
Abstract
Background
A gluten-free diet (GFD) is currently the only available therapy for coeliac disease (CD).
Objectives
We aim to review the literature on the GFD, the gluten content in naturally gluten-free (GF) and commercially available GF food, standards and legislation concerning the gluten content of foods, and the vitamins and mineral content of a GFD.
Methods
We carried out a PubMed search for the following terms: Gluten, GFD and food, education, vitamins, minerals, calcium, Codex wheat starch and oats. Relevant papers were reviewed and for each topic a consensus among the authors was obtained.
Conclusion
Patients with CD should avoid gluten and maintain a balanced diet to ensure an adequate intake of nutrients, vitamins, fibre and calcium. A GFD improves symptoms in most patients with CD. The practicalities of this however, are difficult, as (i) many processed foods are contaminated with gluten, (ii) staple GF foods are not widely available, and (iii) the GF substitutes are often expensive. Furthermore, (iv) the restrictions of the diet may adversely affect social interactions and quality of life. The inclusion of oats and wheat starch in the diet remains controversial.
Introduction
Coeliac disease (CD) is the intolerance to wheat, barley, rye and triticale that occurs in the region of 1/100 individuals in the Western world, in genetically predisposed individuals. 1 The disease is characterized by villous atrophy, small intestinal inflammation, i.e. increased number of intraepithelial lymphocytes (IELs), and increased level of CD-specific serology. 2 Patients with CD who avoid gluten usually experience improved symptoms with healing of the intestinal mucosa. 3 Similarly, patients affected with dermatitis herpetiformis (DH) when on a gluten-free diet (GFD) experience healing of the skin and any gut lesions. 4
The transition from a regular gluten-containing diet to a GFD is the first therapeutic intervention towards improved health after diagnosis of CD. At present, a strict GFD must be considered a lifelong treatment and patients should be seen by a dietitian at the time of diagnosis and offered follow-up to provide ongoing assessment, knowledge update and support. 5 To ensure improvement it is important that patients learn about foods to avoid, maintain a healthy diet, and that compliance is monitored. Inclusion of gluten-free (GF) oats and wheat starch-based products has been controversial over the years, and is discussed in detail below. This paper aims to provide a comprehensive review of the GFD in CD.
Methods
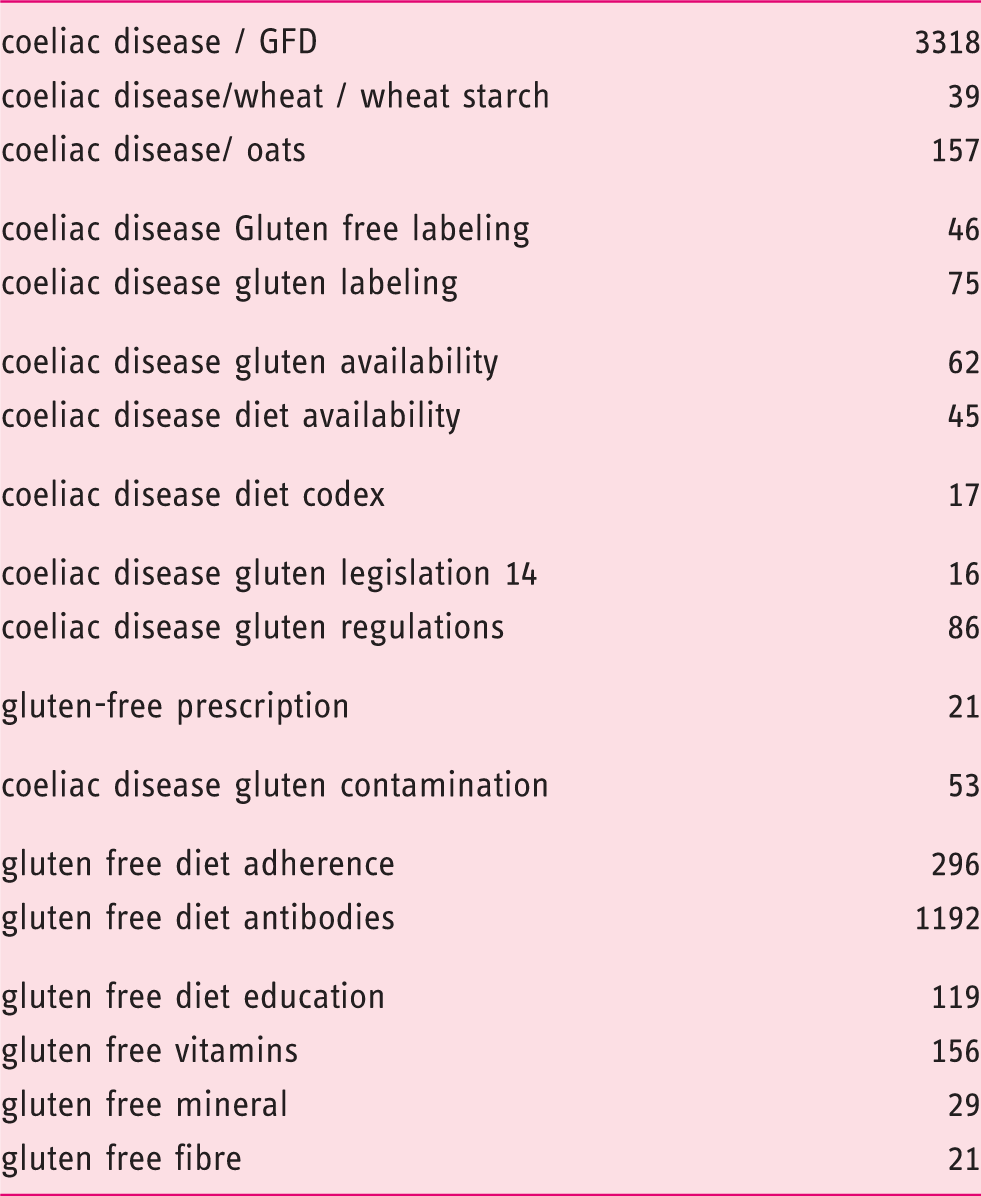
PubMed search: number of hits (years 1900–September 2014)
The gluten-free diet
A GFD has been the mainstay of treatment of CD since the 1950s. 6 Initially, wheat and rye flours were excluded from the diet of coeliac patients,6,7 with barley excluded later. 8 Following the work of Dicke in the 1950s, 6 oats were also withdrawn from the GFD, although the effect of oats in CD has been controversial and will be discussed below.
The term ‘GF’ (gluten-free) relates to the composition of GF foods and is now defined by law in Europe and North America; it denotes food without the storage proteins of wheat (gliadins and glutenins), barley (hordeins) and rye (secalins) and cereal hybrids such as triticale (Figure 1).
Classification of grains: Toxic grains for coeliac patients include bread wheat, durum wheat (used in pasta), spelt wheat, polonicum (Polish wheat), Kamut, monoccum (einkorn), farro, triticale (a cross between wheat and rye), and many other wild grass. They all belong to the Hordeae or Triticeae family. The grasses not in Triticeae are classified as safe (rice, corn, various millets, ragi, teff, oats). Protein sequence between the major wheat gliadin proteins and oat avenins indicates relative closeness of wheat and oats. From: Kasarda DD 2003. Celiac disease and safe grains. http://wheat.pw.usda.gov/ggpages/topics/celiac.vs.grains.html with the permission of the author.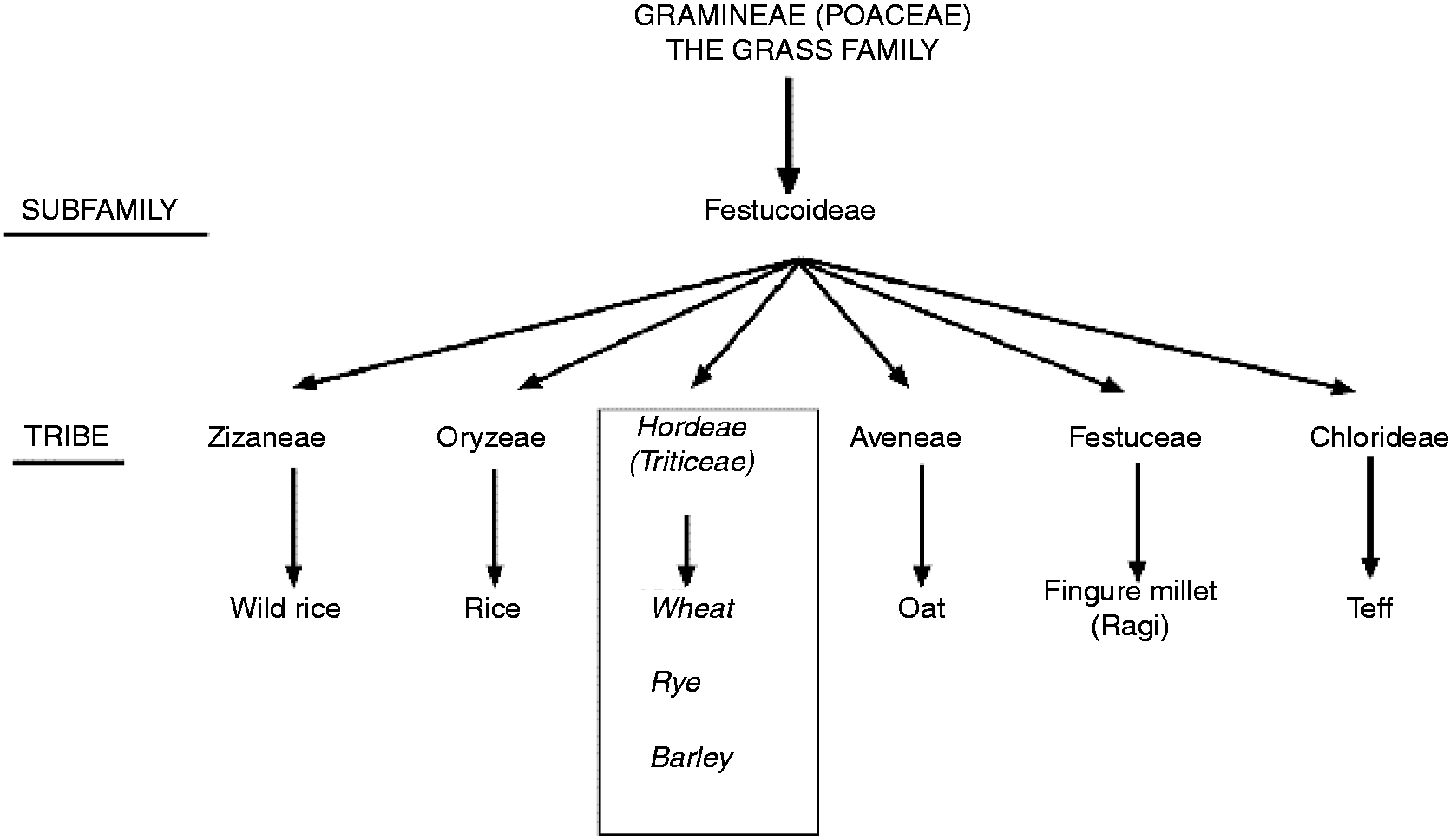
There are three main aspects to the GFD:
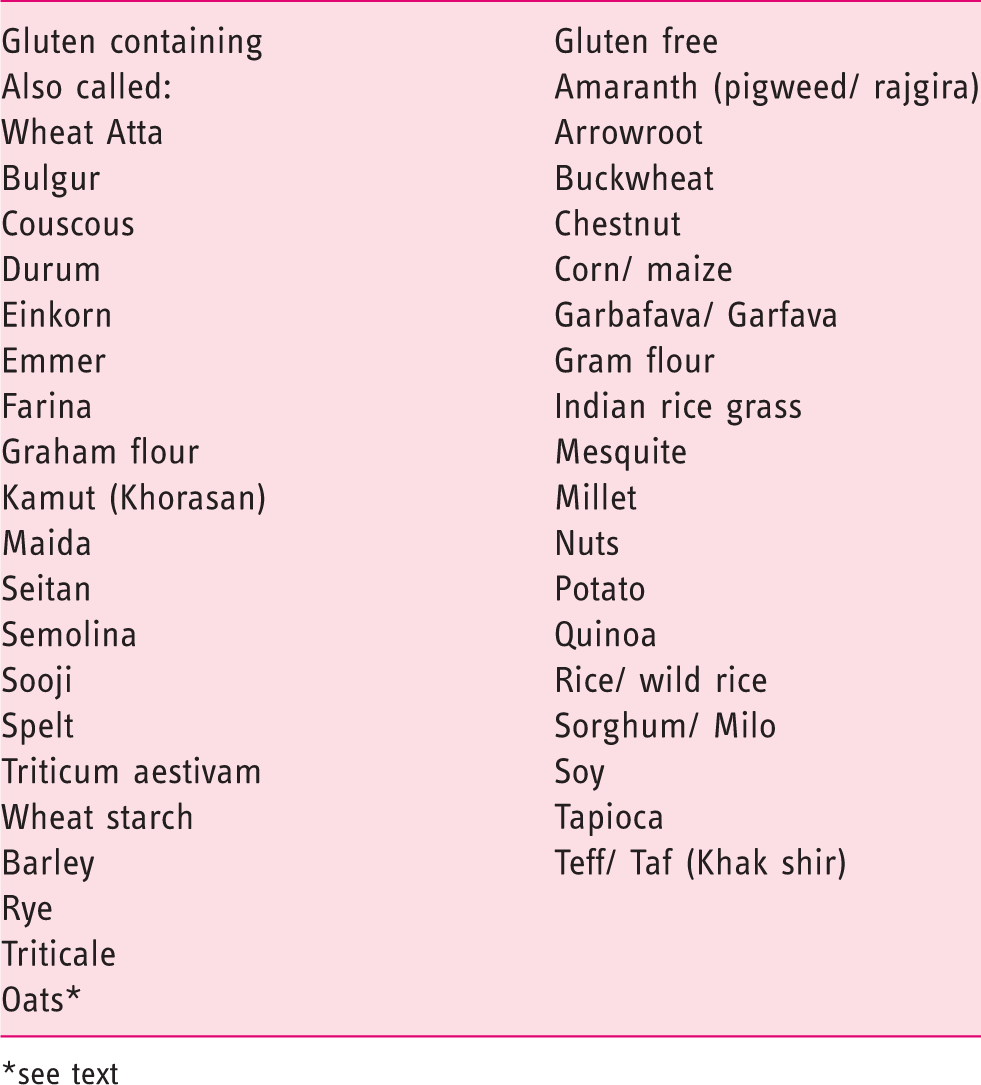
avoiding cereals and products containing gluten such as bread, breakfast cereals, flours, pasta, cakes, biscuits, sauces, etc., derived from wheat, barley, rye or uncontrolled/contaminated oats. eating naturally occurring GF foods and alternative sources of starchy foods such as rice, potatoes, corn and sorghum.
9
(see Table 2). using commercially prepared GF substitutes foods, available to buy or on prescription in some countries. Grains, seeds and other starch sources see text
Patient education
There is a lack of data on the optimal timing and amount of information patients require to understand the condition. It is recommended that information about a GFD is provided by the doctor or dietitian at the time of diagnosis. 10 Immediately after diagnosis some patients may feel overwhelmed and unable to cope with a large amount of information. However, inadequate advice at this stage may lead some patients to seek answers from less reliable sources, as there are currently many information sources available for patients in the form of leaflets, books and internet sites. 11 A useful approach is to offer a follow-up consultation shortly after diagnosis, to allow patients to ask questions and clarify issues regarding diet and health.
Being well informed about the GFD is the key to successful CD management, and we can postulate that knowledge of the disease and gluten content of food are essential factors for dietary compliance. Children’s compliance to a GFD has been linked to parental knowledge and understanding of the disease, and with the socioeconomic status of the families. 12 A recent study indicates that in a paediatric setting, parental information at time of referral for biopsy about GFD as the only therapy for CD was excellent, although specific dietary information was lacking, with only 30% correctly identifying all the gluten-containing foods. 13 In adolescents and adults compliance relates to the level of knowledge of CD.14,15
A clinic with a dietitian and nurse dedicated to CD management seems to improve patients’ satisfaction. 16 However, a recent study suggests that there is no improvement in diet adherence, nutritional indices and quality of life scales between patients who are referred to a dietitian and those who do not have the chance to meet with a dietitian. 17 Further studies are needed in large numbers of patients to address this point. In the meantime we recommend consultation with a dietitian.
Newly diagnosed coeliac patients should be referred to a dietitian to discuss dietary management. As well as avoiding gluten and use of alternative products, it is important to include an assessment of nutrients, vitamins, fibre and calcium content of the diet. Patients with weight loss prior to the diagnosis of CD may require help and support to add weight, while others may require advice on weight management as part of a healthy diet.
The consultation requires an explanation of the principles of the diet plus written information. Patients should be encouraged to join their National Coeliac patient support group. In the UK, patients should be advised about access to GF staple items on prescription (FP10), details of which are available from www.coeliac.org.uk.
CD is a chronic illness. Having a chronic disease, the treatment of which is a lifelong change in diet, significantly influences the patient’s lifestyle. Several studies have reported reduced quality of life because of dietetic restrictions.18–20 This may be particularly true when diagnosis is made after screening in patients with few or no symptoms. A possible explanation for the lack of improvement in this patient group is that screening-detected individuals perceive few, if any, symptoms. To them a strict GFD may instead reduce quality of life. 10
One of the most frequent complaints of patients with CD is the fact that their social life, and in particular eating out or travelling, is limited because of the worry of not finding GF food or of eating food contaminated with gluten. To overcome these concerns requires education not only of the patients but those involved in the catering industry in schools, hospitals, working places, and restaurants.
Is there a ‘safe’ amount of gluten for patients with coeliac disease?
Treatment of CD and DH relies on avoidance of wheat, barley and rye; however, in practice this is extremely difficult, if not impossible, to achieve for most patients. Since the early 1980s there has been much research into maximum safe limits for gluten.
Current controversies and difficulties include: Possible variation in level of sensitivity among coeliac patients – does one size (level) fit all? Accuracy of measurement of gliadin/glutenin/hordein/secalin proteins within foods and accuracy of methods for measuring hydrolysed prolamines. Variation in quantities of GF substitute foods consumed by different patients/nationalities, etc. Best methods of assessment of ‘toxicity’ – clinical, histological or serological?
Intraduodenal infusion of 10 mg of gliadins21,22 did not influence the mucosa in biopsies taken 2–3 hours after infusion, 100 and 1000 mg had a transient impact on histopathology (with reversal of effects by 72 hours). Ingestion of GF bread containing 2.4 g of gliadin daily for 6 weeks was associated with diarrhoea in 4 of 10 patients but no differences in biopsies or 51 Cr-EDTA excretion. 22 Catassi et al. 23 showed an increase in IELs after 100 mg/day of gliadin added to a GFD in children. Montgomery et al. 24 compared biopsies taken from 12 adults following a strict GFD with 13 on a low-gluten diet (2.5–5 g/day) and found no differences in anti-gliadin antibodies (AGA) or villous height or crypt depth, but a significant increase in IELs in the low-gluten group.
A double-blind placebo-controlled trial of gluten challenge in adults 25 (3 months with placebo or 10 or 50 mg gluten/day) showed that no significant effect was seen with 10 mg/day but small intestinal biopsies showed changes in most exposed to 50 mg/day. More recently, a 14-day gluten challenge at >3 g of gluten per day was able to induce histological and serological changes in the majority of adults with CD participating in the study.26,27
It is clear that there is a wide variation in sensitivity between patients, but a systematic review of the papers dealing with this topic and recent data indicate that a safe daily limit is probably in the region of 10 mg.25,27 However, all patients should be encouraged to be vigilant with their diet and avoid all sources of known gluten or contamination which may occur during food preparation.
There are no studies examining what constitutes a safe daily amount of gluten in coeliac patients presenting with extraintestinal manifestations such as ataxia and peripheral neuropathy.
Oats in the gluten-free diet
The potential advantages of incorporating oats in a GFD relate to the additional nutritional benefits, contributing a source of soluble fibre with its associated benefits, lowering post-prandial blood glucose with attenuated insulin response and lowering low-density lipoproteins. They are also a source of protein, minerals and vitamins. The addition of oats to a GFD increases product choice; however, the use of oats has been highly controversial over the years and was formalized in 2008 by the revised Codex standard for gluten.
One gram of oats contains approximately 13 mg of prolamis (avenins), but these make up a lower share of protein than other cereals (about 13% in oats compared with 35% in wheat). They have about half the quantity of proline residues. The results of studies including oat products have been complicated by the fact that many oat products are contaminated with gluten-containing cereals. When Hernando et al. 28 analysed 134 oat grains and products, only 25 were uncontaminated. There also appears to be variability in the response of patients to oats, with a subset of patients demonstrating intolerance to uncontaminated oats. 29
The finding of IgA antibodies to avenin in untreated coeliac patients was thought to be due to a generalized immune response due to abnormal mucosal permeability and not evidence of a harmful effect of oats. 30 However, the in vitro study by Arentz-Hansen et al. 29 yielded avenin-reactive T cells in organ culture from five of nine oat-intolerant patients.
A small number of clinical trials have examined the effect of oats on symptoms, small bowel histology or serology. 31 However, limitations to these studies include lack of accurate assays for prolamins, particularly hordeins, and hence unknown levels of contamination, variations in antigenicity between oat cultivars, 32 small numbers, short periods of challenge and follow-up, and lack of details about withdrawals.
A systematic review of oats 33 used in clinical trials reported that 11/170 (6%) adults and 8/89 (9%) children withdrew because of adverse, mainly gastrointestinal, side effects. It is unclear whether withdrawals were due to oat intolerance or to other causes. One recent study that examined the ingestion of daily oats in 46 patients (286 g/week) for 1 year found no significant histological or serological changes. 34
The conclusions from various systematic reviews33,35,36 were that 50–70 g of oats/day for adults and 20–25 g/day for children are probably within safe limits for most provided they are from a pure, uncontaminated source. However, a recent study by Tjellstrom et al. suggests that oats affect gut microflora function in children, and in some can be associated with gut mucosal inflammation. 37
Also, a small proportion of patients may exhibit intolerance to oats, and oats should therefore only be introduced when the GFD is well established so that possible adverse effects are identified. The long-term risks of consuming oats in CD remain unknown.
The interpretation of data of oat tolerance in CD has varied worldwide. In general, Scandinavian countries have considered uncontaminated oats as acceptable; the Association of European Coeliac Societies (AOECS) does not have an official opinion, with individual countries applying their own recommendations. In America oats are considered to suffer from significant contamination and patients are therefore advised not to eat them. 38 Coeliac societies in Romania, German and Italian-speaking Switzerland, South Africa and New Zealand do not recommend oats. 39 In Canada, however, pure oats are now being produced and are considered safe. 40
Far from helping in decision making, current data shows that incorporating oats into a GFD is a more complex issue than previously suggested. Further work is required on development of oat cultivars with low avenin content or low immunogenicity, along with guidelines for the manufacture and processing of oats, accurate assays to detect avenins in oat products, long-term follow-up of patients consuming oats and also identification and follow-up of those with ‘oat intolerance’.
Codex wheat starch
Wheat starch prepared to be compliant with the international Codex standard for gluten-free labelling purposes (Codex wheat starch) has been used in Northern European countries as the basis for production of GF flour-based foods to improve baking quality and texture.
In 2008, the Codex Alimentarius Commission of the World Health Organization set new benchmarks for producing GF foods. Based on these guidelines the European Commission issued a law on the labelling of food for people who are gluten intolerant, which came into full effect in January 2012.41,42 This regulation defines that foods that contain 20 ppm gluten (20 milligrams of gluten per 1 kilogram of food) or less can be labelled as ‘gluten-free’. This applies both to naturally GF products (e.g. maize, rice, buckwheat) as well as products containing wheat starch. The GF label may also be used for pure, uncontaminated oat products (containing ≤ 20 ppm gluten). Of note, even though the term ‘gluten-free’ implies no gluten, in clinical practice with current methods it is impossible to test for a zero level of gluten. Furthermore, despite the unanimous view that GFDs should be as strict as possible, a diet completely devoid of gluten (with zero gluten) would be difficult if not impossible to implement, as the products on the market may contain trace amounts of contaminating gluten.43–45 However, research has shown that people with CD appear to tolerate these very low levels of gluten safely.25,46–48 It should be also remembered that before the revised Codex standard for gluten, patients with CD in Scandinavia and the UK consumed wheat starch-based products containing gluten traces of up to 200 ppm without any evidence of a deleterious effect on small bowel mucosal morphology or morbidity.49–53
The 20 ppm standard for labelling of GF products is also applied in the USA. The Food and Drug Administration (FDA) introduced the Food Allergen Labeling & Consumer Protection Act in 2006, and recently approved that GF labelling can be voluntary used for any food product under 20 ppm gluten (https://www.federalregister.gov/articles/2014/06/26/2014-14929/small-entity-compliance-guide-gluten-free-labeling-of-foods-availability).
Measurement of gluten in foods
To meet the requirements of the regulations for GF food 54 and to guarantee accurate food labelling, reliable analytical methodology for proper quantification of gluten is necessary. The new Codex standard indicated that enzyme-linked immunosorbent assay (ELISA) R5 by Mendez is currently the official standard for measuring gluten levels in food.41,42 The monoclonal antibody used in the ELISA assay recognizes the pentapeptide QQPFP, and homologous sequences that occur repetitively in the prolamins from wheat, rye and barley. 55 A high accuracy and repeatability of the test has been shown, but the test has some important limitations. For instance, it fails to detect barley contamination in oat products, hydrolysed gluten peptides (in beer, wheat-based starch hydrolysates and syrups), high-molecular weight glutenins of wheat, and low levels of gluten.56–60 To overcome these problems, the development of new, more accurate tests to detect gluten contamination in food is currently in progress.57,61–63
When gluten detection tests were developed, it was found that not only oats,38,64,65 but also many commercially available naturally GF products (e.g. rice, maize and buckwheat) may be contaminated by gluten.43–45 Inherently GF grains, seeds and flours can be contaminated with wheat, rye and/or barley while being harvested, transported and processed. These inherently GF products are widely consumed by coeliac patients, and the contamination of these products may lead to inadvertent gluten intake while on a GFD. This is an important issue, as according to the literature, some patients with long-term treated CD may still have abnormal small bowel mucosa despite an apparently strict GFD;66–70 it is known that ongoing small intestinal damage may predispose the patients to complications of CD (e.g. increased mortality, osteoporosis and fractures).71–74
Economics of the gluten-free diet
In the UK, in Italy and in some other European countries, people medically diagnosed with CD may access GF staple foods on prescription from their national health service. In the UK, supermarket chains have a greater availability, whereas budget supermarkets and corner shops rarely have gluten-free products; the cost is, however, greater than regular similar products.75,76 By contrast, in the USA GF products are mostly available in special health food stores and on the internet, and less commonly in grocery stores. 77 The differences may be explained by the difference in health service support but also by the variability in distribution of specialty food in different countries. Limited access to GF food products, and the increased cost of such products compared with their gluten-based counterparts, may affect compliance to the GFD.75–77 Furthermore, adhering to a GFD may potentially lead to a nutritionally deficient diet compared with a regular diet (due to non-compliance or selective choice of foods 78 ), this requiring further supplementation of the diet with vitamins and fibre supplements, which again adds to the cost of adhering to the diet.79,80 Following a strict GFD requires constant vigilance by the patient with CD, and it has been suggested that an average person with CD spends an extra 10–20 hours per month checking food labels for gluten content. 81 Moreover, patients need to be cautious when eating out, as awareness of GF food can be variable among caterers. 82 All in all, these issues may reduce the adherence to the diet and decrease the quality of life of patients with CD.10,83–85 Government support by prescriptions or monthly allowances may ease the economic burden of CD; 86 unfortunately, such support is not available in all countries.
Nutritional content of the gluten-free diet
There is limited information available on the nutritional adequacy of the GFD and the composition of specialist GF products. A systematic review of the evidence was published by the UK Food Standards Agency in 2009 concluding that insufficient data precludes any conclusions to be drawn on the nutritional composition of a GFD compared with a gluten-containing diet (http://www.food.gov.uk/science/research/allergy-research/t07053).
GF products provide 36% of daily total energy; however, often the lack of nutritional information for GF products has limited dietary analysis. 87 Studies from the Netherlands, Germany, Australia and the UK have shown inadequate vitamin and mineral intake in newly diagnosed 88 and treated adults.79,89,90
One recent study of 18 coeliac children showed higher carbohydrate and lower fat intake in the coeliac patients compared with controls. 87 Another study showed that in adults GFD increases cholesterol levels, 91 and other studies suggested that GFD affects homocysteine levels.92,93 These findings taken together may imply that GFD has the potential to increase cardiovascular risk. However, no definitive evidence confirms the hypothesis. 94
It is recommended that patients should be screened for nutritional deficiencies, such as iron deficiency anaemia and vitamin deficiencies, both at diagnosis and at annual review. 79 However, there are no follow-up studies addressing the long-term clinical and financial implications of such a protocol.
Calcium is essential for forming and maintaining bone mass. However, a study into the effect of calcium and vitamin D supplementation on reduction of fractures in the general population gave conflicting results. 95 It has been demonstrated that 1 year of untreated CD was associated with a bone mass density decrease at the lumbar spine of 0.00570 g/cm2. 96 Currently the recommended daily intake of calcium for patients with CD is 1000–1500 mg, but the question of whether calcium supplements are necessary in coeliac patients and, if so, whether they are necessary for all age groups, remains unanswered. Achieving the recommended intake of calcium for adults with CD and low bone density or osteoporosis requires assessment, support and ongoing advice. 97
Long-term maintenance of the GFD is pivotal in optimizing absorption. Patients who are found to have problems adhering to the GFD, whether through antibody screening, repeat biopsies or diet history, may require more intensive dietary counselling from a dietitian on a more regular basis.
Patient follow-up
There is wide variation in the follow-up of patients after diagnosis, with some receiving no medical input and others offered regular appointments at a specialist coeliac clinic. However, a number of studies confirm that follow-up is necessary15,98 to reinforce the need to adhere to the GFD and obtain mucosal healing that is linked to reduced risk of complications.5,99
Dietary compliance is the key to achieve mucosal healing and relief from most gastrointestinal symptoms. Voluntary or involuntary gluten intake can sometimes be revealed by increased serum levels of anti-transglutaminase IgA antibodies. 100 However, there are no specific biomarkers to adequately assess the mucosal degree of inflammation that may occur for very small amount of gluten and also if serology is negative.
The only measure of persistent villous atrophy and/or inflammation is the small intestinal biopsy. Earlier research suggests mucosal healing is seen in 8–96% of patients at follow-up biopsy (with most studies reporting a healing at follow-up in 57–76%). 5 While mucosal healing does not seem to influence mortality in CD, 99 it does seem to influence the risk of future lymphoproliferative malignancy 72 and osteoporosis. 71 Meanwhile there is no consensus on the role of follow-up biopsies, especially in asymptomatic patients in whom clinical improvement is seen. Many physicians therefore rely on serology at follow-up. Unfortunately, data clearly shows that serology at follow-up has a poor correlation with mucosal healing,155 and reliance on serology may therefore underestimate the activity of CD.
Most coeliac patients respond to a GFD. Dietary consultation with a dietitian when available or a trained physician is vital to ensure that the patient’s diet meets recommended nutrient intakes and individual requirements. Children require specific monitoring of growth and development and nutritional requirements, and ideally, the involvement of a paediatric gastroenterologist and a paediatric dietitian.
Long-term adherence to GFD without assessment may lead to nutrient deficiencies, with a negative impact on health outcome in the coeliac patient, 101 such mineral and vitamin deficiencies, 79 notably folate deficiency. 102 However, starting a GFD can be considered an opportunity to make better food choices. A recent study from Finland showed that on a GFD, 69% of underweight CD patients gained and 18% of overweight and 42% of obese patients lost weight; in the rest, body mass index remained stable. The favourable weight change, however, was associated with subjects’ self-rated expertise on GFD and young age at diagnosis, rather than dietary counselling received. 103
Some studies have shown that the average fibre consumption among patients with CD is generally lower than recommended.90,104 Patients may need advice about alternative sources of dietary fibre or the addition of proprietary fibre supplements. The introduction of GF oat products may be helpful for some. It is equally important to emphasize the nutritional quality of a GFD. 105
Patient surveys show that their preferred follow-up is an appointment with a dietitian in a dedicated clinic, but with specialist medical expertise available (concurrently). Dietitian-led or specialist-nurse-led coeliac clinics are being established to manage patients with CD.17,106 Information on the GFD may be obtained from various sources, not just dietitians or other healthcare professionals. Other surveys have found that while many patients are referred to and advised by a dietitian, the most useful information that they receive is provided by coeliac support groups, 107 and patients should be encouraged to join these organizations. However, adhering to a GFD is difficult for many people. 108 Once diagnosed, coeliac patients should be followed-up to reinforce dietary adherence, so that nutritional needs are met and complications avoided.
Persistence of symptoms despite a gluten-free diet
If symptoms persist after 6–12 months (depending on severity) or recur after a period of recovery, patients should be reviewed. The diagnosis should be confirmed, as some cases are due to incorrect diagnosis. 109 The original biopsies and serology should be reviewed. If not already checked, HLA genotype may be helpful as patients negative for both HLA DQ2 and DQ8 are very unlikely to have CD.
A detailed dietetic review is necessary as the majority of cases are due to ingestion of gluten. In the absence of obvious sources, oats should be excluded as a small percentage of patients may be oat sensitive. 110 Other common sources of gluten include communion wafers and malted drinks. A recent review has also raised the possibility of harm from maize prolamins in a subgroup of coeliac patients 111 and that they may benefit from a GF maize-free diet.
Recently two studies have been published that might have a great impact in managing symptomatic coeliac patients who, despite good dietary adherence, remain symptomatic and still have small intestinal inflammation. The first study showed that ALV003, a mix of two recombinant gluten-specific proteases given per os, is able to prevent gluten-induced mucosal injury due to 2 g of gluten in a phase 2 trial. 112 The second study evaluated in a randomized, parallel, double-blind, placebo-controlled, multicentre trial the effect of larazotide acetate on gastrointestinal signs and symptoms in patients with CD on a GFD (not challenged with gluten). The trial demonstrated that there was a significant difference in the reduction in gastrointestinal symptoms between the larazotide acetate 0.5 mg group and the placebo group in the modified intention-to-treat analysis (p = .022) and the per protocol analysis (p = .005). 113
Patients may have secondary lactose intolerance due to villous atrophy and benefit from a low lactose diet particularly if diarrhoea or bloating persist. In some patients, symptoms may continue if they have primary lactose intolerance. Other co-existing conditions such as microscopic colitis, pancreatic insufficiency, inflammatory bowel disease, bacterial overgrowth and thyroid dysfunction should be excluded.
If symptoms continue up to several months (after diagnosis) despite the above measures there is a general consensus in repeating duodenal biopsies to reconfirm the diagnosis, look for improvement or confirm persistent mucosal abnormality. Biopsies in selected cases should be examined for T-cell receptor monoclonality or evidence of enteropathy-associated small bowel lymphoma (EATL). Patients with persistent symptoms and significant histological abnormalities (villous atrophy with crypt hyperplasia; not inflammation only), despite a strict GFD, after 2 years should be considered to have refractory CD (RCD). 114 The presence in intestinal mucosa of T-cell receptor monoclonality will allow the diagnosis of RCD 2 and immunosuppressant medication or other chemotherapy should be started. Assessment of anti-transglutaminase antibodies during diet follow-up has limitations,115,116 but if serology is positive and the patient has been on a long-term GFD, that would suggest that the patient is consuming gluten (intentionally or inadvertently).100,117,118
Gluten-free diet in dermatitis herpetiformis
Evidence for the efficacy of a GFD in the management of both the gastrointestinal and cutaneous manifestations of DH has come from many sources. 119 The gut improves in a matter of weeks but the skin lesions may take months or years to clear. Because the rash is so itchy the patient is initially treated with dapsone, which has been established as effective therapy for over 70 years. The rash usually clears within 48 hours of starting the drug, but dapsone has no effect on the gastrointestinal changes. The use of dapsone is limited by its side effects, particularly haemolysis, and occasionally has to be substituted with an alternative sulphonamide. The minimal drug requirement to control the rash should be established before starting a GFD. This should be reviewed every 2–3 months as it will fall as the GFD starts to control the rash and the drug is better absorbed as the enteropathy improves.
In the original study by Fry et al. 120 the mean time taken to reduce the drug requirement was 8 months (4–30) and for stopping the drug 29 months (6–108). These authors emphasized the importance of strictness of the diet: 96% of the patients in whom the diet was shown to be strict were able to stop taking drugs altogether. Other studies support these data.121–123 Control of the rash with a GFD is sustained in the long term.124,125 Both the skin and the gut relapse on reintroduction of gluten into the diet.126,127
Many patients with DH have few gastrointestinal symptoms and their rash is well controlled with dapsone. It can be difficult to persuade them to adhere to a strict GFD with its complexity and social limitations. Because of this some patients opt for a normal diet, but even a low-gluten diet will allow some reduction in dapsone dosage. Some authors recommend the avoidance of oats, but provided these are pure with no contamination from gluten-containing cereals they are safe to eat. 128
The advantages of a strict GFD in the management of DH can be summarized as in Bolotin and Petronic-Rosic; 119 (i) a significant reduction or withdrawal of drug therapy; (ii) resolution of the gastrointestinal involvement; and (iii) an early and improved sense of wellbeing. 117 There is also evidence that a GFD has a protective effect against lymphoma in patients with significant CD.129,130
The gluten-free diet in other diseases
A considerable amount of data are consistent with the concept that a strict GFD is necessary for CD and DH due to the evidence of improved health of CD and DH patients on GFD. 5 In recent years, however, a GFD has been proposed also for other diseases. For completeness of the present review, although it is focused on CD and DH, we summarize here the existing data on gluten neuropathy and on non-coeliac gluten/wheat sensitivity.
Gluten-free diet in neurological manifestations
Neurological manifestations due to sensitivity to gluten have been increasingly recognized during the last 20 years. By far the most common manifestations include ataxia (gluten ataxia), neuropathy (gluten neuropathy) and headache with white matter abnormalities on magnetic resonance imaging (MRI) of the brain. 131 There is also a strong association with epilepsy with occipital calcifications and CD. 132
Patients presenting with neurological manifestations often have little in the way of gastrointestinal symptoms (a similar observation to that seen in DH) and diagnosis at a later age (61 vs. 47) by comparison with those who present with gastrointestinal symptoms. 133
Not all patients have enteropathy (only 40% of patients with gluten ataxia have enteropathy), but by definition these patients have serological markers suggestive of sensitivity to gluten (anti-gliadin IgG or IgA antibodies, low level of TG2 antibodies and more recently anti-TG6 antibodies). 134
The effect of a GFD on the neurological manifestations has been the source of a number of single and multiple case reports. Response to a GFD depends on the duration of the ataxia prior to the diagnosis. Loss of Purkinje cells in the cerebellum, the end result of prolonged gluten exposure in patients with gluten ataxia, is irreversible and early diagnosis and treatment is more likely to result in improvement or stabilization of the ataxia. Most case reports primarily report patients with established CD who then develop neurological symptoms. Such studies suggest variable but overall favourable responsiveness to a GFD. Only one systematic study of the effect of a GFD on a cohort of patients presenting with ataxia, with or without an enteropathy, has been published. 135 This study also reported serological evidence of elimination of the AGA as a confirmation of strict adherence to the diet. Some 43 patients with gluten ataxia were enrolled; 26 adhered strictly to the GFD, had serological evidence of elimination of antibodies and comprised the treatment group. Fourteen patients refused the diet and comprised the control group. There was no significant difference in the baseline performance for each ataxia test between the two groups. There was significant improvement in performance in ataxia scores and in the subjective global clinical impression scale in the treatment group when compared with the control group. The improvement was apparent even after excluding patients with enteropathy. Similar observations have been reported in patients with gluten neuropathy where there was evidence of improvement on repeat neurophysiological assessment after 1 year of strict GFD 136 and in patients with headache and white matter abnormalities on MRI where the headaches improve and the white matter changes stabilize. 137 Finally, patients with epilepsy and occipital calcifications often demonstrate improvement in their seizure control after the introduction of a GFD. 132
Gluten-free diet in non-coeliac wheat or gluten sensitivity
It has long been known that a sizeable number of patients with functional gastrointestinal symptoms respond to wheat exclusion from the diet but prove not to have CD on formal testing.138–140 In some cases the underlying cause is an IgE-mediated type I hypersensitivity reaction, 141 which may be discernible as a result of rapid onset of symptoms after gluten ingestion.142,143 or by an association with exercise-induced anaphylaxis. 144 However, the increasing availability of GF food as treatment for CD has led many patients with gastrointestinal symptoms to follow gluten rather than wheat exclusion, and this has led to considerable confusion and controversy over whether gluten or another wheat component is responsible for the symptoms. In addition to gluten, wheat contains poorly digested fermentable carbohydrate sources – such as fibre and fructans (‘FODMAPS’ – fermentable oligodisaccharides, monosaccharides and polyphenols) – that could lead to functional symptoms.145,146 A recent study tested patients with self-reported gluten-sensitive symptoms in a placebo-controlled trial where the gluten was used without contaminating FODMAPs. 147 This demonstrated a significant effect of the gluten itself in mediating a variety of symptoms, including effects on fatigue and mood as well as the gastrointestinal tract. However, a follow-up study demonstrated no benefit of gluten restriction in patients who were already on a low FODMAP diet, suggesting that gluten itself is not the causative factor, 148 although it may still play a role combination with FODMAPs. A number of explanations could underlie these observations and require further clarification. In most studies to date, a proportion of the patients express HLA DQ2 and/or 8 in whom the possibility of CD may not have been exhaustively excluded.142,147–149 Therefore, symptomatic benefit in these patients may indicate an immune response akin to CD and might suggest that symptoms in CD may relate poorly to currently defined histological changes. Responses to gluten withdrawal in patients lacking the necessary HLA require alternative explanations that may not be specific to gluten itself but depend on other substrates such as FODMAPs. However, it is now clear that gluten has a number of effects on the intestinal epithelium that are unrelated to adaptive immune responses. These include a direct effect on enterocytes leading to interleukin-15 secretion and a ‘stress’ response,150,151 and upregulation of zonulin – an endogenous mediator of tight junction permeability – by a mechanism that involves recognition of a gliadin peptide fragment by enterocyte surface chemokine receptors. 152 Intestinal permeability has indeed been found to be altered by gluten in patients reporting gluten sensitivity without HLA DQ 2 or 8, and may result in an increase in IgG AGA.143,149 Finally, the physico-chemical properties of gluten may be relevant (this is the feature that results in improved baking properties), as it may conceivably affect particle size and digestibility of other dietary components and could explain the interaction of gluten with other fermentable substrates leading to symptoms. 153 While there is much yet to understand about the nature of non-coeliac gluten sensitivity, it is important for patients to undergo thorough testing to exclude CD, as the implications of correct diagnosis include the necessary rigour of gluten exclusion needed, whether gluten or wheat exclusion is required for symptom relief, and the risk of long-term complications with CD that are not recognized with non-coeliac gluten or wheat sensitivity. A recent survey showed that in 62% of 146 so-called ‘non-celiac gluten-sensitive’ patients, CD was not adequately excluded prior to GFD. 154
Useful hints and tips for patient management
IMPORTANT: GFD should not be started before testing for CD. In fact, CD can be appropriately diagnosed only when the biopsy and the presence in blood of specific antibodies (anti-transglutaminase IgA, anti-endomisium IgA, anti-deamidated gliadin IgA and IgG) and of the total amount of Immunoglobulin IgA are assessed
While on a GFD in presence of: persistent gastrointestinal symptoms review biopsies and check initial diagnosis was correct, check for GFD adherence, inadvertent gluten intake, irritable bowel syndrome, lactose intolerance, microscopic colitis, pancreatic insufficiency, RCD, lymphoma, colonic cancer, other malignancies. persistent positive serology dietetic review/ food diary to check for GFD adherence, inadvertent gluten intake, repeat lab test after strict GFD. persistent villous atrophy check for GFD adherence, inadvertent gluten intake, RCD, lymphoma, exclude other causes of villous atrophy not related to CD, consider revision of histology (for example: lack of orientation of mucosa fragments, one single biopsy). presence of alarm signs and symptoms (anaemia, increased ESR and CRP, fever, weight loss, persistent diarrhoea, hypoalbuminaemia) check for RCD, lymphoma, colonic cancer and other malignancies, infections. occasional inadvertent gluten intake reassurance; if necessary, symptomatic treatment for diarrhoea, etc. intentional, recurrent/continuous gluten intake discuss reasons with the patient, reinforce the need to follow GFD. Offer psychological support and further dietitian consultation to support the choice for affordable and easy-to-find palatable alternatives to gluten-containing food. Advise the patient to join patients’ advocacy groups for self-support. Follow-up biopsy in symptomatic patients Symptomatic patients should undergo follow-up biopsy to rule out persistent villous atrophy, refractory CD, and malignancy. Follow-up biopsy in asymptomatic patients While the mucosal appearance at follow-up biopsy has been linked to the future risk of lymphoproliferative malignancy and osteoporosis, there is currently no evidence to suggest that all asymptomatic patients should undergo follow-up biopsy.
Key points regarding a gluten-free diet
CD requires a lifelong GFD that generally improves most symptoms and ensures some protection from complications Dietary treatment includes elimination of gluten-based staples/foods, replacement with GF substitutes and also using naturally GF foods The International Codex standard for food labelled as GF has been set at ≤ 20 parts per million (ppm) The GFD should contain appropriate amount of fibre, vitamin and nutrients The GFD should be assessed after some time from diagnosis and may require supplementation We recommend medical and dietetic follow-up Dietary education should include dietetic consultation and be reinforced with additional information by printed and electronic resources; knowledge update and ongoing support are important to aid dietary compliance A GFD may limit a patient’s social life and have a negative impact on quality of life Referring patients to national support organizations (Coeliac UK for UK, or other coeliac societies globally) at diagnosis provides a safety net for individuals at a vulnerable time There is some evidence of beneficial effect of GFD in neurological diseases in which there is the presence of specific gluten-related antibodies Some non-CD people improve their symptoms with the exclusion of gluten from their diet; there is much yet to understand about the nature of non-coeliac gluten or wheat sensitivity. It is important for patients to undergo testing to exclude CD as the implications of correct diagnosis influence the necessary rigour of gluten exclusion
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
DSS has received an educational grant from Dr Schär (a gluten-free food manufacturer) to undertake an investigator-led research study on gluten sensitivity. The other authors disclose no conflict of interest.