
Abstract
Background
Superficial oesophageal adenocarcinoma can be resected endoscopically, but data to define a curative endoscopic resection are scarce.
Objective
Our study aimed to assess the risk of lymph node metastasis depending on the depth of invasion and histological features of oesophageal adenocarcinoma.
Methods
We retrospectively included all patients undergoing an endoscopic resection for T1 oesophageal adenocarcinoma among seven expert centres in France in 2004–2016. Mural invasion was defined as either intramucosal or submucosal tumours; the latter were further divided into superficial submucosal (≤1000 µm) and deep submucosal (>1000 µm). Absence or presence of lymphovascular invasion and/or poorly differentiated cancer (G3) defined a low-risk or a high-risk tumour, respectively. For submucosal tumours, invasion depth and histological features were systematically confirmed after a second dedicated histological assessment (new 2-mm thick slices) performed by a second pathologist. Occurrence of lymph node metastasis was recorded during the follow-up from histological or PET CT reports when an invasive procedure was not possible.
Results
In total, 188 superficial oesophageal adenocarcinomas were included with a median follow-up of 34 months. No lymph node metastases occurred for intramucosal oesophageal adenocarcinomas (n = 135) even with high-risk histological features. Among submucosal oesophageal adenocarcinomas, only tumours with lymphovascular invasion or poorly differentiated cancer or with a depth of invasion >1000 µm developed lymph node metastasis tumours (n = 10/53; 18.9%; hazard ratio 12.04). No metastatic evolution occurred under a 1000-µm threshold for all low-risk tumours (0/25), nor under 1200 µm (0/1) and three over this threshold (3/13, 23.1%).
Conclusion
Intramucosal and low-risk tumours with shallow submucosal invasion up to 1200 µm were not associated with lymph node metastasis during follow-up. In case of high-risk features and/or deep submucosal invasion, endoscopic resections are not sufficient to eliminate the risk of lymph node metastasis, and surgical oesophagectomy should be carried out. These results must be confirmed by larger prospective series.
Keywords
Key summary
Superficial oesophageal adenocarcinoma (OAC) can be resected endoscopically. Data to define a curative endoscopic resection with a low lymph node metastasis (LNM) risk are scarce especially for tumours invading the submucosa. Curative endoscopic resections have been reported in selected OAC invading the first 500 µm of the submucosa, but surgical series showed an LNM risk ranging from 0 to 50%, making endoscopic resection a questionable curative treatment. High-risk histological features were not associated with LNM in intramucosal tumours. LNM occurred only for tumours invading the submucosa with a depth ≥1200 µm or with high-risk histological features regardless of the depth of invasion. Endoscopic resection may be a valid and curative therapeutic option for all intramucosal tumours and for submucosal oesophageal adenocarcinoma with an invasion depth ≤1000 µm and low-risk histological features.
Introduction
The incidence of oesophageal adenocarcinoma (OAC) arising from Barrett’s oesophagus (BO) has increased dramatically over the last three decades in Western countries. 1
Available data for the management of BO and superficial oesophageal adenocarcinoma (OAC) are scarce. Oesophagectomy has been the standard of care in treating these lesions for many years as it treats not only the oesophageal neoplastic lesion but also the potential lymph node metastasis (LNM) and the remaining BO. However, oesophagectomy is associated with high mortality and morbidity.2–5
Endoscopic resection (ER) offers an alternative to en bloc oesophagectomy for superficial OAC. Indeed, the presence of LNM is strongly correlated to histological features and to the depth of the tumour invasion. 6 Several histological features impact the risk of LNM such as lymphovascular invasion (LVI) poor tumour differentiation. 7 , 8 As a consequence, a low-risk (LR) pattern could be associated with a reduced risk of LNM and could then be treated solely by endoscopic means. 9 In superficial OAC limited to the mucosa (T1a OAC) the risk of LNM is close to zero and therefore ER has become the standard of care in treating these lesions. For tumours spreading through the submucosa, surgical series showed a LNM risk ranging from 0 to 50% thus making ER a questionable curative treatment. 5 ,10–16 Nevertheless, recent endoscopic studies have reported curative ERs in selected T1b OAC invading only the first 500 µm of the submucosa. 17 , 18 However, ER of superficial OAC is still controversial for submucosal tumours.
In this study, we aimed to assess the LNM risk for intramucosal and submucosal OAC resected endoscopically, across seven endoscopic centres in France according to histological features and the depth of tumour invasion.
Materials and methods
Study design
We conducted a multicentric retrospective study involving seven French centres. The study was approved by the ethical review board of Lyon University Hospital (number CE: N° 18-05) on 11 December 2018.
The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in an a priori approval by the institution's human research committee. Considering the retrospective aspect of this study, formal written consent was not required. All resections of superficial OAC fulfilling inclusion criteria from November 2004 to November 2016 were included either using the pathology recording software in three expert centres (Edouard Herriot Hospital, Lyon; Dupuytren Hospital, Limoges; Cochin Hospital, Paris) or using local systematic databases in the other centres (Hôpital Européen Georges Pompidou, Paris; Liège University Hospital; Jean Mermoz Private Hospital, Lyon; Croix-Rousse Hospital, Lyon). Participating centres included five teaching hospitals and two non-teaching hospitals. Data regarding endoscopic resections, follow-up data and the occurrence of LNM were retrospectively retrieved from the patients' records.
Patients
All patients undergoing ER with a curative intent in the study period for superficial OAC developed on BO were included if they had a minimal follow-up of 12 months after ER or if they were diagnosed for LNM or underwent curative surgery during the first year after ER. Superficial OAC was defined by a T1 adenocarcinoma (limited to the mucosa or submucosa) diagnosed by an expert in digestive pathology and arising from BO. Adenocarcinoma of the cardia were included only if they were associated with BO tissue and presented histological oesophageal features.
Patients were excluded in case of proven distant metastasis during the initial work up, an OAC infiltrating beyond the submucosa and neoadjuvant or adjuvant radiation therapy or chemotherapy or when surgery was performed as a first line treatment.
Study outcomes
Primary outcome was defined by the occurrence of LNM during follow-up depending on histological features and the depth of tumour invasion. Secondary outcomes included: (a) safety of the endoscopic resection procedures; (b) local and distant cancer recurrences following curative endoscopic resections; and (c) overall mortality.
Endoscopic resection characteristics
All ER were performed under general anaesthesia by endoscopic mucosal resection (EMR) or endoscopic submucosal dissection (ESD). For some patients, the remaining Barrett’s tissue, irrespective of histology, was removed using metachronous ER, radiofrequency (RFA) or argon plasma coagulation (APC or hybrid APC). All the endoscopic procedures were performed by physicians who were very experienced in EMR, ESD and therapeutic endoscopy.
Histological assessment
The staging was based on the pathological examination by a gastrointestinal expert pathologist of endoscopically resected specimens and according to the 7th edition of the UICC TNM classification. 19 Intramucosal tumours (pT1a) were further distinguished between tumours invading the oesophageal epithelium or the lamina propria (m1/m2), and tumours invading the muscularis mucosae (m3). Submucosal tumours (pT1b) were divided between tumours with a shallow submucosal invasion ranging from 1 to 500 µm (according to the European Society of Gastrointestinal Endoscopy (ESGE) guidelines 18 ), named sm1, and tumours invading beyond this threshold in the submucosa (deep sm). We chose to further divide the latter into sm2 tumours with an invasion depth ranging from 501 µm to 1000 µm included, and sm3 tumours with an invasion depth beyond 1000 µm. For submucosal tumours, invasion depth and histological features were systematically confirmed after a second dedicated histological assessment (new 2-mm thick slices) performed by a pathologist specialised in the field of gastrointestinal pathology, according to French pathology standards. If the muscularis mucosae was duplicated, the submucosal tumour invasion was measured under the deepest layer of the muscularis mucosae. Additionally, high-risk (HR) features and the LNM status in surgical specimens were recorded specifically. A tumour was considered HR if it presented either LVI, a poor differentiation or both, and LR if it presented neither.
After EMR or ESD, the resection was considered R0 if the lateral and vertical margins were free of adenocarcinoma. In case of an R1 endoscopic resection followed by surgical resection with remaining neoplastic tissue on the surgical specimen, the deepest tumour invasion of the two specimens was recorded to determine the actual T stage of the tumour and the less favourable histological features were considered for the final analysis. No additional cuts were made for surgical specimens.
Patient management and follow-up after ER
Follow-up endoscopies were performed every 3 months after ER during the first year, to exclude any remaining neoplastic tissue, and to appreciate the extent of the remaining BO tissue as recommended by the ESGE guidelines. 17 During the follow-up, CT scans, PET scans or endoscopic ultrasound (EUS) were used as a routine examination to evaluate LNM occurrence. As this study was retrospective and the data retrospectively collected, the frequency of these tests was not defined beforehand, and therefore the need for CT scans or EUS was left to the discretion of the referring gastroenterologist according to national guidelines that recommend biannual CT scans or EUS, and PET scan only on suspicion of relapse.
Data collection
Patient’s symptoms, endoscopic procedure and histopathological report were collected at the time of the first endoscopic procedure. Follow-up data were retrieved from the medical files including CT scans, EUS, new endoscopic procedures, surgical procedures and histological findings. Follow-up time was calculated from the curative endoscopic procedure to the last investigation, either endoscopic or radiological, or to the curative surgery when performed.
LNM diagnosis
In case of surgical treatment or fine-needle aspiration biopsy, the lymph node status was determined on the pathology report. When the patient was deemed unfit for invasive procedure or chemotherapy, LNM was diagnosed using a non-invasive procedure (PET scan). In these latter cases, diagnosis of LNM was retained if mentioned on reports of an oncology multidisciplinary team meeting.
Statistical analysis
The interquartile range (IQR) and median were used to describe data with a skewed distribution. The primary outcome was assessed using a Kaplan–Meier survival curve with calculation of the hazard ratio (Mantel–Haenszel method) comparing patients with HR tumours and/or >1000 µm of invasion to patients with LR tumours and ≤1000 µm of invasion. All p-values were two-sided and regarded as significant if under 0.05. Statistical analysis was performed using GraphPad Prism (v. 6.05 for MAC OS, GraphPad Software, La Jolla California, USA, www.graphpad.com).
Results
Study population
From 23 November 2004 to 28 November 2016, 188 patients were included from the seven centres of the study (Figure 1). The median follow-up for all intramucosal tumours was 35 months (IQR: 24–61). Considering only the submucosal tumours, the median follow-up was 30 months (IQR: 22–66). Patients’ characteristics and treatment are described in Table 1. All patients that underwent surgery as a complementary treatment after an initial ER had an R0 resection. One hundred and thirty-five tumours were classified as intramucosal (60 m1/2 tumours, 75 m3) and 53 were submucosal (16 sm1, 19 sm2, 18 sm3). High-risk histological features were found in 24 tumours (12.7%): 9 with intramucosal tumours (9/135, 6.4%; 5 LVI, 5 G3 differentiation, one patient had both) and 15 with submucosal tumours (15/53, 28.5%), including 5 sm1 (5/16, 31.3%, 4 G3 and 1 LVI), 5 sm2 (5/19, 26.3%, 2 LVI, 3 G3) and 5 sm3 tumours (5/18: 27.8%, 5 LVI, 1 G3, one patient had both LVI and a G3 differentiation).
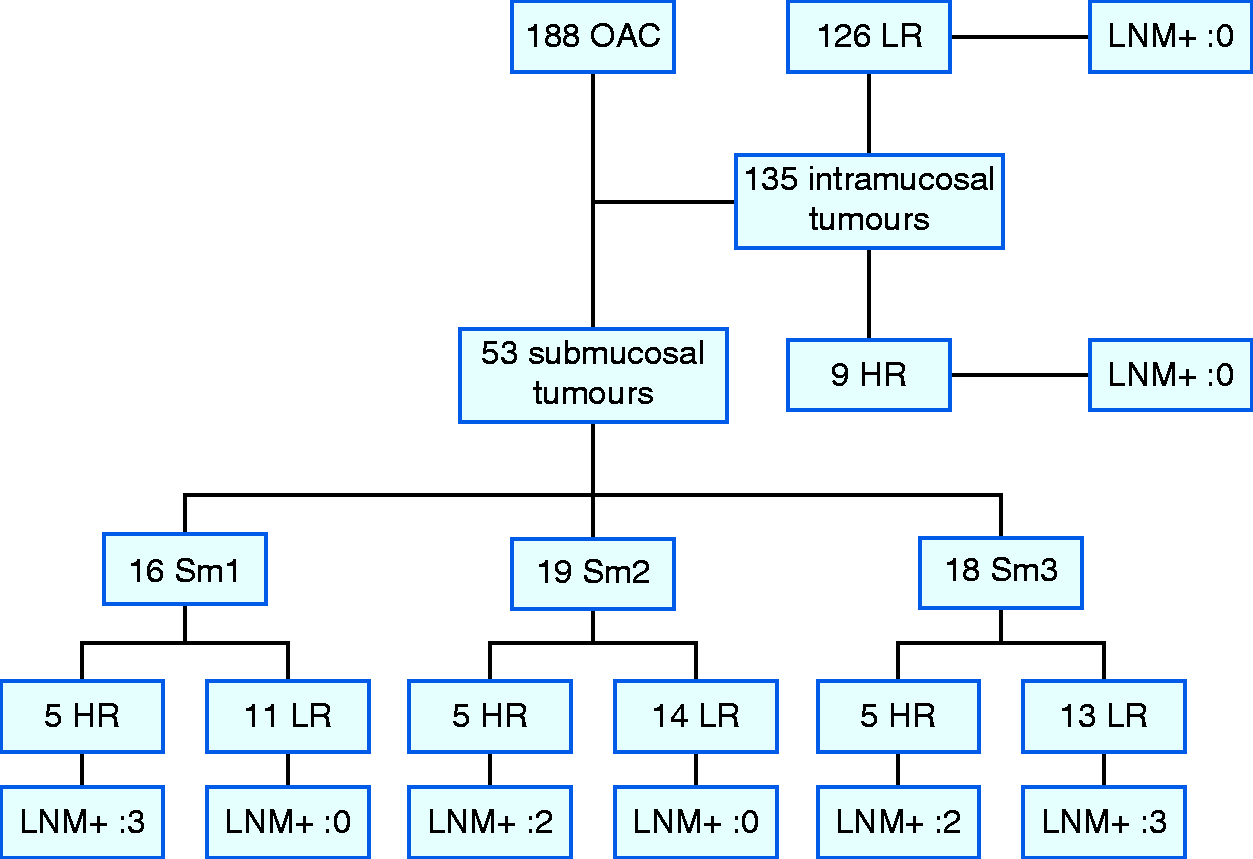
Study flowchart. HR: high risk; LNM: lymph node metastasis; LR: low risk; sm1: depth of invasion ≤500 µm; sm2: depth of invasion between 500 and 1000 µm; sm3: depth of invasion >1000 µm.
Baseline characteristics of patients and procedures.
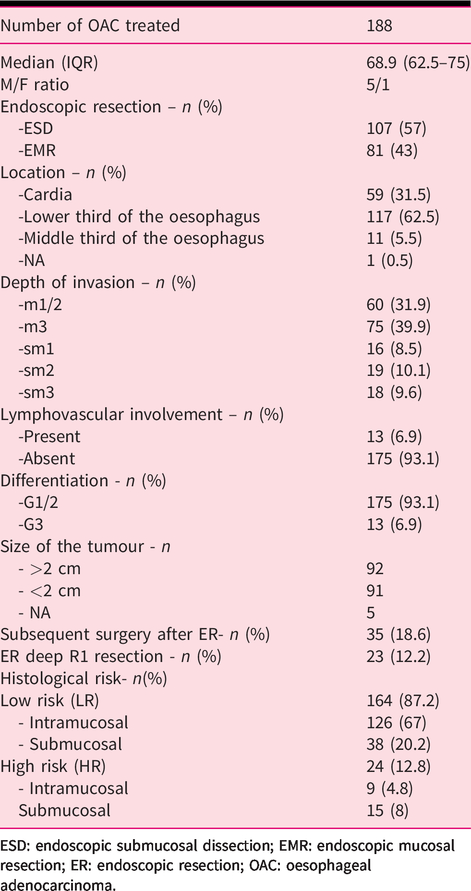
ESD: endoscopic submucosal dissection; EMR: endoscopic mucosal resection; ER: endoscopic resection; OAC: oesophageal adenocarcinoma.
Considering submucosal OAC, the infiltration depth of sm1 adenocarcinomas ranged from 10 to 499 µm within the submucosa with a mean of 285 µm. The infiltration depth of deep submucosal adenocarcinomas (n = 37) ranged from 550 µm to 3200 µm with a mean of 1231 µm, and in this subgroup sm2 and sm3 tumours had a mean invasion depth of 777 µm and 1711 µm, respectively.
Primary outcome: lymph node metastasis
Ten patients presented LNM (10/188; 5.3%; Table 2). Four LNMs were identified on the pathology report of a subsequent surgical specimen after ER, and 6 LNMs were diagnosed during the follow-up by either fine needle aspiration (FNA) performed by EUS (n = 4) or on a PET scan (n = 2), showing intrathoracic hypermetabolic lymph nodes.
Characteristics of oesophageal adenocarcinoma (OAC) with lymph node metastasis (LNM) diagnosed during follow-up.
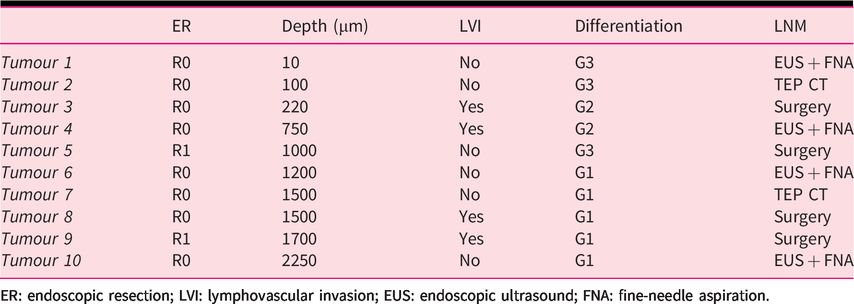
ER: endoscopic resection; LVI: lymphovascular invasion; EUS: endoscopic ultrasound; FNA: fine-needle aspiration.
No LNMs were discovered during the follow-up of intramucosal tumours (0/135) even when the tumours presented high-risk features (0/9; Table 3). LR sm1 tumours were not associated with LNM (0/11, 0%), neither were LR sm2 tumours (0/14). However, 60% of HR sm1 tumours developed LNM (3/5; Table 2). No LNM occurred in LR sm tumours with an invasion depth ≤1200 µm (0/26; 11 sm1, 14 sm2, 1 sm3 between 1000 and 1200 µm). Patients with LR tumours with a depth of invasion ≤1000 µm had a lower risk of LNM compared to patients with HR tumours or a depth of invasion >1000 µm (hazard ratio: 12.04, 95% CI 3.146 to 46.11; p = 0.0003, Mantel–Haenszel method). Curves of the proportion of LNM free survival in those two groups are presented in Figure 2.
Occurrence of lymph node metastasis (LNM) depending on histological features and invasion depth.
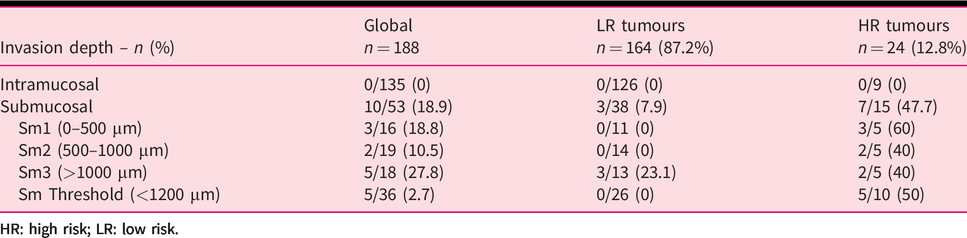
HR: high risk; LR: low risk.
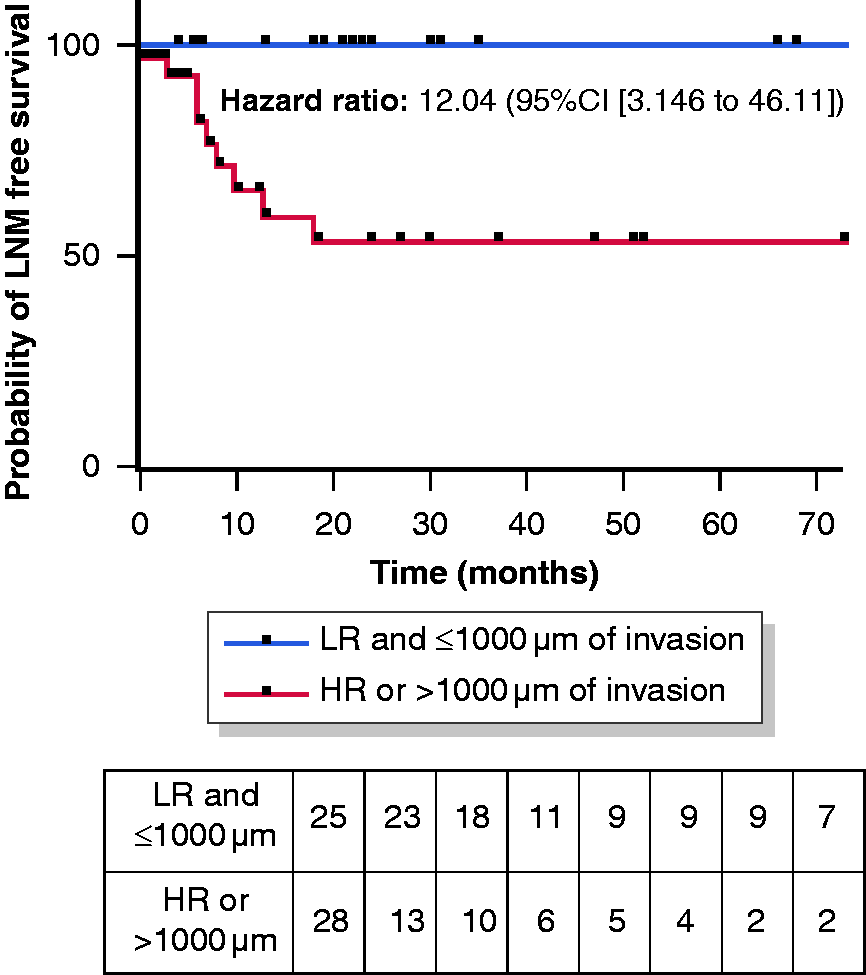
Kaplan–Meier analyses of lymph node metastasis-free survival of the entire population of submucosal oesophageal adenocarcinoma based on depth of invasion and histological features. 95%CI: 95% confidence interval; HR: high risk; LNM: lymph node metastasis; LR: low risk.
Secondary outcomes: adverse events, recurrences and mortality
Eight non-significant adverse events of bleeding during procedures occurred (n = 8/188, 4.2%). One procedure (0.5%) had to be aborted due to excessive bleeding, and an additional delayed ER was performed to successfully eradicate the remaining neoplastic tissue. Delayed bleedings occurred in two patients (1.0%) who had to undergo an additional endoscopic procedure with successful outcomes. Perforations were reported during four procedures (2.1%), and all were managed endoscopically but the resection had to be aborted prematurely in those four cases. Three patients had to undergo a subsequent surgical procedure to remove the remaining neoplastic tissue.
Oesophageal stricture following an ER developed in 20.2% (n = 38) of the patients, and all underwent a successful endoscopic treatment with repeated balloon dilatations.
During follow-up, local metachronous adenocarcinoma was diagnosed in 18 patients (18/188, 9.6%). In all these cases, patients had gone through a surveillance endoscopy negative for cancer after the initial endoscopy. Among these patients, 72.2% (13/18) could be treated successfully with iterative ER and four underwent surgery (22.2%).
Among ER patients, the 30-day mortality rate was 0.5% (1/188; one died of pneumonia during the post ER hospital stay and was positive for LNM). For the full period of follow-up, 27 patients died (14.4%), and among them 8 were considered tumour related (8/188, 4.3%).
Discussion
In our study including 188 oesophageal adenocarcinomas, no LNM occurred after ER of intramucosal OACs, or well differentiated submucosal OACs with an invasion depth ≤1200 µm and no LVI.
The management of intramucosal OAC is relatively consensual since several studies found a very low risk of LNM, ranging from 0 to 1.8%, and an improved overall survival rate in patients treated by endoscopic means compared to surgery.18–22 Pech and colleagues, in one of the largest cohorts of intramucosal OAC treated endoscopically found a 96.3% complete remission rate and a 0.2% tumour-related death rate following ER for intramucosal OAC. 22 However, a significantly higher risk of recurrence and failure of endoscopic treatment was reported in poorly differentiated intramucosal OAC in contradiction to our data where the LNM risk was still non-existent for intramucosal OAC regardless of the histoprognostic features. This might suggest that for all intramucosal tumours, irrespective of the histological features, a curative ER could be used as first line therapy, but a closer and thorough endoscopic surveillance programme following the ER should be undertaken in poorly differentiated intramucosal OACs.
Regarding LR submucosal tumours, no metastasis, nodal or distant, occurred when the invasion depth was beyond 1000 µm, and even 1200 µm, but with the limitation that there was only one patient with an LR tumour between 1000 and 1200 µm. In the current ESGE guidelines, 17 an ER is considered curative when the tumour invasion depth does not exceed 500 µm in the submucosa for LR tumours. In our study, occurrence of LNM for LR tumours with an invasion depth beyond 1200 µm was indeed null. Similarly, Fotis and colleagues described only one LNM in pT1b LR adenocarcinoma under a 1200 µm submucosal invasion depth among 22 LR lesions (4.5%). 23 If we combine data published by Fotis et al. with ours, the LNM risk for LR tumours with an invasion depth beyond 1200 µm is 2% (1/48). Both results are still inferior to the mortality risk of oesophagectomy ranging between 2 and 5% in expert centres and up to 20% in non-expert hospitals, and a morbidity rate reaching 40%.2–5, 10 ,24–26 Thus, our results could suggest that an organ-preserving strategy by endoscopic means could be used to efficiently treat submucosal OAC with favourable pathological features and with an invasion depth in the submucosa ≤1000 µm and maybe even ≤1200 µm. However, these data should be confirmed by larger prospective series.
Several endoscopic studies evaluated the LNM risk for LR OAC with a submucosal invasion. In accordance with our results, Alvarez Herrero et al. found no LNM for LR sm1 tumours. Moreover, in sm2/3 LR tumours no LNMs were reported during a follow-up period of 26 months. 27 Similarly, Manner et al. in a prospective cohort reported only 1 LNM (1/49; 2%) in the LR sm1 subgroup, after ER of a G2 differentiated OAC, 28 whereas others found no LNM in selected LR sm2 (pragmatic definition) OAC. 29
Surgical studies have found a much higher rate of LNM in pT1sm1 OAC, with rates reaching 50%, 6 , 10 , 11 , 14 , 16 , 28 hence suggesting that oesophagectomy should be carried out to treat every OAC invading the upper third of the submucosa. Nevertheless, reported rates of LNM in surgical studies for sm2/3 OAC were also much higher than reported in endoscopic studies reaching 36% for sm2 tumours and 78% for sm3 tumours.9–11, 13 , 14 , 30 , 31 However, most of these studies did not draw a distinction between LR and HR tumours. Furthermore, as surgical resection specimens are usually cut into larger pieces than endoscopic resection specimens (usually every 2–3 mm), the accuracy of the submucosal infiltration measures may not be the same among surgical and endoscopic studies. The deepest tumour invasion point or a single embolus could also easily be missed, resulting in under-staging the tumour. Also, sm1 is defined on esophagectomy specimens by an infiltration of the upper third of the submucosa and does not necessarily match the 500-µm threshold we used in our work.
In our study, patients presenting with tumours exhibiting HR pathological features and invading the submucosa had a high risk of LNM. Data in the literature about HR submucosal tumours are scarce with an LNM rate ranging from 8.7% to 42% on small series. 23 , 32
Regarding the safety of ER, the rate of adverse events is very low, and no deaths were procedure related. Oesophageal stricture following the procedure was the most common complication, but recent techniques to reduce the risk of stenosis were not routinely used at the beginning of the study period.
This work presents many limitations inherent to its retrospective design. First, the frequency of examination to detect LNM was not defined beforehand, and heterogeneity among patients may contribute to the differences observed. However, all centres involved were referral centres in the management of OAC, and patient follow-up was done according to national guidelines. Second, due to limited follow-up for some patients, LNMs may have been missed. However, it has been shown that LNMs after an ER occur within a median of 12 months and metastatic lesions within a median of 16 months. 11 , 35 In our study, the median follow-up was 34 months and patients with a follow-up of less than 12 months with no LNM or curative surgery were excluded to reduce this possible bias.
Third, the number of patients with high-risk lesions was limited both for intramucosal tumours (9/135) and submucosal tumours (19/53), which limited the conclusion that can be drawn from this work.
Our study is in accordance with data from the literature and confirms that intramucosal oesophageal adenocarcinoma with no invasion beyond the muscularis mucosae could be treated solely by endoscopic means regardless of the histological features. For pT1b with shallow infiltration of the submucosa and LR features, the endoscopic approach seems to be a valid option. This work suggests that the curative threshold may be raised from 500 µm to 1000 µm and even possibly 1200 µm. However this must be confirmed by larger prospective studies. Due to the high morbidity and mortality of oesophagectomy, this organ-preserving approach may be proposed after a multidisciplinary discussion, 33 , 34 especially in patients deemed unfit for thoracic surgery but with a thorough follow-up after the ER. For all high-risk tumours invading the submucosa, oesophagectomy, if possible, should remain the standard of care irrespective of the tumour invasion depth as the risk of LNM seems to outweigh the risk of oesophagectomy.
Footnotes
Ethics approval
This study was performed in accordance with the Declaration of Helsinki and was approved by the Ethical committee of Lyon university hospital.
Declaration of Conflicting Interest
The author(s) have no conflicts of interest to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
This study was retrospective without need for informed written consent.