
Abstract
Transjugular intrahepatic portosystemic shunt is a percutaneous radiologic-guided procedure that aims to reduce portal hypertension by creating a shunt between the portal venous system and the hepatic venous system. The most common cause of portal hypertension is liver cirrhosis in Western countries. Two main indications of transjugular intrahepatic portosystemic shunt are validated by randomised controlled studies in patients with cirrhosis and variceal bleeding (salvage transjugular intrahepatic portosystemic shunt, early-transjugular intrahepatic portosystemic shunt or rebleeding despite an optimal secondary prophylaxis) or refractory ascites. Careful selection of the patients is crucial in order to prevent post-transjugular intrahepatic portosystemic shunt complications, including liver failure, post-transjugular intrahepatic portosystemic shunt encephalopathy occurrence and cardiac decompensation, for a better long-term outcome. In this review, we will discuss transjugular intrahepatic portosystemic shunt indications in 2020 in patients with cirrhosis and portal hypertension, with a special focus on variceal bleeding and refractory ascites. Then, we will describe transjugular intrahepatic portosystemic shunt-related complications, the contraindications and the current knowledge on patient’s selection.
Keywords
Clinical case
A 62-year-old male patient with alcohol-related liver cirrhosis was referred to the intensive care unit for haematemesis. Clinical examination revealed mean arterial pressure of 60 mm Hg, ascites and jaundice. Blood examination results were the following: haemoglobin 8 g/dl, total bilirubin of 3.6 mg/dl (60 µmol/l), creatinine 1.2 mg/dl (106 µmol/l), International Normalized Ratio (INR) 1.4, albumin 3 g/dl. The Child-Pugh score was 11, and the Model for End Stage Liver Disease (MELD) score 17. The patient received Intravenous (i.v.) antibiotics (ceftriaxone 1 g), and terlipressin 2 mg. After orotracheal intubation, an upper endoscopy was performed and showed large oesophageal varices with a platelet-fibrin plug; band ligation was performed. The level of N-terminal pro-brain natriuretic peptide (NT-proBNP) was 96 pg/ml and the echocardiography excluded right heart insufficiency and pulmonary arterial hypertension. Two days later, the patient underwent transjugular intrahepatic portosystemic shunt (TIPS) placement without any complication. He was discharged 1 week after the procedure. Four weeks later, clinical evolution was favourable, without rebleeding, no signs of hepatic encephalopathy and remission of ascites. The Child-Pugh score was 8, and the MELD score 13.
Introduction
Since its first description in dogs by Rösch et al. published in 19711 and the first implantation in 1989 in human, the TIPS technique has evolved, improved, and become a widespread treatment for portal hypertension (PHT) related complications. Development of materials combined with a better selection of patients has significantly improved the prognosis of patients treated by TIPS.
Median survival for patients with compensated cirrhosis is over 12 years but shortens to less than 2 years in decompensated cirrhosis with a 5-year mortality rate up to 88% when two decompensating events have occurred. 2
Indications
Variceal bleeding (VB)
VB is one of the main complications of cirrhosis. Its prognosis has improved for the last 30 years due to the combination of medical therapy (vasoactive drugs and antibiotics) and endoscopic therapy, with a 6-week survival rate reaching 85% in the last series. 3 TIPS may be indicated in three clinical situations: (a) as rescue therapy (salvage TIPS); (b) in patients in whom stabilization has been achieved thanks to endoscopic, vasoactive and antibiotic treatment, but who are at risk of rebleeding (early or preemptive-TIPS (preemptive TIPS)); and (c) in patients experiencing rebleeding despite an optimal secondary prophylaxis.
Salvage TIPS
Salvage TIPS is a therapy that has proven its effectiveness in patients with cirrhosis and refractory VB. Refractory VB is defined by VB that does not respond to the combination of vasoactive drugs, endoscopic treatment and antibiotherapy. The primary outcome is control of bleeding and the improvement of survival. Despite excellent control of bleeding, mortality is high, ranging from 30–50%. 4 Mortality is usually associated with hyperbilirubinaemia, renal failure, hyponatraemia, sepsis, catecholamine use and a high Acute Physiology And Chronic Health Evaluation (APACHE) score. 5 However, to date no robust data are able to select or exclude patients for the TIPS procedure, i.e. very high positive predictive value of early death for individual decision-making. In a study conducted in a French centre, 6 a series of patients with very severe cirrhosis (Child-Pugh score C14 or C15) and refractory variceal bleeding were described. In-hospital mortality was 100% despite the control of bleeding. After the implementation of the MELD score for graft allocation in France in 2007, a successful liver transplantation in five consecutive selected candidates after salvage TIPS in Child-Pugh C14–C15 patients was performed. Outcome was excellent in this small cohort (100% survival). Therefore, salvage TIPS could be considered as a futile procedure in Child-Pugh C14 or C15 cirrhotic patients who will not be candidates for liver transplantation. We recommend an expert’s advice for each case.
Preemptive or early TIPS
In VB, risk factors of early rebleeding after a successfully medical and endoscopic treatment are the severity of liver disease evaluated by Child-Pugh or MELD score, PHT and the severity of the bleeding episode. The concept of preemptive TIPS was first introduced by Monescillo et al.: 7 in this study, high-risk patients, defined by a hepatic venous pressure gradient (HVPG) ≥20 mm Hg were randomised into two groups, one group allocated to TIPS placement within the first 24 h after stabilization and the other one to the standard treatment. Rebleeding and survival were significantly better in the TIPS group. The main limits of this study were: (a) the need for HVPG measurement to select high-risk patients; (b) the standard treatment applied was sclerotherapy, an endoscopic technique associated with a failure rate of 30–40%. Thus, other studies were published in high-risk patients with a simpler definition, applicable in clinical practice. The pivotal study was published by García-Pagán et al. 8 and randomly assigned 63 patients with cirrhosis Child-Pugh C10–C13 and VB or Child-Pugh B with active bleeding during endoscopy within 72 h after admission to receive TIPS (32 patients) or standard therapy using non selective beta blockers (propranolol or nadolol) plus endoscopic band ligation (31 patients). During a median follow-up of 16 months, rebleeding or failure to control bleeding occurred in 14 patients (45%) in the standard therapy group, compared with one patient (3%) in the preemptive TIPS group. Furthermore, survival at 1 year was significantly better in the TIPS group (87.5% versus 61.3%). Last, hepatic encephalopathy (HE) was not more frequent in the preemptive TIPS group. Thereafter, other studies were published9–12 confirming the benefit of preemptive TIPS in terms of rebleeding. However, the benefit in terms of survival, especially in patients with Child-Pugh B cirrhosis and active VB is still matter of debate. The more recent randomised controlled trial (RCT) performed in China failed to demonstrate the benefit of preemptive TIPS in terms of survival in this latter group of patients. 13 Even if the Baveno VI Consensus recommends the placement of preemptive TIPS for the Child Pugh B and active VB and Child Pugh C10–C13 patients, 14 there is evidence that this statement will be changed during the next consensus in 2020. Moreover, no recommendation can be formulated in patients with the most severe disease, i.e. with Child-Pugh C14–C15 cirrhosis.
Secondary prophylaxis of VB
Secondary prophylaxis of VB relies on the association of non-selective beta-blockers and endoscopic treatment. If rebleeding occurs despite a well-conducted secondary prophylaxis, a TIPS placement must be discussed. A meta-analysis published in 2008 including 12 RCTs showed a significant decrease in rebleeding rates and death due to rebleeding after TIPS placement when compared to endoscopic treatment. More recently, two RCTs compared TIPS and standard secondary prophylaxis after a first episode of VB, in unselected Child-Pugh A to C patients. Lower rebleeding rates were observed in the two studies in patients treated by TIPS. 15 , 16 However, there was no difference in terms of survival in both studies.
Ascites
Refractory ascites
According to the criteria of the International Ascites Club, refractory ascites is defined as ‘ascites that cannot be mobilised or the early recurrence of which, i.e. after large volume paracentesis (LVP) cannot be satisfactorily prevented by medical therapy'.17
The benefit of TIPS for the prevention of recurrence of ascites is largely demonstrated. In the meta-analysis of individual data of Salerno et al., 18 the recurrence of tense ascites occurred in 42% of patients treated with TIPS and 89% of patients treated by LVP.
In terms of survival, the study of Lebrec et al. 19 showed lower survival among patients treated by TIPS while the trials of Rossle et al., 20 Gines et al. 21 and Sanyal et al.22 showed a similar survival between the two groups of patients. Finally, the two studies of Salerno et al. 23 and Narahara et al. 24 found a benefit in terms of survival in patients treated by TIPS. These contradictory results may in part be explained by the heterogeneity of the criteria of inclusions and exclusion within each (Table 1).
Main studies comparing large volume paracentesis (LVP) and other therapeutics in patients with refractory or recurrent ascites with transjugular intrahepatic portosystemic shunt (TIPS).
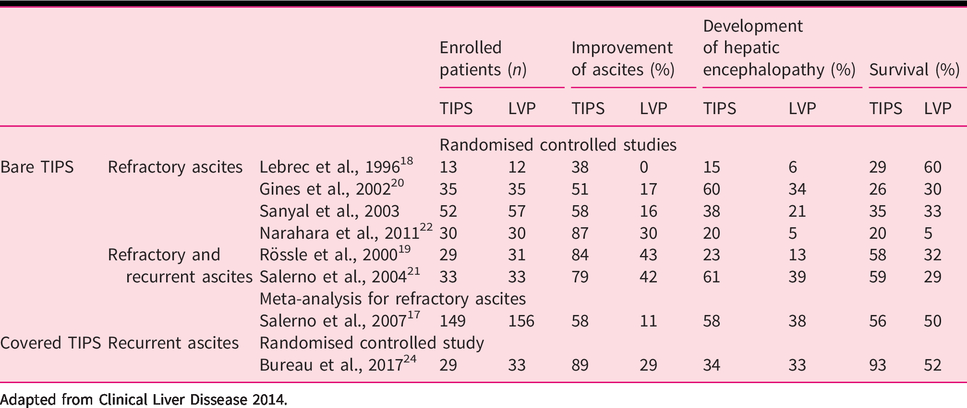
Adapted from Clinical Liver Dissease 2014.
The study of Bureau et al. 25 allowed defining criteria to select ‘good' candidates for the TIPS placement. Bilirubin level <50 µmol/l (<3 mg/dl) and of platelets > 75 *109/L were associated with significant better survival without transplantation.
Recurrent ascites
Recurrent ascites is defined as ascites that recurs earlier than 1 month after initial control. Bureau et al. compared the prognosis of patients with recurrent ascites receiving either TIPS with covered stents or standard medical treatment. 26 In order to be included, they needed to have required at least two LVPs within a minimum 3 weeks interval. Noteworthy, about 30% of patients had a history of VB and about 20% had a history of renal failure, highlighting the severity of their circulatory dysfunction. Survival without transplantation at 1 year was 92% in the TIPS group and 52% in the LVP group. The number of LVPs was lower in the TIPS group (32 vs 320). There were more episodes of VB, complicated hernias and hospitalizations in the LVP group. The rate of occurrence of HE was similar in both groups (35%).
TIPS complications
The main complications of TIPS are liver failure, HE and cardiac decompensation.
Liver failure
Creating a porto-systemic shunt and subsequently a portal flow diversion leads to decrease in liver perfusion with possible progression to liver failure. Multiple models were developed in order to predict survival: the MELD score has been shown to be superior to the Child-Pugh score as a predictor of short-term outcome after TIPS. 27 In case of elective TIPS, patients with a MELD score of 18 or greater have a significantly higher 3-month mortality rate than those with a MELD score of 11–17 and 10 or less (35%, 16% and 0%, respectively). 28
In case of post-TIPS liver failure, recalibration of TIPS and liver transplantation should be discussed.
HE
The incidence of post-TIPS HE is about 35% in highly selected patients. The principal risk factors are: an older age, previous history of HE, presence of minimal HE a higher Child-Pugh and MELD score and sarcopaenia. The treatment of post-TIPS HE refers to medical management (lactulose, and then rifaximin). In case of refractory HE, it has been proposed that endovascular shunt reduction may be the key to improving and controlling HE. In case of refractory HE, however the definite treatment for post-TIPS HE is liver transplantation. 29
Cardiac decompensation
The creation of portosystemic shunt leads to a large-volume blood shift from the splanchnic to the systemic circulation, leading to an increase in cardiac output and right heart pressures. The abrupt and sudden increase in right heart pressures is usually transient. Cirrhotic cardiomyopathy is defined as chronic cardiac dysfunction in a cirrhotic patient and is characterised by a blunted contractile response to stress and an altered diastolic relaxation. Patients with cirrhotic cardiomyopathy have the highest risk of developing post-TIPS cardiac failure. Prognostic factors of diastolic dysfunction in cirrhotic patients treated with TIPS have been studied by Cazzaniga et al. 30 and Rabie et al. 31 Cazzaniga et al. showed an association between a post-TIPS E/A ratio<1 (marker of diastolic dysfunction) and mortality, however an E/A ratio>1 before TIPS was not associated with outcome.
Last, regarding heart failure, a very recent prospective study has shown that cardiac decompensation occurs in about 20% of patients. 32 The authors described that a combination of a brain natriuretic peptide (BNP) <40 pg/ml or a NT-proBNP<125 pg/ml before TIPS and the exclusion of diastolic dysfunction at echocardiography ruled out the risk of cardiac decompensation.
TIPS contraindications and pre-TIPS evaluation
It seems crucial to carefully select patients for TIPS placement; however contraindications for TIPS need always to be balanced against the benefit of treatment. In case of salvage TIPS, there is no strict contraindication.
In case of ascites, TIPS is contraindicated in patients with heart failure, advanced liver failure, defined by a Child-Pugh score >13 or a MELD score >19, and chronic or recurrent HE. Exclusion criteria were indeed heterogeneous amongst the RCTs, but some of them were similar, such as age>70 or 75 years, HE on the day of TIPS placement, Child-Pugh >11, Hepatocellular carcinoma (HCC) out of Milan criteria and heart failure.
A careful clinical, biological examination and morphological evaluation is required: (a) clinical history, including age, systematic search for a previous episode of HE or heart decompensation; (b) physical examination with screening for confusion, flapping, left or right signs of heart failure; (c) biological evaluation including routine blood examinations, hepatic function, renal and cardiac function with BNP or NT-proBNP; (d) morphological evaluation including abdominal ultrasound exam or Computed tomography (CT) scan, and echocardiography.
TIPS seems to be the best therapeutic option in patients <65 years, without any previous episode of HE, with a Child-Pugh score <13 and a MELD score <19, a total bilirubin level <50 µmol/l, a platelet count >75 × 109/l, a normal value of BNP/NT-proBNP, and normal echocardiography. TIPS should be contraindicated in patients >70 years, with history of more than two episodes of HE.
Conclusion
Technical progress and better selection of patients have improved the outcome of patients with cirrhosis treated by TIPS. In terms of VB, there are three clinical scenarios: TIPS as a rescue therapy in refractory bleeding, in the prevention of rebleeding in high-risk patients with controlled acute variceal bleeding and in secondary prophylaxis of VB. In cases of recurrent ascites, TIPS placement improves survival, while in refractory ascites TIPS decreases the number of LVPs and other PHT related complications (see Supplementary Material Abstract).
To date, no pharmacological prophylaxis of HE has shown a beneficial effect in patients treated by TIPS. The results of a large French RCT using rifaximin are expected. Last, we strongly suggest for each patient that whenever a TIPS placement is discussed the anticipation of liver transplantation could be envisioned in the case of severe post-TIPS complication.
Supplemental Material
sj-pdf-1-ueg-10.1177_2050640620952637 - Supplemental material for Transjugular intrahepatic portosystemic shunt in patients with cirrhosis: Indications and post-transjugular intrahepatic portosystemic shunt complications in 2020
Supplemental material, sj-pdf-1-ueg-10.1177_2050640620952637 for Transjugular intrahepatic portosystemic shunt in patients with cirrhosis: Indications and post-transjugular intrahepatic portosystemic shunt complications in 2020 by Adelina Horhat, Christophe Bureau, Dominique Thabut and Marika Rudler in United European Gastroenterology Journal
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AH: no conflict of interest; CB: speaker for Gore, consultancy for Alfasigma; MR: speaker for Gore, Gilead, Abbvie; DT: consultancy for Gore, Alfasigma, Gilead, MSD, AbbVie, Medday.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.