
Abstract
Background
Various techniques have been described for endoscopic resection of large symptomatic colon lipomas. Lipoma unroofing might provide a safer, more time efficient and easier technique compared to dissection-based techniques, endoscopic mucosal resection (EMR) or loop-assisted resection. The aim of this systematic review was to compare efficacy and safety (endoscopic resolution rates, clinical remission rates and adverse events) of lipoma unroofing with respect to dissection-based techniques, EMR or loop-assisted resection.
Methods
As most outcomes were binary in nature and several outcomes did not occur in some studies, routine calculation of standard errors in outcome probability was not possible. Therefore, original patient data were extracted, after which efficacy and safety were compared.
Results
Twenty four studies met the selection criteria, which encompassed 77 lesions (46.8% female, mean age 63 years (interquartile range (IQR) 53–72 years), mean size 45.4 mm (IQR 30.0–60.0 mm). Ten patients underwent unroofing (13.0%), whereas 7 (9.1%), 31 (40.3%) and 29 patients (37.7%) underwent dissection-based techniques, EMR and loop-assisted-snare resection, respectively. Endoscopic resolution rates were 60%, 100% (p = 0.103), 93.6% (p = 0.024) and 93.1% (p = 0.028). Clinical remission rates were identical in all four groups (100%). Amongst patients who underwent EMR and loop-assisted techniques, adverse events were identified in 12.9% (p = 0.556) and 13.8% (p = 0.556), respectively, compared to none in the unroofing and dissection-based resection group.
Conclusions
In patients with large colon lipomas, endoscopic treatment by unroofing, dissection-based resection, EMR and loop-assisted resection provided similar clinical remission rates. Amongst patients undergoing EMR and loop-assisted resection, increased endoscopic resolution rates were seen at the expense of more adverse events, although the latter did not reach statistical significance. Until more reliable comparative data are available, the most optimal resection technique should rely on local expertise and patient profile.
Keywords
Introduction
Gastrointestinal lipomas are benign lesions, which can be identified by several typical endoscopic features, such as the typical yellow hue, ‘naked fat sign’, the sub-epithelial or submucosal location and the ‘pillow sign’. Although generally asymptomatic, 75% of lesions >20 mm have been found to cause symptoms, with manifestations such as intussusception, ulceration, pain, diarrhoea, bleeding and large-bowel obstruction, which may necessitate endoscopic treatment.1,2 In the context of large colon lipomas, several endoscopic techniques have been reported, such as loop-assisted techniques and snare resection. However, in situations where the dimensions of the lesion make these methods unfeasible, endoscopic submucosal dissection (ESD),3,4 other dissection-based techniques and, most importantly, simple unroofing may offer effective alternative treatment options.5–10
Mentioned for the first time in 1997, the unroofing technique relies on intraluminal expulsion of the residual submucosal content following snare resection of the distal part of the subepithelial mass 11 (Figure 1). Subsequent spontaneous evacuation of the underlying residual lipomatous tissue is said to lead to complete resolution of these lesions. Little endoscopic experience is required, procedure time and costs are kept to a minimum and possible dissection-related adverse events can be averted, as only a simple snare resection is needed. Although no R0 resection will be acquired, relevance of an immediate complete resection is limited in the context of these benign lesions. Moreover, tissue from partial resection can still be sent for pathological evaluation to confirm the visual diagnosis. Regarding efficacy, there are reports of cases where re-intervention was required, presumably following insufficient unroofing, which may be caused by re-epithelialization following a limited unroofing site, hampering expulsion of the submucosal content.12,13 Comparative studies evaluating the different techniques used for resection of giant colon lipomas are scarce. Only one retrospective analysis has compared unroofing, endoscopic mucosal resection (EMR) and ESD in resection of 21 large colon lipomas, which showed complete resolution with all three techniques. 14
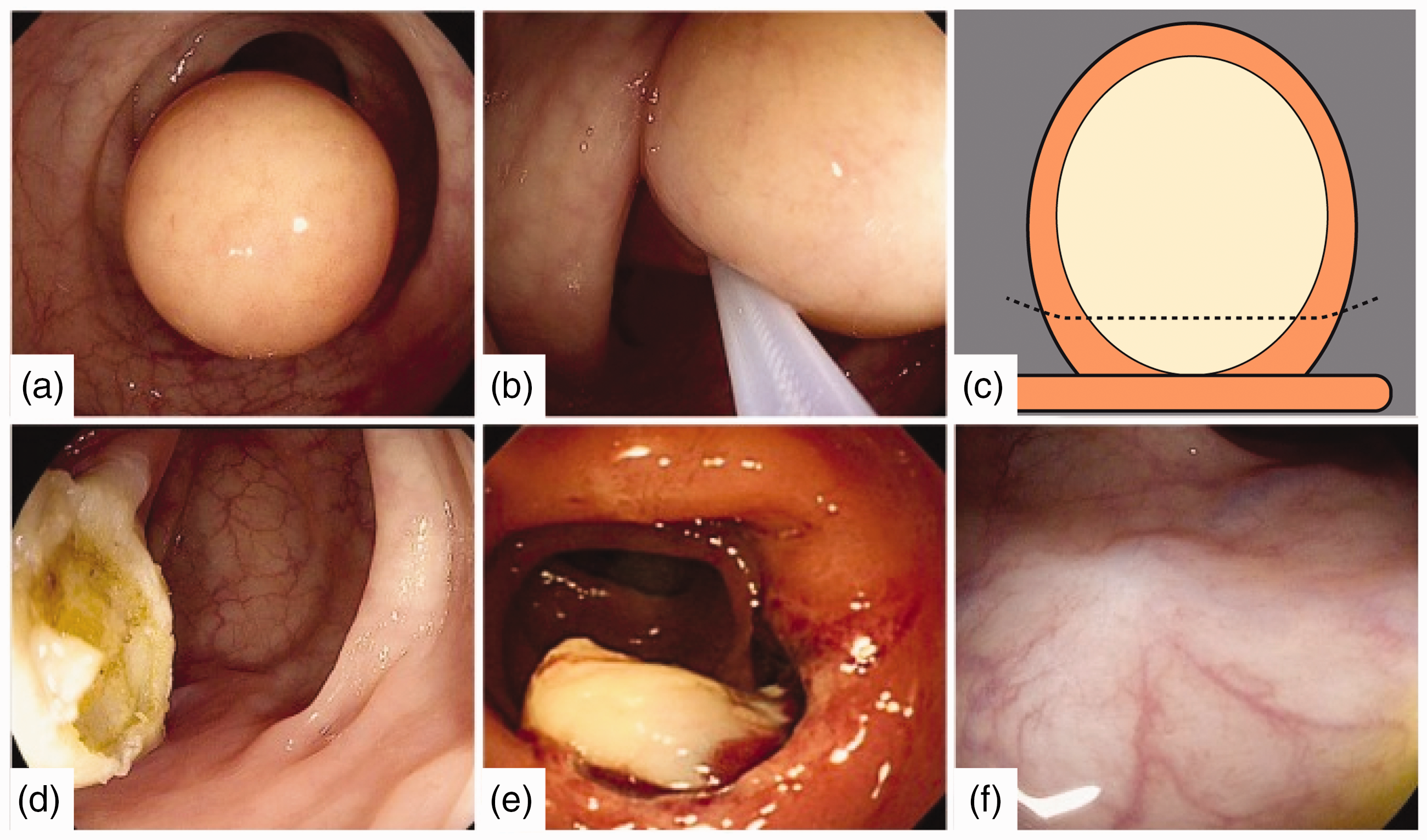
Unroofing technique. Large yellowish mass (30 mm×30mm) protruding into the lumen in the sigmoid colon (a). Partial snare resection at the base (b), with schematic illustration of the unroofing technique (c). Defect following partial snare resection, as expected showing a significant amount of residual lipoma at the base (d). Endoscopic follow-up the next day, revealing lipomatous tissue flowing from the snare into the lumen (e). Endoscopic follow-up after one year, showing complete resolution of the lesion. Reproduced with permission from author and publisher. 7
To our knowledge, no other studies comparing these techniques have been done in the setting of symptomatic colon lipomas. The aim of this systematic review was to compare the safety and efficacy of unroofing with dissection-based techniques, EMR and loop-assisted resection.
Methods
The current study was performed in accordance with the Preferred Reported Items for Systematic reviews and Meta-Analysis guidelines. 15 PubMed, Embase, the Cochrane Library and Clinicaltrials.gov were searched independently by A.M.V.B. and M.B. for studies reporting or evaluating endoscopic treatment of symptomatic colon lipomas until the 30 March 2019. The following search terms were used: ‘colon’, ‘ESD’, ‘EMR’, ‘endoscopic resection’, ‘endoscopy’, ‘giant lipoma’, ‘lipoma’, ‘loop’, ‘loop-assisted resection’ and ‘unroofing’.
Study selection and data extraction
Studies were selected by means of preset selection criteria. Subsequent inclusion and exclusion criteria are mentioned in Supplemental Table S1. Data were extracted independently by the first two authors, without any language restrictions. Furthermore, the bibliographies of relevant articles were also reviewed to identify additional studies. Literary searches by both investigators were compared, in case only one investigator identified an eligible study. Discrepancies and the decision over whether to include or exclude a study were resolved by means of discussion. Data of interest were extracted into a single database. For the studies in the final analysis, this included: author(s), year of publication, country of origin and language, article type, number of patients, sex, mean age, lesion size and type, resection technique, complete resolution rates and adverse events. Due to the lack of controlled trials, retrospective and prospective observational studies were also included, as were case reports. We considered all clinical studies or reports that had been published until March 2019. As the current work only involved previously performed studies, approval by the Institutional Review Board or individual patient consent was deemed unnecessary.
Interventions
We compared four different endoscopic techniques for colon lipoma management: lipoma unroofing, dissection-based techniques, EMR and loop-assisted techniques. Lipoma unroofing is defined as the application of partial snare resection, after which the endoscopist relies on spontaneous intraluminal expulsion of the lesional contents for lesion resolution. If predominantly dissection-based techniques were used during the endoscopic procedure, for example using pure ESD or when dissection of a stalk was performed, these techniques were considered dissection-based techniques. All procedures performed with snare resection (piecemeal or en-bloc) with and without submucosal injection are hereafter designated as EMR. Similarly, if during the procedure a detachable was used, be it for preventive haemostatic reasons or in context of the ‘loop-and-let-go’ technique, 16 the procedure was regarded as a loop-assisted resection, regardless of the actual resection technique used (snare resection or spontaneous loop-assisted amputation).
Outcomes
‘Endoscopic resolution’ was defined as the complete disappearance of the lesion on any given time point, without the use of adjunctive therapies other than the index procedure. ‘Clinical remission’ was defined as the successful treatment of symptoms attributed to the colon lipoma. All adverse events were included. No specific exclusion criteria for adverse events were used.
Statistical analysis
As outcomes were mostly binary and some outcomes did not occur in several studies, classic calculation of standard errors in outcome probability was not possible. Therefore, original patient data were extracted, after which complete resolution rates and adverse events were compared. For discrete data, proportions and percentages were reported, whereas for continuous data, medians and the corresponding interquartile ranges (IQR) were used. We used Fisher’s exact test for categorical data, the Mann–Whitney U-test for continuous data and Student’s t-test and the Kruskal–Wallis test for independent means. We calculated odds ratios (OR) with 95% confidence intervals. Furthermore, a p-value of <0.05 was regarded as statistically significant. The included studies showed extensive methodological variation, as case reports, prospective studies and retrospective analyses were included. For this reason, heterogeneity assessment by I2 was not performed, as the extensive variation in the studies included would inevitably lead to a high I2. The same applies to the Newcastle–Ottawa scale. As most studies were not controlled, this tool could not be used to assess the quality of the included studies in this particular systematic review.
Results
Twenty four studies between 1979 and 2019 met the selection criteria. The selection process is depicted in Supplemental Figure S1. Three retrospective analyses, 20 case reports and one prospective study were included (Supplemental Table S2). In total, 77 individual patients and lesions were identified, of whom 46.8% were female patients, with a mean age of 63 years (IQR 53–72 years) with a mean lesion size of 45.4 mm (IQR 30.0–60.0 mm). Ten (13.0%) patients underwent unroofing, whereas seven (9.1%) patients, 31 (40.3%) patients and 29 (37.7%) patients underwent dissection-based techniques, EMR and loop-assisted resection, respectively (Table 1). In the last group, 21 (72%) patients were treated using the ‘loop-and-let-go’ technique, 16 while the remaining eight (28%) patients underwent simple snare resection following pre-emptive detachable loop application. Overall, colon lipomas caused symptoms in a total of 40/77 (52%) patients, of which pain (n = 22; 29%) was the most frequently reported symptom (Supplemental Table S3). Patients undergoing unroofing were more frequently symptomatic than patients treated with EMR (80% vs. 48%, p = 0.027) and experienced pain more frequently (70% vs. 16%, p = 0.003). When comparing baseline characteristics such as age, sex and lesion size, no significant differences were detected amongst the four different techniques (Table 2).
Baseline characteristics.
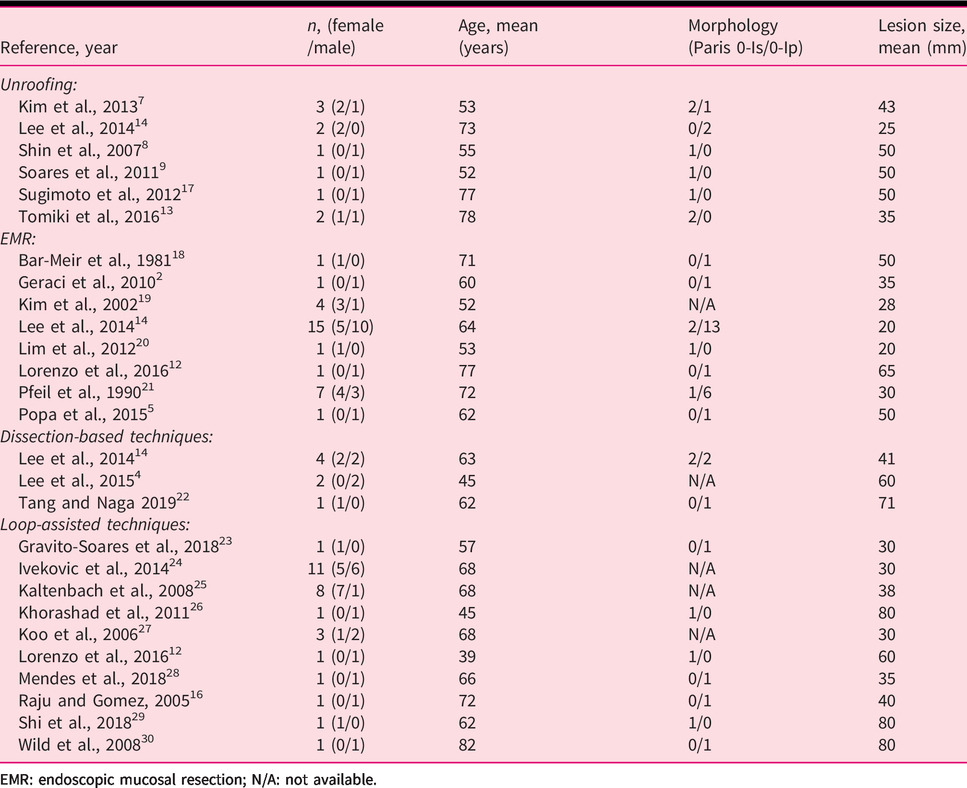
EMR: endoscopic mucosal resection; N/A: not available.
Comparison baseline characteristics.

Efficacy
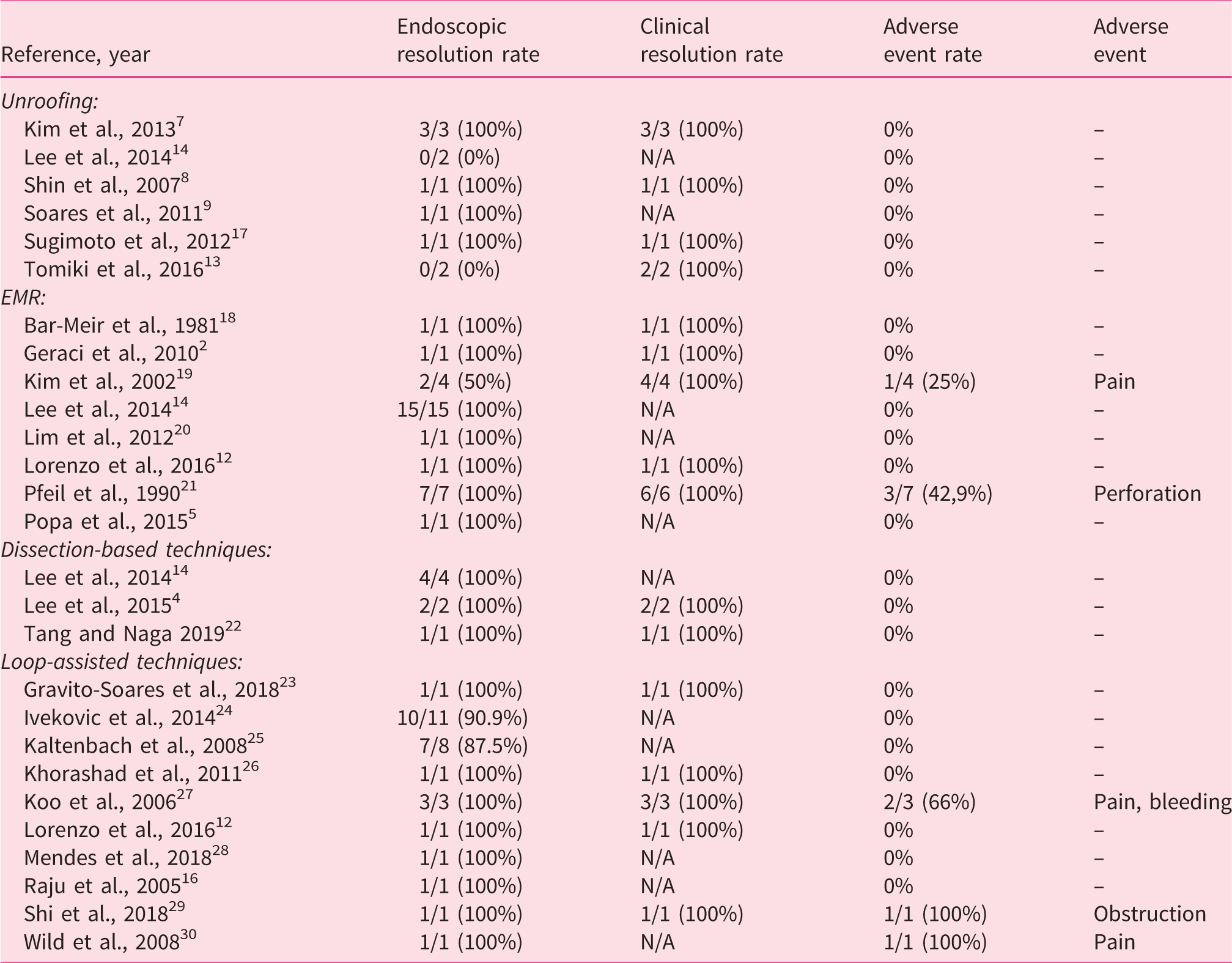
Cumulative endoscopic resolution rates were 60% for unroofing, 100%, and 93.6% and 93.1% for dissection-based resection, EMR and loop-assisted resection, respectively (Table 3). Compared to unroofing, only EMR (p = 0.024) and loop-assisted resection (p = 0.028) led to a significant increased rate of endoscopic resolution (Table 4). Using a dissection-based technique, only a trend towards increased complete endoscopic resolution was seen (60% vs. 100%, p = 0.103), which could be attributed to the low numbers of lesions treated by this specific technique, as a perfect efficacy was also observed in this group. Clinical remission rates were 100% in all endoscopic techniques. When comparing Paris 0-Is lesions with 0-Ip lesions, no significant differences in complete endoscopic resolution or clinical remission were seen (Supplemental Table S4).
Individual outcomes.
Cumulative outcomes.
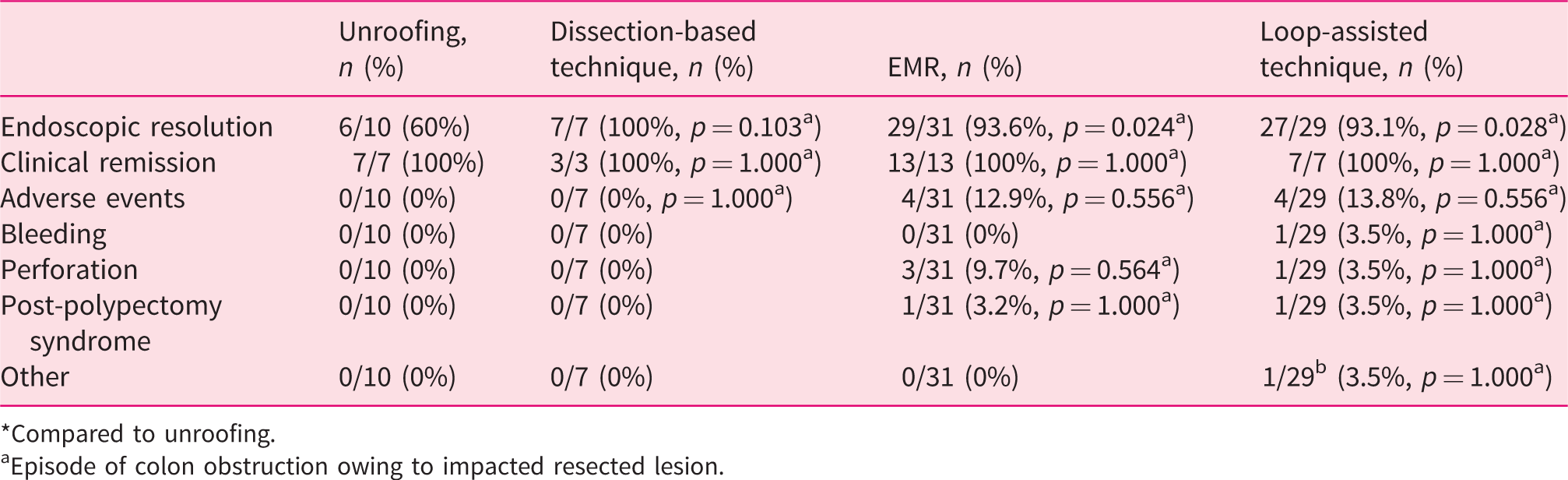
*Compared to unroofing.
aEpisode of colon obstruction owing to impacted resected lesion.
Safety
No adverse events were identified in patients receiving endoscopic treatment by unroofing and dissection-based resection. Amongst patients who underwent EMR and loop-assisted techniques, adverse events were identified in 12.9% (p = 0.556) and 13.8% (p = 0.556), respectively (Table 4). EMR led to perforation in three patients, whereas loop-assisted resection caused bleeding, perforation, post-polypectomy syndrome and obstruction in one patient each. Similar to the efficacy outcomes, no differences were seen regarding safety when comparing Paris 0-Is with Paris 0-Ip lesions (Supplemental Table S4). Number-needed-to-treat analysis revealed that eight patients needed to undergo unroofing in order to prevent one adverse event amongst patients receiving EMR or loop-assisted resection.
Discussion
In our systematic review, unroofing, dissection-based resection, EMR and loop-assisted resection provided identical clinical remission rates, although increased endoscopic resolution rates were seen when comparing unroofing with EMR and loop-assisted resection. These increased endoscopic remission rates came at the cost of increased adverse events in up to 13.8% of patients compared to none amongst patients undergoing unroofing or dissection-based resection. Presumably due to the low numbers included, no significant difference in adverse event rates was proven. Using lesion morphology as a discriminator, no differences in efficacy and safety were seen.
Several authors have questioned the efficacy of the unroofing technique.13,31 Tomiki et al. reported two colon lipomas (20 and 50 mm) managed by unroofing. In their cases, additional endoscopic resection was required because the initial unroofing had proven to be too limited, leading to incomplete lesion resolution. 13 Indeed, sufficient tissue should be resected in order to achieve a large mucosal aperture through which the intra-lesional lipomatous contents can migrate. Because there is little long-term follow-up data and relook colonoscopies are not frequently performed, it is uncertain whether every lesion treated by unroofing completely disappears or, in some cases, a reduced amount of lipoma persists. The relevance of a complete resolution is, however, questionable, as it is considered that an already partial obliteration will lead to sufficient symptom relief. Our data suggest the same, as clinical remission rates were identical, despite significantly lower endoscopic resolution rates amongst patients in the unroofing group.
Studies comparing the different techniques are scarce, which can be attributed to the low frequency at which colon lipomas in general lead to symptoms. The largest comparative data originate from a retrospective analysis performed in 2014, 14 where 21 colon lipomas were treated by three different techniques: unroofing (n = 2), EMR (n = 15) and dissection-based resection (n = 4). Although the two lesions treated by unroofing were intrinsically incomplete resections, inherent to the unroofing technique, complete endoscopic resolution without adverse events was also achieved in these two patients at follow-up. However, owing to the limited sample size and methodological quality of this retrospective study, firm conclusions regarding the individual treatment profiles cannot be made.
Concerning the current study, there are several weaknesses that need to be assessed. First, due to the nature of the papers involved, publication bias should be taken into account. However, this was the case in all four technique subgroups, and one could argue that this could annul the effect of publication bias when comparing these techniques. Second, due to the lack of randomized controlled trials, only case reports, one prospective study and three retrospective analyses were included. Methodological heterogeneity is therefore significant in our systematic review. Third, due to the low numbers of patients receiving the unroofing technique and dissection-based resection, our study might be significantly underpowered. We performed a power calculation and found that at least 34 cases treated by unroofing are needed to reach significance concerning safety outcomes. Larger and higher-quality studies are therefore desperately needed, although this presumably will take a multi-national effort and will be time-consuming because of the rarity of these large symptomatic colon lipomas. Finally, significant rates of missing data concerning clinical remission in the EMR and loop-assisted resection group were identified. Therefore, caution should be exercised when drawing conclusions regarding this specific outcome. Our study also has several strengths. To our knowledge, this is the largest comparative study concerning endoscopic management of colon lipomas, encompassing the majority of published work in this specific field. Furthermore, no earlier systematic reviews have been published in this context.
It has been suggested that until larger studies or longer follow-up data are available, management of symptomatic large and giant colon lipomas should be individualized based on local expertise, the patient’s age and co-morbid conditions. 31 Indeed, complete resection by dissection-based resection for example should be considered in situations where unroofing has failed in the past, amongst the young or when local ESD expertise is readily available. However, in many Western endoscopy centres where ESD expertise might be limited, endoscopic unroofing should be considered the primary technique, especially in situations where the lesion cannot be captured by detachable snare or classic snare, the latter being often the case in lesions >20 mm. Also, in situations where co-morbidities dominate, for example in elderly patients, low-risk unroofing seems to possess the most optimal treatment profile.
In conclusion, the lack of adverse events following unroofing suggests that this technique might provide a safer therapeutic option in patients with large symptomatic colon lipomas compared to EMR and loop-assisted resection, without sacrificing chances of clinical remission. Especially in centres where local expertise concerning ESD might be limited, in elderly patients or when lesions cannot be captured by snare, unroofing may be the treatment of choice. However, significant heterogeneity and variable methodological quality of the studies involved should be taken into account. Therefore, until more comparative data are available, the ideal resection technique should depend on local expertise and patient profile.
Supplemental Material
sj-pdf-1-ueg-10.1177_2050640620948661 - Supplemental material for Endoscopic treatment of large symptomatic colon lipomas: A systematic review of efficacy and safety
Supplemental material, sj-pdf-1-ueg-10.1177_2050640620948661 for Endoscopic treatment of large symptomatic colon lipomas: A systematic review of efficacy and safety by Michiel Bronswijk, Anne-Marie Vandenbroucke and Peter Bossuyt in United European Gastroenterology Journal
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M.B. received travel grants from Takeda and Prion Medical. P.B. received financial support for research from AbbVie, Mundipharma, Pfizer, Janssen and Mylan; lecture fees from AbbVie, Takeda, Pfizer and Janssen; and advisory board fees from Abbvie, Takeda, Hospira, Janssen, MSD, Mundipharma, Roche, Pfizer, Sandoz and Pentax. A.-M.V. declares no competing interests.
Ethics approval
The current work only involved previously performed studies, therefore approval by the Institutional Review Board was waived.
Informed consent
Individual patient consent was waived.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.