
Abstract
Crohn’s disease (CD) is a chronic inflammatory bowel disease that usually progresses to bowel damage, defined as strictures, fistulas and abscesses. These complications require intestinal resection and lead to further irreversible structural damage. Cross-sectional imaging, such as magnetic resonance imaging, computed tomography and ultrasound, are accurate in assessing intestinal damage at a definite time point and the progression of damage over time. Recently, an imaging-based index, the Lémann Index, has been proposed and developed in order to quantify bowel damage in CD patients; emerging data confirm that this Index can measure the structural damage with good sensitivity to change. One challenge remains to understand whether existing or future treatments might be able to stop bowel-damage progression or even reverse intestinal damage, improving the prognosis and changing the natural history of CD. We reviewed the current data available in the literature focused on the measure of structural damage in CD patients, mainly focusing on the impact on therapies in reversing bowel damage. We also explored some further perspectives on measuring and targeting intestinal damage in clinical research and in clinical practice as an ultimate therapeutic target.
Brief clinical case
Two 29-year-old patients were diagnosed with ileal Crohn’s disease (CD). Colonoscopy showed deep ulcers and passable stricture for 15 cm in the terminal ileum, and this was confirmed by magnetic resonance imaging (MRI) enterography. No obstructive symptoms were present. The two patients were treated for 24 weeks with anti-tumour necrosis factor (TNF). However, one patient achieved remission, and the other one had obstructive symptoms requiring ileal resection. After one year, both patients presented with clinical remission (Harvey–Bradshaw Index <4), biochemical remission (normal C-reactive protein (CRP)) and no endoscopic lesions. There was, however, one major difference: one of them had permanent CD-related structural damage due to ileal resection, whereas the other one had no active structural bowel damage.
How to diagnose structural damage in CD
As in rheumatoid arthritis, 1 the concept of bowel damage has also been investigated in inflammatory bowel disease (IBD), in particular in CD. The advances in cross-sectional techniques, such as ultrasounds (US), computed tomography (CT) enterography and MRI, which are routinely used with the same accuracy to assess CD activity, 2 have led to better evaluation of extra-intestinal complications (strictures, fistulas and abscesses), which can be considered as signs of bowel damage.3,4
There is no clear definition of bowel damage, since the presence of irreversible fibrosis or penetrating complications may coexist with active inflammation.5,6 Usually, in CD, a shift in disease behaviour according to the Montreal classification 7 from non-stricturing non-penetrating behaviour to a stricturing or penetrating phenotype is considered as disease progression. 8 Moreover, the presence of any complication, such as stricture, fistula or abscess, is widely accepted as bowel damage.3,8 Peyrin-Biroulet et al. 8 defined bowel damage as the presence of any fistula (including perianal fistulas), abscess or stricture assessed by CT or MRI. Quantification of cumulative bowel damage is thus important to understand how the disease progresses and tp plan an effective therapeutic management that could prevent bowel-damage progression over time.
Quantifying structural bowel damage: available proposed scores
The assessment of bowel damage requires a full evaluation of the gastrointestinal tract. A combination of endoscopy9,10 together with imaging techniques, such as MRI, CT or US, allows the involvement of the bowel wall and extra-luminal complications (including fistulas and abscesses), as well as perianal disease,1,2,11–14 to be assessed and can give a precise overview of the damaged digestive tracts.
Two scores of intestinal damage based on imaging techniques have been proposed: the Lémann Index15,16 based on a combination of endoscopy, MRI or CT findings and surgical history, and the sonographic lesion index for CD (SLIC)17,18 based on the small intestine contrast ultrasonography (SICUS). 17 While the validity of the Lémann Index has been widely investigated in observational cohort studies, the SLIC has yet to be validated in further studies, mainly because of the limitations and the poor reproducibility of the SICUS.
The Lémann Index
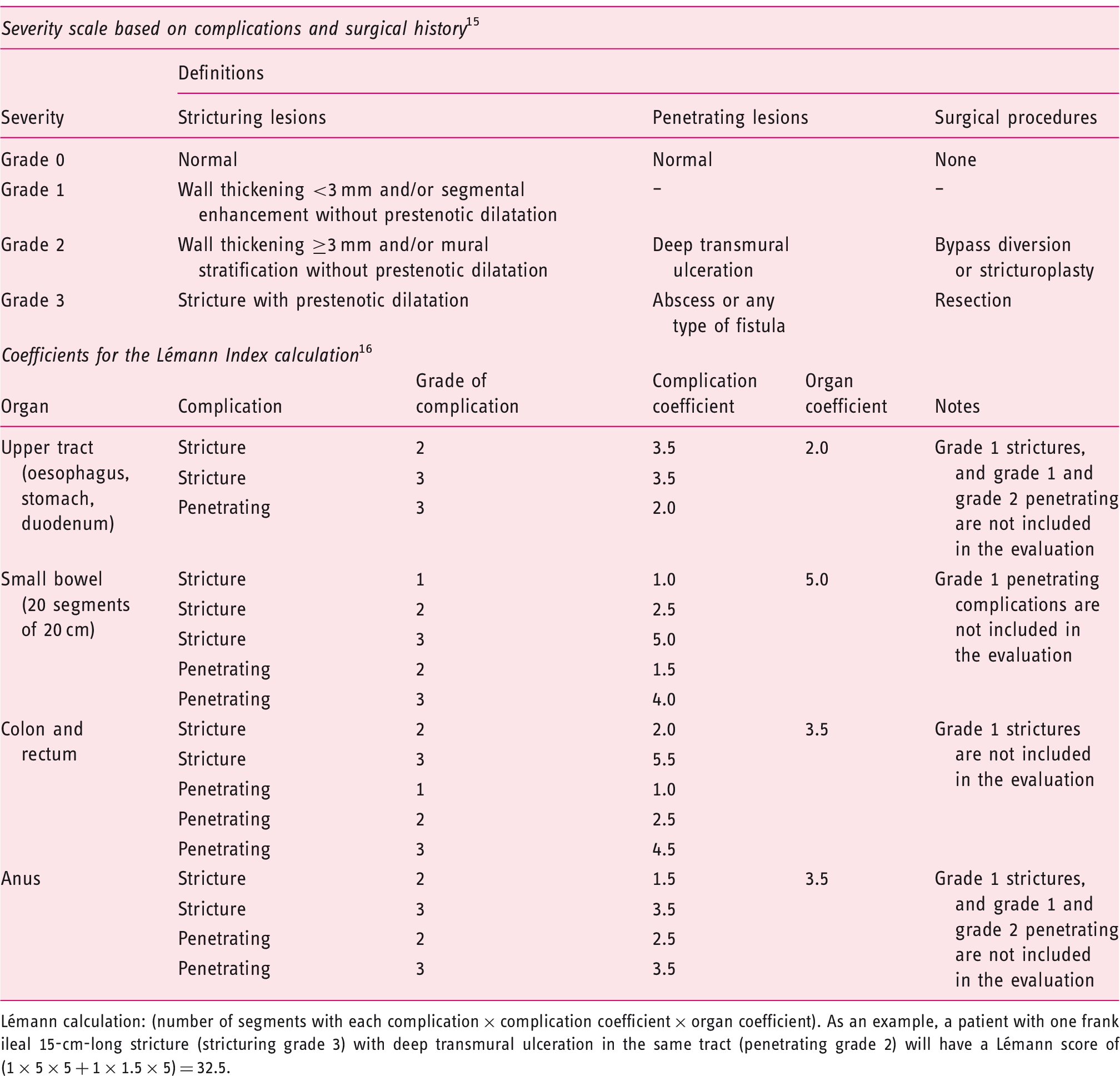
Lémann calculation: (number of segments with each complication × complication coefficient × organ coefficient). As an example, a patient with one frank ileal 15-cm-long stricture (stricturing grade 3) with deep transmural ulceration in the same tract (penetrating grade 2) will have a Lémann score of (1 × 5 × 5 + 1 × 1.5 × 5) = 32.5.
Natural history of bowel-damage progression in CD
IBD, including CD and ulcerative colitis (UC), are chronic, destructive, progressive and disabling diseases. CD involves the entire gastrointestinal tract, mainly the ileum and the proximal colonic tract, 20 and can affect the entire bowel wall, even with extra-mural complications, whereas UC affects only the colonic tract and is limited at the mucosal level. 21 In CD, the chronic inflammatory pattern activates tissue-repairing mechanisms which lead to irreversible fibrosis, or deep ulcers may go through the entire bowel wall, resulting in fistulas and abscesses. 22 All these complications cause permanent bowel damage, since they usually require surgery. 23 In UC, these complications are rare. However, in long-standing disease, there could be an infiltration of neutrophils and activation of fibroblasts, resulting in colonic damage and loss of function. 24
Up to 60% of patients who present with a non-stricturing non-penetrating CD phenotype at diagnosis evolve to stricturing or penetrating disease.25,26 About 40% of CD patients present with bowel damage at the time of diagnosis. 4 Cumulative CD-related bowel damage can compromise the intestinal function, with important consequences for patients’ quality of life, including disability, 27 although no studies have directly investigated this association. Whether prevention of organ damage by early effective therapy or treatment to reverse bowel damage in IBD can be considered achievable goals remains unclear.
Is bowel damage reversible in IBD?
Measures of structural bowel damage in clinical studies.
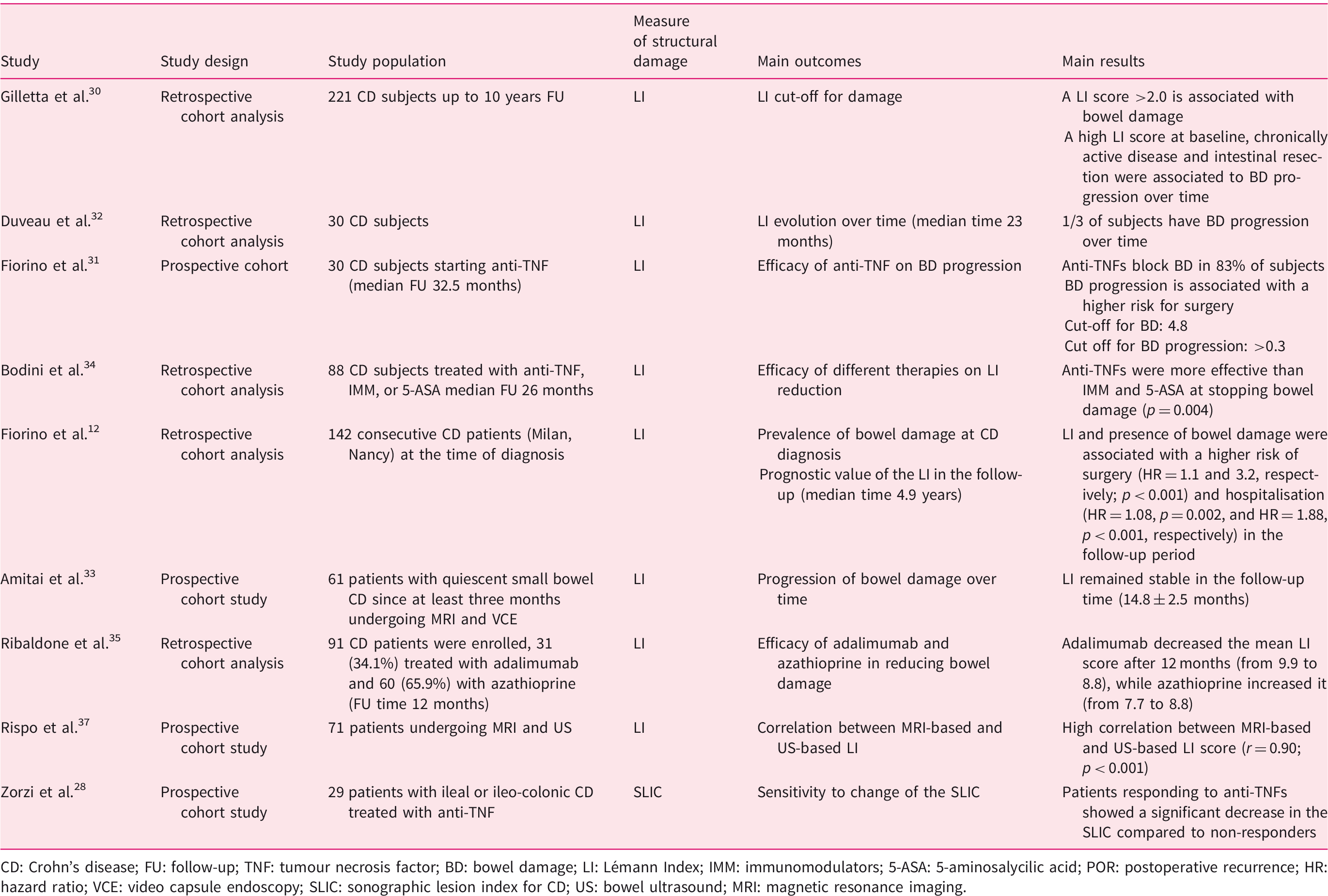
CD: Crohn’s disease; FU: follow-up; TNF: tumour necrosis factor; BD: bowel damage; LI: Lémann Index; IMM: immunomodulators; 5-ASA: 5-aminosalycilic acid; POR: postoperative recurrence; HR: hazard ratio; VCE: video capsule endoscopy; SLIC: sonographic lesion index for CD; US: bowel ultrasound; MRI: magnetic resonance imaging.
Fiorino et al. 29 investigated bowel damage variations in 30 subjects treated with anti-TNF and followed up prospectively for a median of 32.5 months. A Lémann Index score of 4.8 was found to be the best cut-off value for bowel damage, and an increase of >0.3 in the Lémann Index score was associated with bowel-damage progression. Anti-TNFs were effective in stopping bowel-damage progression in 83% of subjects. Bowel-damage progression was associated with the risk of major surgery in the follow-up period (hazard ratio (HR) = 0.19, p = 0.005). 29 Bodini et al. 32 evaluated 104 CD patients divided in three study groups according to treatments received – biological drugs (n = 40; 38.4%), azathioprine (n = 19; 18.3%) and mesalazine (n = 45; 43.3%) – for a median time of 29.5 months. The median Lémann Index score did not change significantly in the biological group (p = 0.543), whereas it increased in the azathioprine group (p = 0.0006) and in the mesalazine group (p < 0.0001), suggesting that resolution of inflammation may be associated with the blockade of disease and damage progression in CD patients. These results are also confirmed by a retrospective analysis by Ribaldone et al. 33 who found a decrease in the Lémann Index score after 12 months (from 9.9 to 8.8) in patients with CD treated with adalimumab compared to CD patients treated with azathioprine, in whom the mean Lémann Index score increased (from 7.7 to 8.8). In this study, adalimumab was associated with a significantly higher bowel-damage regression/blockade than in patients treated with azathioprine (67% vs. 28%, respectively; p = 0.006). Magro et al. also showed that disease progression was lower for both monotherapy with azathioprine (HR = 0.15, p < 0.001) or combination therapy with anti-TNF-α (HR = 0.33, p < 0.001), whereas upper gastrointestinal-tract involvement, male sex and steroid use were associated with an early progression of phenotype from B1 to B2 or B3 (p < 0.001). 34
A prospective study 31 of 61 CD patients with known quiescent small-bowel CD, followed up with magnetic resonance enterographies and video capsule endoscopies for a median of 14 months, showed that significant structural bowel damage was present in 21.4% at baseline, defined as a Lémann Index score >4.8. However, structural bowel-damage progression, defined as an increase in the Lémann Index score of >0.3, was negligible in the follow-up time.
All these data suggest that the blockade of disease progression as assessed by the Lémann Index might be a relevant goal to assess the long-term effectiveness of therapeutic management in CD. Early treatment may be effective in preventing bowel-damage progression in CD. A retrospective analysis of 88 patients followed up at the Mount Sinai Hospital in New York showed that damage progressed in 29 (50%), regressed in 20 (34.5%) and stabilised in 9 (15.5%) among the 58 early-treated cases. There was a trend in favour of earlier introduction to slow the rate of progression (ρ = 0.241; p = 0.069). However, further prospective large studies are needed to confirm these preliminary findings.
The Lémann Index has been developed by using MRI or CT as a standard cross-sectional imaging technique to assess structural bowel damage. Recent advances in knowledge in regards of bowel US suggest that bowel damage can be assessed by this technique, translating the Lémann Index calculation by using US findings. Rispo et al. 35 developed a US-based Lémann Index and compared this index to the Lémann Index assessed by MRI. They prospectively enrolled 71 consecutive patients with CD. Seventy-three per cent of patients had complications (strictures and/or fistulas). Median MRI Lémann Index and US Lémann Index scores were 6.62 (95% confidence interval (CI) 4.2–9.7) and 6.04 (95% CI 3.6–9.2), respectively (ρ = 0.90; p < 0.001). There was no significant correlation between the Lémann Index and the Harvey–Bradshaw index (p = 0.9), while a significant correlation was found between both scores (US and MRI based) and CD duration (p = 0.01).
Measuring structural damage in IBD: future challenges
The concept of bowel damage is an emerging goal for the general management of CD, and it is strongly connected with disease severity. A Delphi consensus by 14 IBD specialists under the umbrella of the International Organization for IBD has agreed on the relevance of accumulating bowel damage (in particular, complications and major surgery with intestinal resection) as associated with overall CD severity. 36 However, the best way to define, quantify and monitor bowel damage over time is still debated.
The Lémann Index is accurate for assessing bowel damage at a definite time point. However, there are some issues regarding this score in measuring bowel damage that are still to be clarified. First, data from Fiorino et al.
29
showed that structural bowel damage as measured by the Lémann Index can be reduced by effective therapies (Figure 1), in contrast with the definition of damage, which should be irreversible by a definition.
6
The presence of parameters of inflammation, such as deep ulcers, is the main reason for such a discrepancy. The persistence of bowel damage measured by the Lémann Index when inflammation is absent, and the absence of a correlation with the current endoscopic and radiological scores, such as the Simplified Endoscopic index of Severity or the MaRIA score,29,37 indicate, however, that the Lémann Index may be influenced by but is not a score of inflammation. In the same study, the authors suggest the evaluation of ‘residual bowel damage’, that is, the damage assessed by the Lémann Index after successful treatment of inflammation, as a pure parameter of the structural damage not related to active inflammation, and therefore the difference in the Lémann Index score at two different time points (i.e. before and after adequate time of therapy) would give clearer and more valid information on the disease course than a single measure at one definite time point. This aspect may raise some concerns as to the validity of a single measurement of the Lémann Index in patients at high risk of progression, since endoscopic activity and the assessment of mucosal healing are key aspects for CD prognosis.
29
Resolution of bowel damage after effective therapy on an extensive colonic Crohn’s disease treated by anti-tumour necrosis factor. After two years, there was a complete resolution of bowel damage in the affected colon.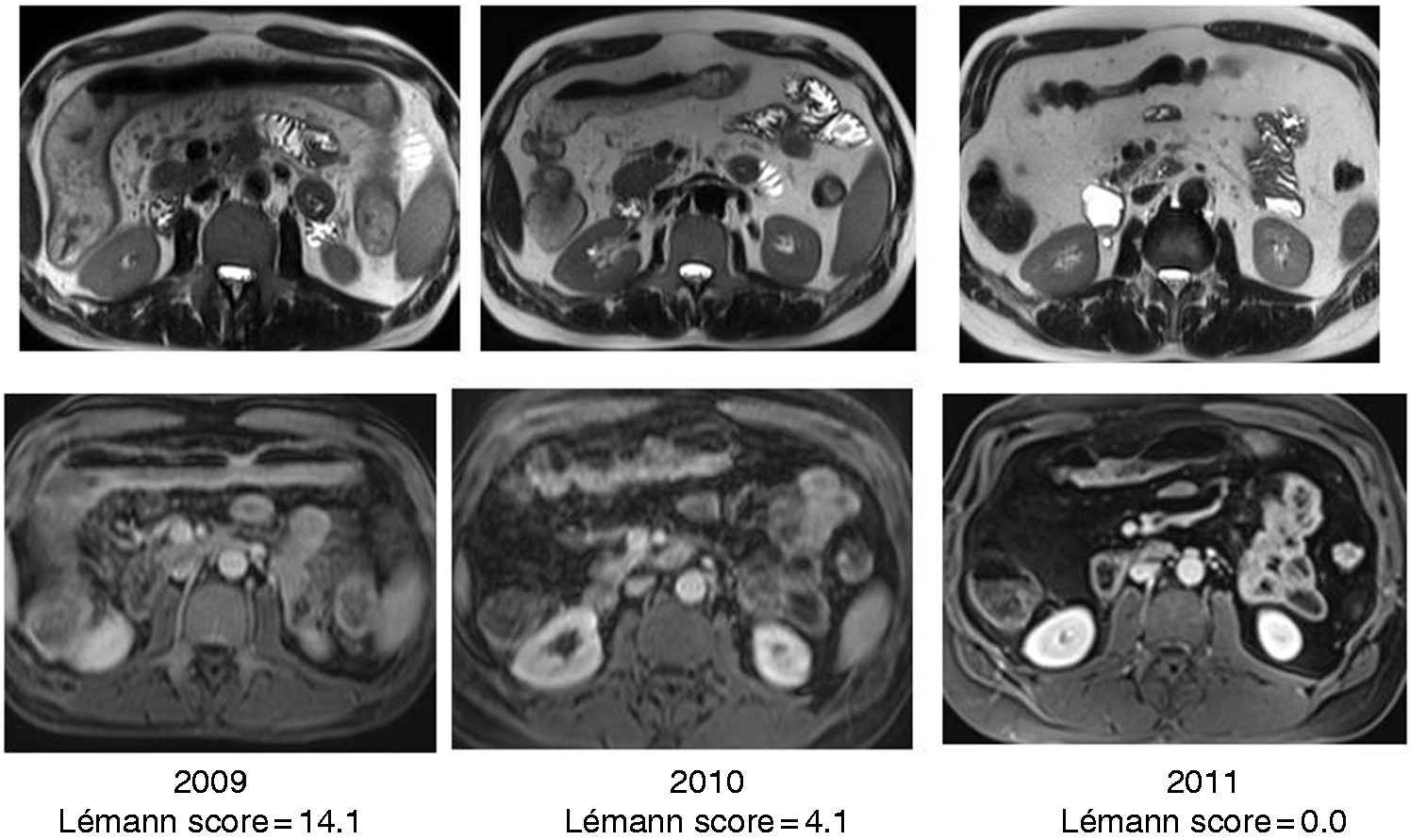
Several studies have shown that blockade of bowel damage progression measured by the Lémann Index could be associated with positive outcomes in the long term,29,31,32 although further research is needed. There are no validated cut-offs to discriminate the presence of bowel damage and clinically relevant changes over time. Gilletta et al. found that a score >2.0 was related to the presence of bowel damage, although this cut-off was calculated on patients undergoing surgery for complications. 28 Fiorino et al. propose a cut-off of 4.8, based on a blinded independent clinical evaluation by a gastroenterologist. 29 The same cut-off was used in further observational studies with similar results.31,32,35 Recently, Fiorino et al. 4 found that any unit of increase of the Lémann Index at diagnosis may be associated with negative course of disease, in particular with a significantly higher risk of hospitalisation and surgery, weakly confirming that probably the increase of the Lémann Index at two definite time points rather than a clear cut-off may be more useful in clinical practice and in further clinical trials.
Measuring bowel damage by the proposed indexes may be quite complex to be used routinely in clinical practice. The Lémann Index requires a combination of MRI (abdominal MRI, and pelvic MRI in the case of perianal disease) with endoscopy and surgical history, careful measurement of all the involved segments and a complex calculation of the final score. However, the recent study by Fiorino et al. 4 demonstrated that a simpler assessment of bowel damage, defined as the presence of any strictures, fistulas or abscesses, as previously proposed by the Paris Consensus on early CD definition, 38 predicts hospitalisation and surgery in newly diagnosed CD patients. This simpler approach may be more useful in clinical practice, limiting the measure and the quantification by the Lémann Index in selected patients where the accurate quantification of bowel damage may be crucial for therapeutic management, as well as a valid outcome measure in clinical trials.
There are several other gaps in the current evidence that should be addressed in further research. First, all studies cited in this review used the Lémann Index, even though it has not been validated. Second, the observation period in these studies was between 12 and 36 months, which can be considered quite a short period of time to see significant bowel-damage progression and the actual impact on the natural history of the disease. Third, the majority of the studies are retrospective and do not take into account the potential impact of the time of exposure to medical therapy on bowel-damage evolution. Finally, the definition of significant bowel damage probably needs some clarifications and adjustments. As an example, the LYRIC study 39 showed that limited ileocaecal resection in CD patients who failed conventional therapies has potentially the same benefits on patients’ overall quality of life than infliximab. In this case, limited structural bowel damage does not result in a negative course of disease and can be considered fully acceptable.
In conclusion, assessing and addressing structural bowel damage as a primary outcome may be the ultimate goal for the therapeutic management of IBD, at least in CD, together with quality of life and disability. 37 Further data are strongly needed to set clear outcome measures and to understand the impact of medications on bowel damage, and how this goal may impact on the natural history of disease. Moreover, further investigation is needed in patients with UC, especially with long-standing disease.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: G.F. received consultancy fees from Ferring, MSD, AbbVie, Takeda, Janssen, Amgen, Sandoz, Samsung Bioepis, Roche, Celltrion, Mylan. S.D. has served as a speaker, consultant and advisory board member for Schering-Plough, Abbott (AbbVie) Laboratories, Merck and Co, UCB Pharma, Ferring, Cellerix, Millenium Takeda, Nycomed, Pharmacosmos, Actelion, Alfa Wasserman, Genentech, Grunenthal, Pfizer, Astra Zeneca, Novo Nordisk, Cosmo Pharmaceuticals, Vifor, and Johnson and Johnson. The other authors have no conflicts to disclose.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.