures.
According to ESGE surveys, 75% of ESGE member societies explicitly promote performance measures and have actively undertaken initiatives to implement the endoscopy performance measures. There was, however, a clear discrepancy between promotion and explicit endorsement by member societies. Historically, the interest in quality in endoscopy was driven by the quality of colonoscopy because of its significant effect on patient outcomes. 12 Despite this, the endorsement for lower gastrointestinal performance measures in 2019 was only 40% (Figure 1). Obviously, endorsement is a process that requires more discussion with individual members and often translation or adaptation to the specific local situation in a country.
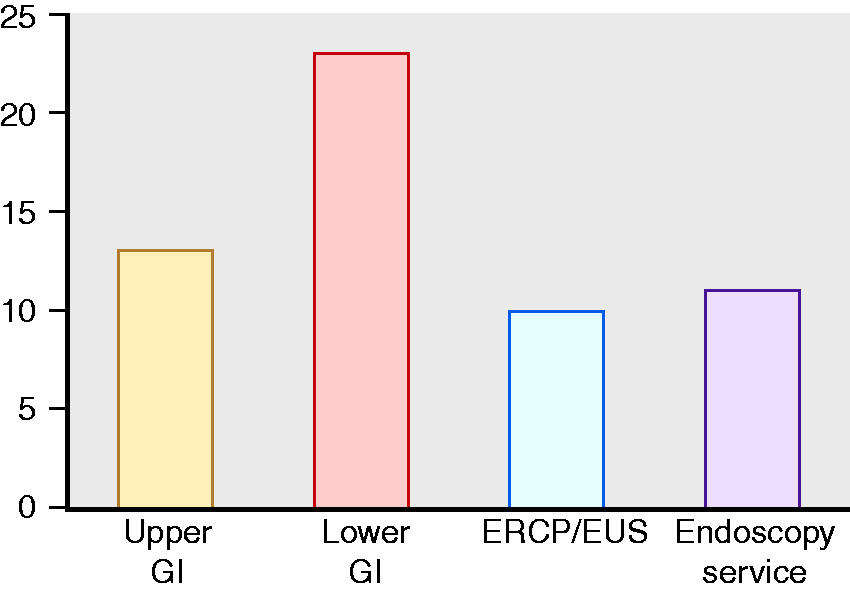
Percentage of National Societies endorsing each performance measure. GI: gastrointestinal; ERCP: endoscopic retrograde cholangiopancreatography; EUS: endoscopic ultrasound.
We found that there is a striking difference between the engagement and promotion of quality measures by national endoscopy societies and the awareness of such measures by national health authorities. In only a quarter of the countries are national health authorities aware of the performance measures in endoscopy and the explicit monitoring of performance required. It can be anticipated, however, that in the coming years national health authorities will become more aware of performance measures and will include them directly into stringent regulations.
Barriers for implementation
RECOMMENDATION
Barriers against performance measure implementation should be locally identified and classified into specific categories.
To facilitate the dissemination and implementation of endoscopy performance measures, it is important to identify potential barriers. In our surveys, we asked the national societies to identify such possible hurdles. These can be divided into three categories.
Resistance to change
The first identified barrier concerns the personal motivational level of the endoscopist. In the 2019 ESGE survey, representatives of the national societies reported a lack of enthusiasm and a resistance to change by local practitioners. In addition, some endoscopists feel they are too busy to implement all the performance measures and prefer to continue their endoscopy practice as it is. There is nothing more difficult to plan, more doubtful of success, nor more dangerous to manage than the creation of a new system. For the initiators have the enmity of all who would profit by the preservation of the old institutions and merely lukewarm defenders in those who would gain by the new one. Machiavelli N. The Prince; 1532. Translated by Vincent ERP. New York, NY: New American Library, 1952
Even now, five centuries later, any change in practice will meet resistance.
Lack of/misconceptions of regulation
A possible reason for practitioner resistance lies in the fact that implementation of performance measures is perceived by many as an administrative burden in an already overly busy daily practice. In addition, there is a fear that implementation of performance measures will come at an additional cost (e.g. computer software packages or payment for administrative support) and that it may prolong endoscopy procedure times. The lack of mandatory regulation by national health authorities and the perceived belief of associated increased costs fail to incentivise endoscopists to speed up the process of quality assessment.
In addition, the adoption of performance measures is generally considered to be an intervention aimed to punish under-performing endoscopists. Instead, performance measure adoption should be considered as a continuous incentive to improve endoscopists’ performance by the offer of retraining and other educational interventions.
Practicality of measuring performance measures
The construct of some of the performance measures is quite complex. To calculate performance measures adequately, inclusion and exclusion criteria need to be considered, or one has to count and indicate how many pictures were taken and what the location was. For instance, accurate photodocumentation of anatomical landmarks and abnormal endoscopic findings is a key performance measure for upper gastrointestinal endoscopy. This seems quite straightforward but, in order to audit this, all pictures and anatomical landmarks must be entered into an electronic report or must be checked image by image. 2 In most endoscopy units, a proper information technology system to assist quality assessment is lacking. Even if an electronic reporting system is used, these often lack uniformity or standardised terminology and allow free-text input that compromises automated performance measure extraction. 13
In the ESGE member society survey, only in 15% of the countries did more than 90% of endoscopy services use an electronic reporting system. In one out of three countries this coverage was less than 10% (Figure 2).
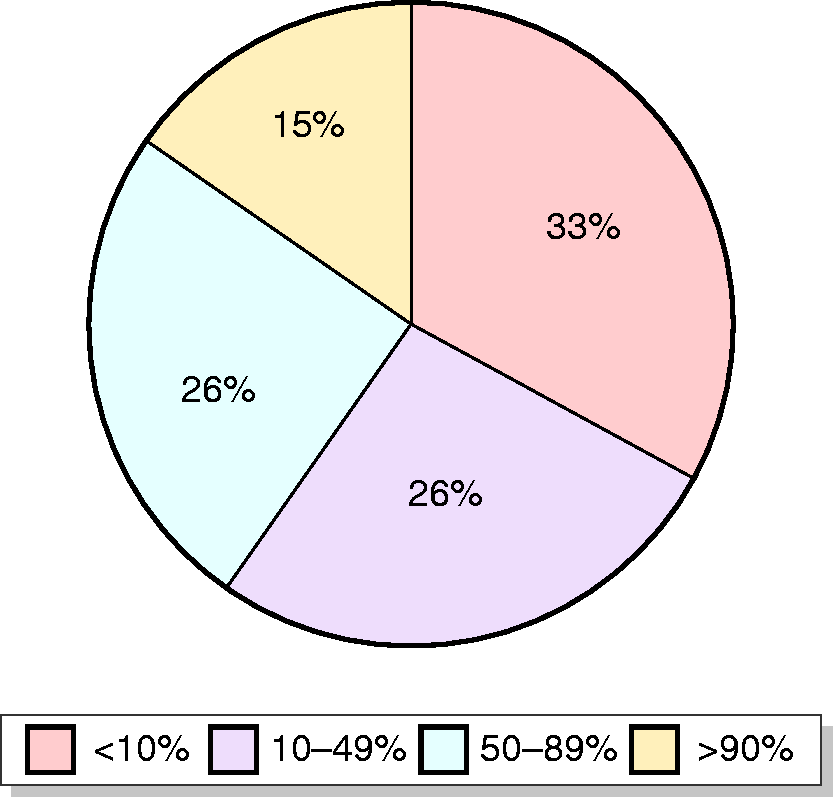
Levels of coverage for electronic reporting systems among different countries.
How to overcome these barriers
Prioritise performance measures within your local society
RECOMMENDATION
Endoscopy societies should prioritise a set of performance measures, taking into consideration local factors, such as disease prevalence, performance measure relevance and the feasibility of performance measure implementation.
Taking available evidence into consideration, the current set of performance measures is scientifically developed thorough a Delphi process. 14 Every working group tried to reduce the number of performance measures to a minimum to keep the process of auditing realistic and feasible. The ESGE wants to emphasise, however, that for many performance measures there is no high-level evidence, and that performance measures may not always be applicable or maybe of less importance in a specific country or endoscopy service. For instance, performance measures relating to Barrett’s oesophagus may be more important in western Europe, whereas the follow-up of gastric intestinal metaplasia may be of more importance in southern and eastern Europe. Therefore, the ESGE encourages national societies to initiate discussion with their members to select those performance measures that are perceived to be most locally important and/or relevant.
As an example, the ESGE survey assessed the priorities of member societies with regard to the 11 performance measures for upper gastrointestinal endoscopy quality assessment. 2 Surprisingly, three minor performance measures that were classified as possibly less important/more challenging by the upper gastrointestinal QIC made it into the top six (Table 1). The ESGE strongly encourages national societies to perform a similar survey for all performance measures among their members. This could be done at a national meeting using an online voting system during a session dedicated to quality in endoscopy. For example, the Belgian Society of Gastrointestinal Endoscopy did this at their annual meeting in 2019. By explaining the different performance measures and the reasons or evidence behind them, the national societies can play an essential role in overcoming the resistance to change and gaining acceptance of the concept of measuring quality in gastrointestinal endoscopy.
Top six priorities for upper gastrointestinal quality indicators according to the 2019 ESGE member society survey.
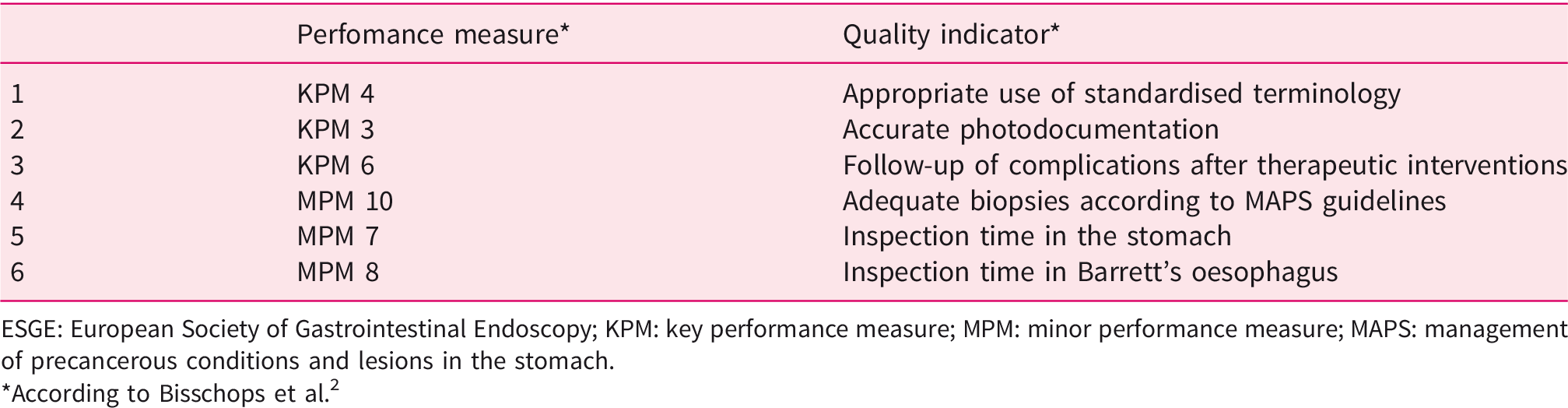
ESGE: European Society of Gastrointestinal Endoscopy; KPM: key performance measure; MPM: minor performance measure; MAPS: management of precancerous conditions and lesions in the stomach.
*According to Bisschops et al. 2
Disseminate the performance measures through your national society
RECOMMENDATION
Educational and scientific interventions should be implemented or endorsed by endoscopy societies to disseminate performance measures. The use of new or existing electronic databases to audit performance measures, such as the ESGE Quality Check App, is also desirable to facilitate performance measure assessment.
Thus far, many national societies have undertaken initiatives for the dissemination and implementation of performance measures, and the evidence below shows that this pays off and improves the overall quality of endoscopy. In an optimal scenario, there is a three-way synergy between national societies, national health authorities and individual members. However, because the health authorities in many countries are not aware of the quality in endoscopy paradigm, this synergy is often lacking. Nonetheless, there are numerous examples in which national societies have taken the lead.
The role of the national societies is in fact two-fold: first, they raise the awareness of quality in endoscopy by assessing problems or lack of quality and by running individual projects, and thereby they subsequently improve quality. Second, this often leads to publications that further substantiate the evidence for certain performance measures. Many quality improvement initiatives are currently undertaken for promoting awareness of quality in endoscopy through dedicated sessions or meetings organised nationally.
For instance, in Italy, a wide variation in cecal intubation rate and adenoma detection rate (ADR) was identified and it was found that, in many instances, split-dose bowel preparation was not used. A subsequent Italian randomised controlled trial was conducted and showed a clear increase in ADR when split-dose bowel preparation was used. 15 The direct involvement of different endoscopy services in the identification of a problem, and subsequently provision of the evidence that simple measures do actually improve quality should convince even those endoscopists most resistant to change.
In Russia, two projects were initiated for dissemination of the upper gastrointestinal and lower gastrointestinal performance measures, STANDUP and QUACOL. They first assessed the quality of colonoscopy and found it to be suboptimal. 16 By organising more than 50 dedicated workshops and 18 educational events all over the country, they significantly improved the ADR from 18% to 25.8% and cecal intubation rates from 86% to 96.2%.
These types of initiatives raise awareness among endoscopists that simple measures that do not cost anything can improve the quality of endoscopy. Most recently, two interesting reports from Spain and Portugal showed a significant improvement in upper gastrointestinal endoscopy performance following simple quality improvement interventions.17,18 They showed a statistically significant improvement in the use of photodocumentation, the use of adequate standardised endoscopic terminology and the application of correct biopsy protocols.
The involvement of local governmental regulatory agencies usually stimulates quality measurement, often because of the possible financial repercussions and consequences if quality standards are not met. Nonetheless, the involvement of national health authorities may also catalyse quality initiatives without being mandatory. For instance, in 2007, the Austrian Society of Gastroenterology and Hepatology initiated the voluntary reporting of a minimum number of colonoscopies and polypectomies per year by way of an electronic reporting system. They are backed up by the Austrian Federation of Statutory Insurance institutions and Austrian Cancer Aid. Although providing the data means double data entry for the endoscopist and despite being voluntary, there is a high participation rate because the endoscopy units receive a quality label from the Austrian Society of Gastroenterology and Hepatology if they perform well. This has resulted in a significant improvement in quality in colonoscopy over time in Austria. 19
Start measuring quality indicators: the ESGE quality check app
The degree to which auditing and measuring of quality indicators is achieved depends on the level of development/sophistication of the endoscopy report. Three levels of development can be identified (Figure 3). As shown in the results of the ESGE survey, there is wide variability in endoscopy procedure reporting.
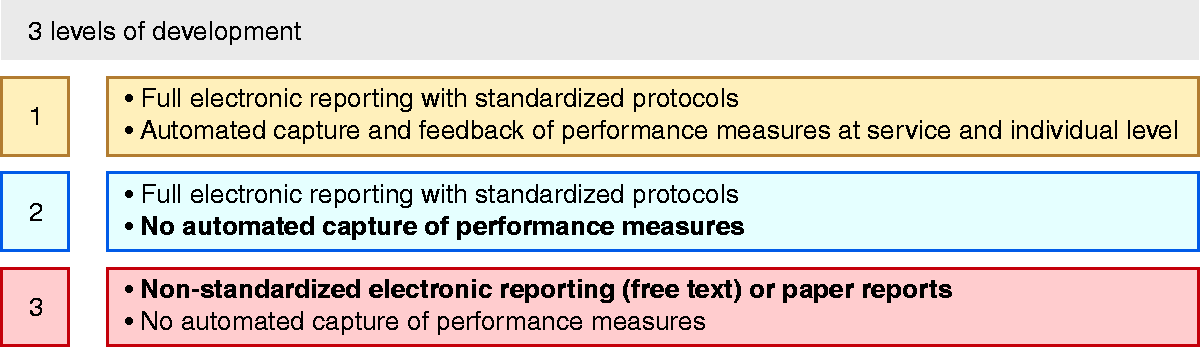
The different levels of development for gastrointestinal endoscopy reporting.
In an ideal world, a full electronic reporting system with standardised protocols would be available. 20 Such a reporting system would allow automated capture and feedback of performance measures at an endoscopy service and individual level, virtually in real time.
Because of the involvement of national health authorities to regulate quality in endoscopy, the implementation and widespread use of such electronic reporting systems in endoscopy will undoubtedly be accelerated. This is the case with the National Health Service (NHS) in the United Kingdom, which introduced bowel cancer screening in 2006, with a strong emphasis on quality monitoring. 21 Recently, the British Society of Gastroenterology, Association of Upper Gastrointestinal Surgeons and the Association of Coloproctology of Great Britain and Ireland initiated the national endoscopy database project, under the oversight of the joint advisory group on gastrointestinal endoscopy. They negotiated with different companies to implement and unify standardised endoscopy reporting systems as a prerequisite for inclusion in the project. As a consequence, they now have an electronic reporting system that allows participating endoscopy centres to monitor quality and patient outcomes directly, without double data entry, directly from the patient’s endoscopy report. 22
Even without the explicit influence of national health authorities, national gastroenterology/endoscopy societies can achieve similar effects and obtain standardised reporting systems from software companies. For instance, the Portuguese Society of Digestive Endoscopy went through a similar process to unify endoscopy reporting in negotiation with software providers. Recently, the Dutch bowel cancer screening programme reported how they developed and deployed a quality register to collect uniform data. This was done in cooperation with commercial endoscopy reporting systems and a national histopathology database to extract data from core hospital resources or histology databases without manual interference of the healthcare providers, again avoiding double data entry. 23
However, in most cases, the endoscopist will have an electronic endoscopy reporting system with or without standardised reporting protocols or will still be using paper reports or free-text digital reports. In those cases, automated capture is impossible. Nonetheless, it is possible to audit these services as well. Indeed, measuring approximately 300 gastroscopies and 300 colonoscopies per audit would allow for an adequate snapshot of the quality of those procedures (95% confidence interval 0.87–0.93). The main challenge that remains is to take all inclusion and exclusion criteria into consideration during an audit, which in fact may be tedious if done manually. In order to facilitate this, the ESGE has developed a quality check app that allows retrospective audit of endoscopy procedures by entering consecutive cases. The ESGE quality check app can be downloaded and used on all mobile or desktop platforms. It will guide the endoscopist through different questions to take all exclusion criteria into consideration and will provide the appropriate questions in relation to the pathology that is found. It is estimated that it will take 2 minutes per case entry so, with 3–4 days of administrative work per year, hospital management could support quality assessment and provide a quality snapshot of its colonoscopy and gastroscopy services, without any significant financial investment.
The future role of the ESGE and UEG
The ESGE will support and provide the ESGE Quality Check App.
Individuals who are interested in obtaining and using the Quality Check App can contact the ESGE secretariat to ask for access (
Through the ESGE travelling endoscopy programme, the ESGE can provide dedicated sessions on quality in endoscopy within locally organised meetings. The members of the ESGE QIC are ambassadors of quality in endoscopy and are already undertaking personal initiatives within their home countries to implement quality measurement. The ESGE QIC members also keep up to date with emerging evidence of quality in endoscopy, in order to revise the performance measures in the future. In addition, the ESGE QIC will analyse data from the quality check app to build a benchmark of quality throughout Europe for other endoscopy centres and to assess performance measures that may turn out to be less relevant.
It will also be important to address quality in gastrointestinal endoscopy at the European political level. For this purpose, the ESGE and UEG will join forces through public advocacy initiatives; for example, the public affairs committee of UEG and the ESGE public advocacy committee, to prioritise quality in endoscopy and improve patient outcomes throughout Europe.
Conclusion
Developing quality indicators for gastrointestinal endoscopy is a work in progress, with new insights that become apparent every year. The ESGE and UEG have developed a set of performance measures for all fields of gastrointestinal endoscopy. Although there are still hurdles to overcome, many initiatives throughout Europe have facilitated and promoted quality assessment and put the important issue of quality in gastrointestinal endoscopy on the map. The ESGE strongly recommends the dissemination and implementation of the quality indicators, as well as the monitoring of these indicators at the local level. This will help to provide the best possible gastrointestinal endoscopy care for our patients throughout Europe.
This quality of care project may very well serve as a framework to identify quality indicators in other areas of digestive health and help to initiate further quality of care projects in the field of digestive health. Such future initiatives to implement quality of care evaluation into daily practice will hopefully improve the overall care of patients with digestive diseases.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: RB is supported by the Research Foundation–Flanders (FWO) and has provided consultancy and received speaker’s fees and research support from Norgine, Pentax Europe and Fujifilm (2017 to present). MDR has received research grants from Olympus and Fujifilm (2018 to present). MFK has provided speaking, teaching and consultancy services to Olympus (2017 to present), and speaking and teaching services to Fujifilm, from whom he also has equipment on loan (2019 to present). CS has provided consultancy to Medtronic (2017–2020). MA, AD, DD, PF, IMG, CH, WK, HM, TP, MDR and AV declare that they have no conflicts of interest.
Ethics approval
▪
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.