
Abstract
Background
Coeliac disease (CD) is associated with an increased risk of other immune-mediated conditions.
Methods
Medical record data were collected retrospectively from 749 CD patients in Ireland. Prevalence of autoimmune diseases was compared with previously published results from general populations. Patients were divided into four groups based on the year of diagnosis to analyse changes in the prevalence of autoimmune thyroidal disease over time.
Results
Median age at the time of CD diagnosis was 56 years (range 18–91 years). A total of 233 (31.1%) patients had a coexistent immune-mediated condition (IMC). Autoimmune thyroidal diseases were seen in 149 (19.9%) patients, hypothyroidism in 110 (14.7%), type 1 diabetes in 27 (3.6%), psoriasis in 20 (2.7%), inflammatory bowel disease in 14 (1.9%) and rheumatoid arthritis in 12 (1.6%). All conditions were more common in CD patients than in the general population. Type 1 diabetes was diagnosed mainly before CD, whereas there was no such trend in other conditions. Autoimmune thyroidal diseases became less common in female CD patients over time.
Conclusions
Prevalence of autoimmune diseases is increased in adult CD patients compared with the general population. However, concomitant autoimmune thyroidal diseases became less common over time in women.
Keywords
Key summary
Summarise the established knowledge on this subject
Coeliac disease (CD) often coexists with other immune-mediated conditions IMCs. The main IMCs coexisting with CD are type 1 diabetes mellitus (T1DM) and autoimmune thyroid disease (ATD). A combination of shared genetic and potentially environmental factors plays a role in the co-occurrence of CD with other IMCs. Few data exist on the coexistence of CD with other IMCs in Ireland.
What are the significant and/or new findings of this study?
Of 749 CD patients, 31.1%had a coexistent IMC, the most prevalent being ATD, T1DM, psoriasis, inflammatory bowel disease (IBD) and rheumatoid arthritis (RA). The total number of T1DM and ATD cases was significantly greater than expected based on prevalence studies of similar populations in the literature. After controlling for the age of the patients at data collection, a significant decrease in coexistent ATD was observed in females over time.
Introduction
A recent systematic review has found the global prevalence of CD based both on serology and biopsy to be approximately 1%, with the condition being more common in females and children. 1 CD patients have a well established propensity to develop other immune-mediated conditions (IMC). 2 Therefore, patients with type 1 diabetes mellitus (T1DM) and autoimmune thyroid disease (ATD) are recommended to undergo CD screening due to the high co-occurrence of both conditions.3,4 Common genetic susceptibility variants presumably contribute to this phenomenon, and CD shares human leukocyte antigen (HLA) associations with both T1DM and ATD. In the case of T1DM, the two conditions also share over 30 overlapping non-HLA loci.5,6 CD shares non-HLA loci with many other inflammatory conditions, including prominently, inflammatory bowel disease (IBD) and rheumatoid arthritis (RA). 6
Common environmental exposures may also affect disease course and comorbidity. It has been suggested that gluten exposure in untreated CD patients may potentiate the development of CD-associated IMCs. 7 Thus, there seems to be a link between the amount of gluten intake in infancy and CD and T1DM development.8–10 Other environmental exposures, such as reovirus and enterovirus infections, may trigger the development of CD,11,12 and viral gastroenteritis has also been observed to increase the odds of developing IBD, which has significant comorbidity with CD. 13 In fact, the risk of developing IBD is greater not only in first degree relatives of CD patients but also in their spouses, indicating a mix of genetic and environmental factors predisposing to IMCs. 14 Shifts in environmental exposures are an obvious mechanism by which disease presentation may change over time, as observed particularly with the prevalence of ATD in our population.
The aim of the present study was to investigate the prevalence and timing of presentation of coexistent IMCs, as well as their burden, in a CD patient population in Ireland. Moreover, we have previously reported a reduction in ATD over time among CD patients diagnosed in adulthood, concomitant with an increased age at CD diagnosis. Thus, we wished to investigate this observation in greater detail, delineating the burden of ATD in our cohort, and the effect of factors such as the gender and age of the patients at data collection in our findings.
Methods
Study design and study population
A retrospective analysis of medical records was performed using a CD patient cohort (n = 749) attending five secondary referral centers in Ireland and diagnosed between 1960 and 2015. Patients with suspected CD are normally referred to secondary referral centres with expertise in CD diagnosis and management; our patients are therefore likely to be a relatively unselected and representative sample. The majority of the patients were identified based on their participation in a previous study on the genetics of CD. All patients are Caucasians of Irish ancestry; 79% of patients were diagnosed in the five participating referral centres, with the remainder diagnosed at other secondary referral centres. Data was collected from medical records, hospital information systems, and a structured questionnaire completed by the patient and the physician or research nurse for patients currently attending the coeliac clinic. All patients gave written informed consent. Patients were included in this and the earlier study based on positive CD diagnosis without other selective criteria. CD was diagnosed by serology and histology for the majority of patients. Serology included anti-Gliadin antibodies (AGA) for patients diagnosed during the 1970s to the 1990s; anti-tissue transglutaminase antibodies (tTGA) were introduced in the late 1990s and have since been the first-line screening method for CD diagnosis, together with anti-endomysial antibodies (EMA). Four patients were diagnosed before 1970 by biopsy and clinical follow up at primary referral centres (St James Hospital and University Hospital Galway). The study was approved by the Research Ethics Committees of St James's Hospital Dublin and all other contributing centres (REC reference 2010/07/10 and 2015-03 List 9; dated 28 July 2010 and 3 March 2015 respectively), and conforms to the ethical guidelines of the 1975 Declaration of Helsinki.
Data collection and definition of study variables
The following information was collected retrospectively; age at data collection, gender, age at diagnosis with CD, year of CD diagnosis, presence of coexistent IMCs, age at diagnosis with coexistent IMCs, and family history of other IMCs. Patient age at data collection was considered to be the age at last follow-up. The presence of the following CD-associated IMCs was determined in the study cohort; T1DM, ATD, RA, IBD and psoriasis. The presence of coexistent IMCs was corroborated in the medical records.
Statistical analysis
Prevalence of various IMCs among patients with CD.

Prevalence ratios (PRs) and relative timing of onset of immune mediated conditions (IMCs) in coeliac disease (CD) cases. Prevalence ratios are calculated using population prevalence data from the studies listed in column 1 and detailed in supplementary Table S1.
PR = Prevalence ratio; ATD = Autoimmune thyroid disease; T1DM = Type 1 diabetes mellitus; RA = Rheumatoid arthritis; SLE = Systemic Lupus Erythematosus; ND = Data not available.
To detect changes in the clinical phenotype of CD over time, a categorical variable was created for the year of diagnosis as follows; (a) before or during 1985, (b) 1986–1995, (c) 1996–2005, (d) during or after 2006. These time periods are similar to those of Kivelä et al. 17 and reflect the introduction of new CD diagnostic procedures. Thus, all biopsies prior to 1985 were jejunal capsule biopsies; from 1986 these were widely replaced by duodenal pinch biopsies. A modified EMA test and tTGAs were introduced in 1994 and 1997, respectively, substituting previously used AGAs.16,17
Statistical analyses were carried out using SPSS version 24.0 (SPSS, Inc., Chicago, IL). Discrete variables are presented as percentages, and continuous variables as medians and ranges. The relationship between discrete variables was analysed using the χ 2 test. Differences between groups were assessed using the Mann-Whitney U and Kruskall-Wallis H non-parametric tests. A threshold p-value of < 0.05 was considered significant in all analyses.
Results
General population prevalence studies and PRs
We compared the prevalence of selected IMCs in our cohort of CD patients with the prevalence of these IMCs in the general population, as reported by different studies conducted in the US or Europe (described in supplementary Table S1).
Table 1 confirms an increased prevalence of several IMCs in our patient population. The prevalence of ATD is significantly increased, with 149 cases observed versus 28.6 expected when compared with the meta-analysis by Garmendia Madariaga et al., corresponding to a prevalence ratio (PR) of 5.2 (95% CI 4.5–6.0). Both hypothyroidism and hyperthyroidism were increased, with PR 4.8 (95% CI 4.0–5.7) and PR 6.6 (95% CI 4.5–8.7), respectively. ATD is diagnosed equally prior to, at the same time as, or after CD diagnosis, and a female bias is observed.
For T1DM, we observed 27 cases compared with the 2.2 or 2.5 expected based on the PRs reported by Maahs et al. and Forouhi et al., giving PRs of 12.3 (CI 7.7–16.8) and 10.8 (CI 6.8–14.8), respectively. For IBD, 16 cases were observed compared with 2.2/6.2 expected, giving PR 7.3 (CI 3.7–10.8) and 2.6 (CI 1.3–3.8).
ATD is diagnosed equally frequently prior to, or at the same time as CD, compared with after CD diagnosis. T1DM, on the contrary, is diagnosed mainly before CD diagnosis. Females are more likely to be affected by all conditions except T1DM and ulcerative colitis.
Analysis of coexistent ATD for CD patients diagnosed in adulthood over four time periods
Analysis of the prevalence of co-existent ATD over time.
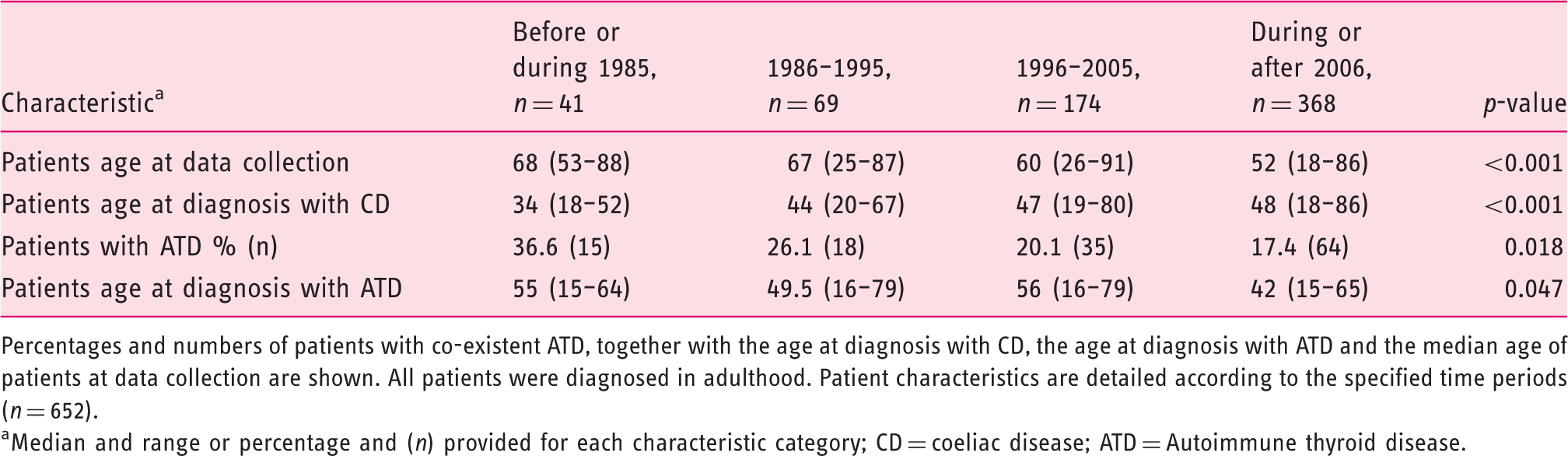
Percentages and numbers of patients with co-existent ATD, together with the age at diagnosis with CD, the age at diagnosis with ATD and the median age of patients at data collection are shown. All patients were diagnosed in adulthood. Patient characteristics are detailed according to the specified time periods (n = 652).
Median and range or percentage and (n) provided for each characteristic category; CD = coeliac disease; ATD = Autoimmune thyroid disease.
Analysis of the prevalence of co-existent ATD among CD patients over 55 years of age over time.
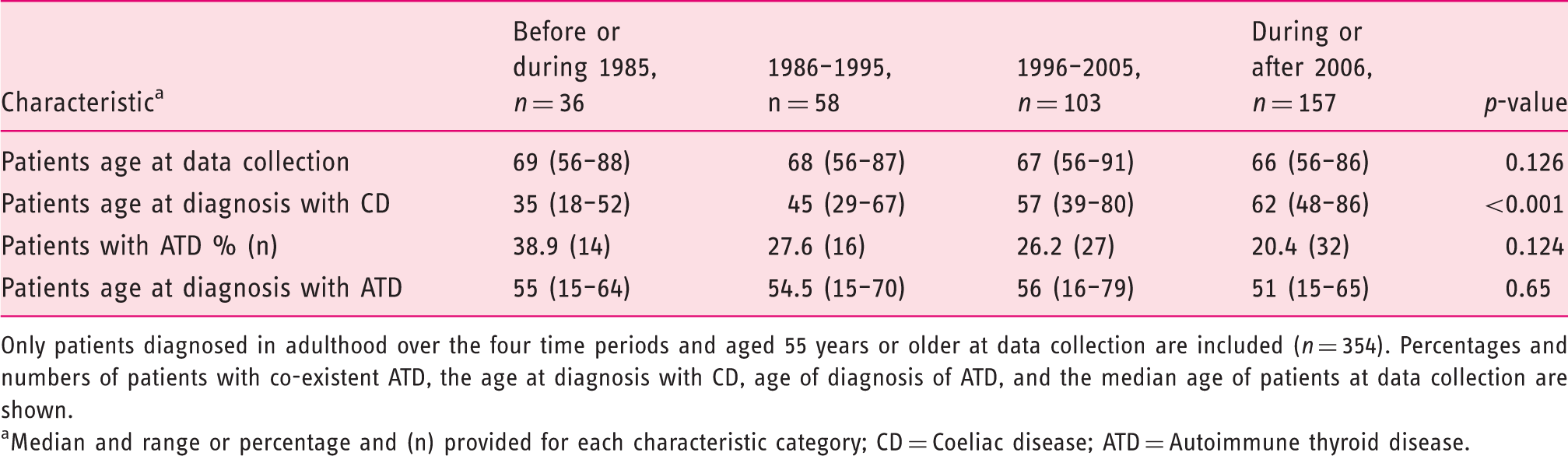
Only patients diagnosed in adulthood over the four time periods and aged 55 years or older at data collection are included (n = 354). Percentages and numbers of patients with co-existent ATD, the age at diagnosis with CD, age of diagnosis of ATD, and the median age of patients at data collection are shown.
aMedian and range or percentage and (n) provided for each characteristic category; CD = Coeliac disease; ATD = Autoimmune thyroid disease.
Data for those aged >55 years at data collection are shown in Table 3. A total of 89 patients had coexistent ATD; 79 of these were female. A non-significant trend towards less coexistent ATD over time was again observed, falling from 38.9% before or during 1985 to 20.4% during or after 2006 (p = 0.124) (Table 3). However, when stratified by gender, ATD decreases significantly in female patients, from 65% before or during 1985 to 28.9% during or after 2006 (p = 0.01; not significant in males p = 0.44) (Figure 1). Patient age at data collection is similar over the four time periods (decreasing from 69 to 66 over time) (p = 0.126). The age at ATD diagnosis is also stable (p = 0.65). Thus, we observe a decrease in the prevalence of coexistent ATD over time in the overall group, and also when controlling for age, where there is a significant reduction among females (Figure 1).
Prevalence of coexistent ATD for female CD patients diagnosed in adulthood and >55 years at data collection divided into four periods according to the year of diagnosis (n = 226).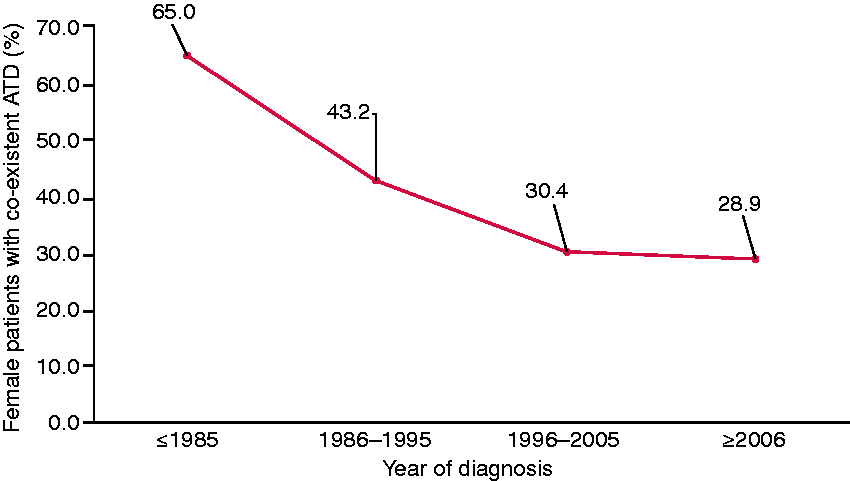
Discussion
The prevalence of coexistent IMCs among CD cases in this study is 31.1%, in line with previous findings. 18 This is significantly greater than the estimated prevalence in the general population of these IMCs of 3–9.4%. 19 As with similar studies in adult CD, we find the most common coexistent IMCs are T1DM and ATD. 18 The total number of T1DM (n = 27) and ATD (n = 149) cases we observed among our CD population was higher than expected based on prevalence studies in the literature. The PRs and 95% CI values we obtain for T1DM and ATD are in line with those found in a comparable analysis of a North American CD cohort. 15 We found that, in the majority of cases, T1DM precedes CD, whereas ATD, IBD, RA and psoriasis occur equally either prior or at the same time than after CD diagnosis, in agreement with other studies (Table 2). 15 Active screening for CD in patients with T1DM, and the overt and life-threatening presentation of T1DM, probably contribute to T1DM detection prior of CD.
We confirm previous reports that ATD is observed frequently with CD, as well as having a pronounced female bias. 20 The total number of cases of ATD (n = 149) observed equates to an ATD prevalence of 19.9% (14.7% for hypothyroidism and 4.9% for hyperthyroidism), which is somewhat higher than those found in other studies in CD patients. Volta et al. reported a prevalence for hypothyroidism of 13%, while Neuhausen et al. reported 10.3%.15,18 We also report for the first time a significant reduction in ATD over a 55-year period, which is still present when controlling for the age of patients at data collection (Tables 2 and 3). In this subgroup, who were >55 years of age at data collection, ATD decreases significantly for women, known to be at higher risk of developing ATD than men (Figure 1). Our data also suggests a shift in timing of presentation of CD relative to ATD; CD presents before ATD in earlier periods and after ATD in later periods (Tables 2 and 3). However, this observation may be an artifact of the retrospective nature of this study and would need to be investigated prospectively.
Shared susceptibility genes seem to be a logical explanation for the coexistence of IMCs. Indeed, HLA DR3, DQ2 and DQ8 are associated with T1D, ATD and CD, and are the primary genetic drivers of comorbidity, although particular combinations of HLA alleles are associated with comorbidity, which may differ from each disease individually.5,21 Gutierrez-Achury et al. found no significant evidence that non-HLA susceptibility loci are a factor in the coexistence of T1DM and CD (despite the large number of these shared by the two conditions), although CTLA4 and IL2RA are associated with double autoimmunity. 5
We observe a decrease in the levels of comorbid ATD in our case population against a backdrop of static ATD incidence generally, and increasing incidences of CD and T1DM.22–24 It may be that among the increasing numbers of CD patients, the genotype is changing and is unfavorable for the development of ATD, and/or that environmental factors are changing. There is some evidence for this conjecture: the proportion of newly diagnosed T1DM patients with a higher risk HLA susceptibility genotype has decreased over time—especially in younger patients. 25 These findings suggest a role for environmental factors, which are now able to cause the development of T1DM on a genotypic background that would not previously have been sufficient to cause disease. 25 Thus, the opposite may be true for ATD in a CD population, i.e. that the pool of patients developing CD is increasingly composed of individuals predisposed only to CD and not to ATD, which may be influenced by unknown variation in environmental exposures.
Increased awareness of CD resulting in earlier diagnosis may be causing a decrease in ATD due to reduced long-term exposure to gluten and/or tTGAs. Naiyer et al. observed how tTGAs bind to tissue tranglutaminase II in thyroid tissue, and that tTGA titres correlate with those of antithyroidperoxidase antibodies. 26 Although they did not show proof of thyrocyte damage, this suggests that tTGA deposition could lead eventually to thyroid dysfunction. 26 However, studies exploring ATD development in CD patients have failed to see any protective effect of the GFD,20,27 which does not necessarily exclude gluten as a causative factor. Convincing evidence does exist implicating dietary gluten in the development of T1DM, which could thus contribute to the incidence of T1DM/CD comorbidity. 10 If gluten reactivity does precipitate ATD, the general observation that CD is increasingly of older onset as also seen here (mainly observed in groups >45 years of age) may be a more plausible explanation for decreased incidence of ATD in this population, 28 in that at risk individuals may have a lower gluten load during their lifetime. 29
There is a significant increased risk of coexistent IBD in our cohort, with an IBD prevalence of 1.9%, and PRs 6.4 and 2.3 for study 1 and 2, respectively (Table 2). This is in line with similar studies that have reported a prevalence range 2.2% to 3.3%, or a range of 2- to 10-fold increased risk of patients with CD having coexistent IBD. 30 Both diseases also share common potential environmental factors involved in disease initiation such as viral infections.12,31 This is supported by familial studies that have found an increased risk of developing IBD not only in first degree relatives of coeliac patients, but, curiously, also in their spouses. 11 It is notable that, similar to T1DM and CD, IBD incidence is increasing worldwide. However, unlike CD, for T1DM and IBD the increasing incidence is affecting more children.24,32
Although we observe an increased risk of coexistent RA in our CD patient cohort, only the 95% CI for study 2 is significant (Table 1). Unlike us, Neuhausen et al. 15 have shown lesser risk of developing coexistent CD in RA patients and RA in CD patients, respectively. Although RA can occur at any age, its prevalence increases with age and incidence has been increasing in recent decades in women >50 years of age. 33 Therefore, the fact that our sample is older and female biased could be inflating our results. In the case of psoriasis, study 1 yielded an increased psoriasis risk of 1.7 in our patients which was borderline significant (95% CI: 1.06–2.7) (Table 2). A recent systematic review with meta-analysis has reported a 3-fold increase in the risk of developing CD in patients with psoriasis. 34
Strengths and Limitations
This is the largest study on CD clinical presentation over a lengthy period of time conducted in the Republic of Ireland. To our knowledge, few studies internationally have examined such an extended time frame in the adult CD population. The observed significant changes in coexistent ATD in a country with historically high CD detection rates, expands current knowledge about the evolution in CD presentation.
Two of the main limitations of this study are that it is retrospective and that it has used a convenient sample, which could lead to selection bias; however, the fact that the participating centres are secondary referral centres, means that our sample should be broadly representative of patients both geographically and in terms of disease severity, mitigating potential selection bias. The associations observed between CD and other IMCs, although in line with those found in similar studies, could be the result of detection bias, which may be resolved only with population screening studies. The lack of a control group is also a limitation, as the studies we have used are based on the general population, which does not rule out people with CD. Changes in the diagnostics and awareness/screening of CD could potentially have resulted in only sicker patients being diagnosed in the past, or some patients being incorrectly diagnosed in the earlier periods; however, all our cohort of patients have been extensively followed by physicians and nurses with expertise in CD. Moreover, many studies have proven a true increase in the incidence of CD as well as a change in its clinical presentation over a time period similar to the one considered in our study, which cannot be explained solely by improved diagnostic techniques.17,23
Conclusion
Our results support previous findings that CD patients have an increased occurrence of IMCs, and describes the prevalence of the most common of these in Ireland. ATD is the most common IMC, but is declining at a remarkable rate over the 55-year time frame of this study. Our findings support existing evidence that the prevalence and presentation of several IMCs, and CD and ATD in particular, are in a state of flux, with important implications for diagnosis and treatment.
Supplemental Material
UEG899225 Supplemental Material - Supplemental material for Prevalence of coexisting autoimmune thyroidal diseases in coeliac disease is decreasing
Supplemental material, UEG899225 Supplemental Material for Prevalence of coexisting autoimmune thyroidal diseases in coeliac disease is decreasing by Patricia Dominguez Castro, Grace Harkin, Mary Hussey, Brian Christopher, Clifford Kiat, Jun Liong Chin, Valerie Trimble, Deirdre McNamara, Padraic MacMathuna, Brian Egan, Barbara Ryan, David Kevans, Mohamed Abuzakouk, Richard Farrell, Con Feighery, Valerie Byrnes, Nasir Mahmud and Ross McManus in United European Gastroenterology Journal
Footnotes
Acknowledgements
The authors would like to thank Lina Zgaga from the Department of Public Health and Primary Care in Trinity College Dublin for her comments and advice. They also thank all patients for providing the information necessary for this study, and all the administration staff in the participating hospitals for their help retrieving patient data.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
The study was approved by the Research Ethics Committees of St James’s Hospital Dublin and all other contributing centres (REC reference 2010/07/10 and 2015-03 List 9; dated 28 July 2010 and 3 March 2015 respectively), and conforms to the ethical guidelines of the 1975 Declaration of Helsinki.
Funding
Work performed at the Trinity Centre for Health Sciences, St James’s Hospital, Dublin 8, Republic of Ireland. The authors declare no conflict of interest. This research was funded by Trinity College Dublin with a Postgraduate Ussher Fellowship; no other specific grant from any funding agency in the public, commercial or not-for-profit sectors was received. R. McManus is funded by an SFI principal investigator award (09/IN.1/B2640). All authors approved the final version of the paper.
Informed consent
All patients gave written informed consent.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.