
Abstract
Background
Although diverticular disease is a common condition, its effective treatment is challenging in clinical practice.
Objective
The objective of this article is to assess pharmacological management in different clinical settings of diverticular disease and factors associated with treatment using the Italian registry Registro Malattia Diverticolare (REMAD).
Methods
At study enrolment, patients were categorised into subgroups: diverticulosis, symptomatic uncomplicated diverticular disease and previous diverticulitis. We registered demographic, clinical and lifestyle factors, quality of life and the use of treatments for diverticular disease in the last year. Logistic regression analysis assessed the association between clinical factors and treatment consumption.
Results
A total of 500 of the 1206 individuals included had had at least one treatment for diverticular disease in the last year: 23.6% (166/702) of patients with diverticulosis, 55.9% (165/295) of patients with symptomatic diverticular disease, and 80.9% (169/209) of patients with previous diverticulitis (p < 0.001). In multivariate analysis, the following factors were significantly associated with treatment use: female gender, family history of colonic diverticula, organic digestive comorbidity and impaired physical quality of life components.
Conclusion
Individuals with diverticular disease take medications based on the different clinical settings of disease. We identified different features associated with treatment use in the distinct clinical entities of diverticular disease.
Keywords
Key summary
Current knowledge:
Although diverticular disease is a very common condition, its natural history is poorly known and most of our knowledge is anchored to old and methodologically flawed data. The treatment of diverticular disease in its different clinical scenarios is still challenging.
Key findings of this study:
This study demonstrated that patients with diverticular disease take medications based on different clinical settings of the disease. Different factors are associated with the use of therapy, particularly the impairment of quality of life in patients with symptomatic diverticular disease.
Introduction
Colonic diverticulosis is the most frequent non-neoplastic outcome at routine colonoscopy, 1 and its prevalence increases with age. 2 The spectrum of diverticular disease covers different clinical settings with protean symptoms, severity and outcomes. 3 Colonic diverticular disease may be classified as follows: 1) asymptomatic diverticulosis; 2) symptomatic uncomplicated diverticular disease (SUDD), with abdominal symptoms without overt inflammation; and 3) acute diverticulitis, with or without complicated disease or recurrence, characterised by macroscopic inflammation.3–5 In the United States, the annual cost of diverticular disease ranges between 2.2 billion and 2.6 billion dollars, making this condition the fifth most costly gastrointestinal disorder considering direct and indirect costs. 6 The natural history of diverticulosis and diverticular disease is poorly known and most of our knowledge on its epidemiology, pathophysiology, prevention and management is anchored to old and methodologically flawed data.
The Italian Study Group on Diverticular Disease (Gruppo Italiano Malattia Diverticolare or GrIMAD), a scientific association with the aim to implement knowledge on diverticular disease, created in May 2015 an ongoing registry of patients with a diagnosis of diverticular disease, the Registro Malattia Diverticolare (REMAD). Currently, the registry is running a five-year, multicentre, prospective, observational, cohort study which involves 1217 consecutive patients with the purpose of comparing clinical features and lifestyle factors associated with diverticular disease and its different clinical scenarios, and to obtain insights into the natural history of diverticular disease. 7
Although the diagnosis of diverticular disease may be easy, 1 its management is cumbersome since randomised controlled trials (RCTs) on treatments for the different clinical entities are scarce, often dated, and low in quality or negative. 8 The management of these patients often follows tradition or expert opinion rather than evidence-based medicine. Similarly, the existing practice guidelines are mainly based on expert opinion.8,9 The goal of treatment in diverticular disease remains symptom relief and prevention of diverticulitis and its recurrence. The actual strategies, although often lacking a robust mechanistic basis, comprise modulation of gut microbiota or dysbiosis with poorly absorbable antibiotics such as rifaximin or probiotics, and low-grade inflammation with anti-inflammatory compounds such as mesalazine or probiotics. Unfortunately, recent large high-quality trials assessing the role of mesalamine in the prevention of recurrent diverticulitis were negative10,11 or showed only a trend in reducing symptoms after diverticulitis. 12 For all the above reasons, the treatment of diverticular disease is still challenging.8,9
Thus, the aims of the present study were to assess what pharmacological management was performed in real-life Italian patients with different clinical entities of diverticular disease and whether the choice to undertake a treatment was related to demographic, clinical, lifestyle and health-related quality of life (HRQOL) factors of these patients.
Patients and methods
Study design
For the purpose of this study, we utilised the REMAD registry that follows prospectively a large cohort of patients with diverticular disease in Italy. Briefly, as previously described, 7 1217 patients enrolled consecutively during a two-month recruitment period from 47 Italian centres have been classified and phenotyped. In particular, demographic, clinical and pharmacological assessments have been performed using a set of validated questionnaires. 7 Demographic and clinical features of enrolled individuals have been previously described. 7 Inclusion and exclusion criteria as well as study methodology are discussed in detail in a previous paper. 7 In all participating centres, the mean rate of individuals who declined to take part in the registry was 24.0% ± 8.3%. 7
The protocol was approved by the coordinating centre University Federico II, Naples, on 24 September 2014 (approval identification no: 161/14) and by independent ethics committees at each centre. The study was carried out according to the Declaration of Helsinki and the principles of good clinical practice. Written informed consent was provided by all patients. All authors reviewed and approved the final version of the manuscript and had full access to the study data. The study was registered on a public registry (ClinicalTrial.gov no: NCT03325829).
Data collection
At entry in our database, all patients were categorised into three subgroups 7 : diverticulosis, SUDD, and previous diverticulitis (PD). Demographic and clinical features, lifestyle factors and HRQOL were registered as previously detailed. 7 HRQOL was assessed with the Italian version of the Short-Form 12 (SF-12) Items Health Survey.13,14 This instrument was previously developed in the Italian general population and subsequently validated in individuals with chronic pancreatitis who reported chronic abdominal pain. 14 It includes 12 items that generate two summary scales exploring physical (Physical Component Summary or PCS-12) and mental (Mental Component Summary or MCS-12) HRQOL components. PCS-12 and MCS-12 range from 0 to 100 and higher scores indicate better HRQOL. The two scores are based on the score of eight subscales, four for each HRQOL component: physical functioning, role-physical, bodily pain and general health for PCS-12; vitality, social functioning, role-emotional and mental health for MCS-12. In addition, PCS and MCS scores were both dichotomised based on a score of 50 that represents the mean value of the Italian general population. 15 A score lower than 50 is representative of patients with impaired HRQOL.
The following clinical features were evaluated as dichotomous data: female gender, age ≥60 years, body mass index (BMI) ≥30 kg/m2, family history of colonic diverticula or cancer, presence of organic digestive comorbidity (including at least one of the following well-documented organic digestive diseases as diagnosed by history-taking: gastroesophageal reflux disease, Helicobacter pylori-positive or -negative gastritis, peptic ulcer disease, coeliac disease, inflammatory bowel disease, previous acute appendicitis, cholelithiasis, acute or chronic hepatitis, cirrhosis, acute or chronic pancreatitis, other diseases), Charlson index score ≥3, active smoking, alcohol or coffee drinking, physical activity, MCS-12 <50, and PCS-12 <50. In addition, age, BMI, MCS-12 and PCS-12 were also assessed as continuous data.
Pharmacological assessment was performed evaluating therapies that patients were taking or had taken in the last year for diverticular disease or diverticulosis. The following treatments were evaluated: poorly absorbable antibiotics (rifaximin, paromomycin, neomycin), mesalazine, probiotics, prebiotics/fibres and antispasmodics. The rate of assumption was categorised as follows: occasional (≤3 per year for poorly absorbable antibiotics or ≤2 per year for the other treatments), frequent (>3 per year for poorly absorbable antibiotics or >2 per year for the other treatments), monthly or continuous. The different cut point reflects the different mechanism of action and way of use between poorly absorbable antibiotics such as rifaximin (a short-term cyclic treatment) and the other treatments (long-term treatments, generally).
Statistical analysis
Continuous data were described as mean and SD, and categorical data as frequencies. The following analyses were applied: one-way analysis of variance, the Fisher exact test and the chi-squared test. Where appropriate, the three subgroups of participants were compared by using the chi-squared test for trend. Univariate analysis was performed using chi-squared test or independent t-test as appropriated, while multivariate logistic regression, including as covariates all the considered variables, identified independent factors associated with treatment for diverticular disease. In particular, for the latter, the enter method was used and all variables, significant or insignificant, were included in the analysis. We also computed odds ratios (ORs) and 95% confidence intervals (CIs). All statistical analyses were performed using a dedicated software package (MedCalc Software, Mariakerke, Belgium, version 12.2). P values less than 0.05 (two tailed) were considered significant.
Results
Therapies in different clinical settings of diverticular disease
Individuals taking therapies for diverticular disease according to subgroups based on diverticular disease status.
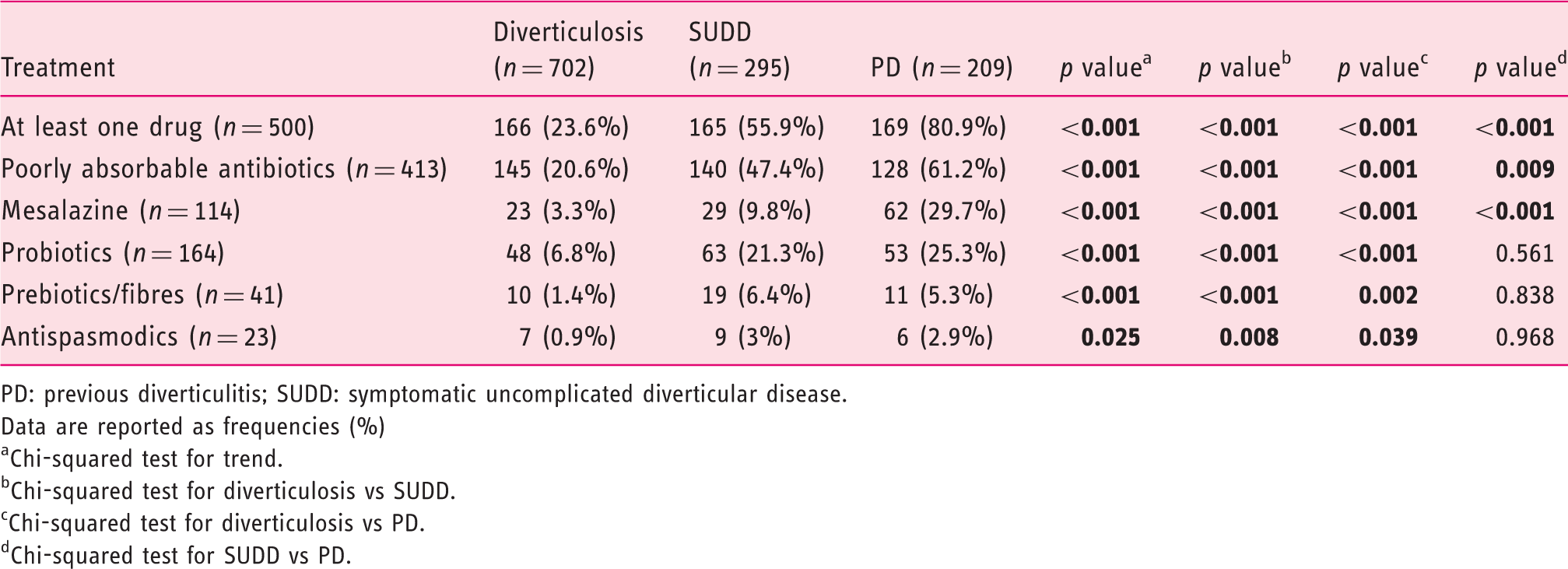
PD: previous diverticulitis; SUDD: symptomatic uncomplicated diverticular disease.
Data are reported as frequencies (%)
Chi-squared test for trend.
Chi-squared test for diverticulosis vs SUDD.
Chi-squared test for diverticulosis vs PD.
Chi-squared test for SUDD vs PD.
Frequency of drug intake according to diverticular disease status.
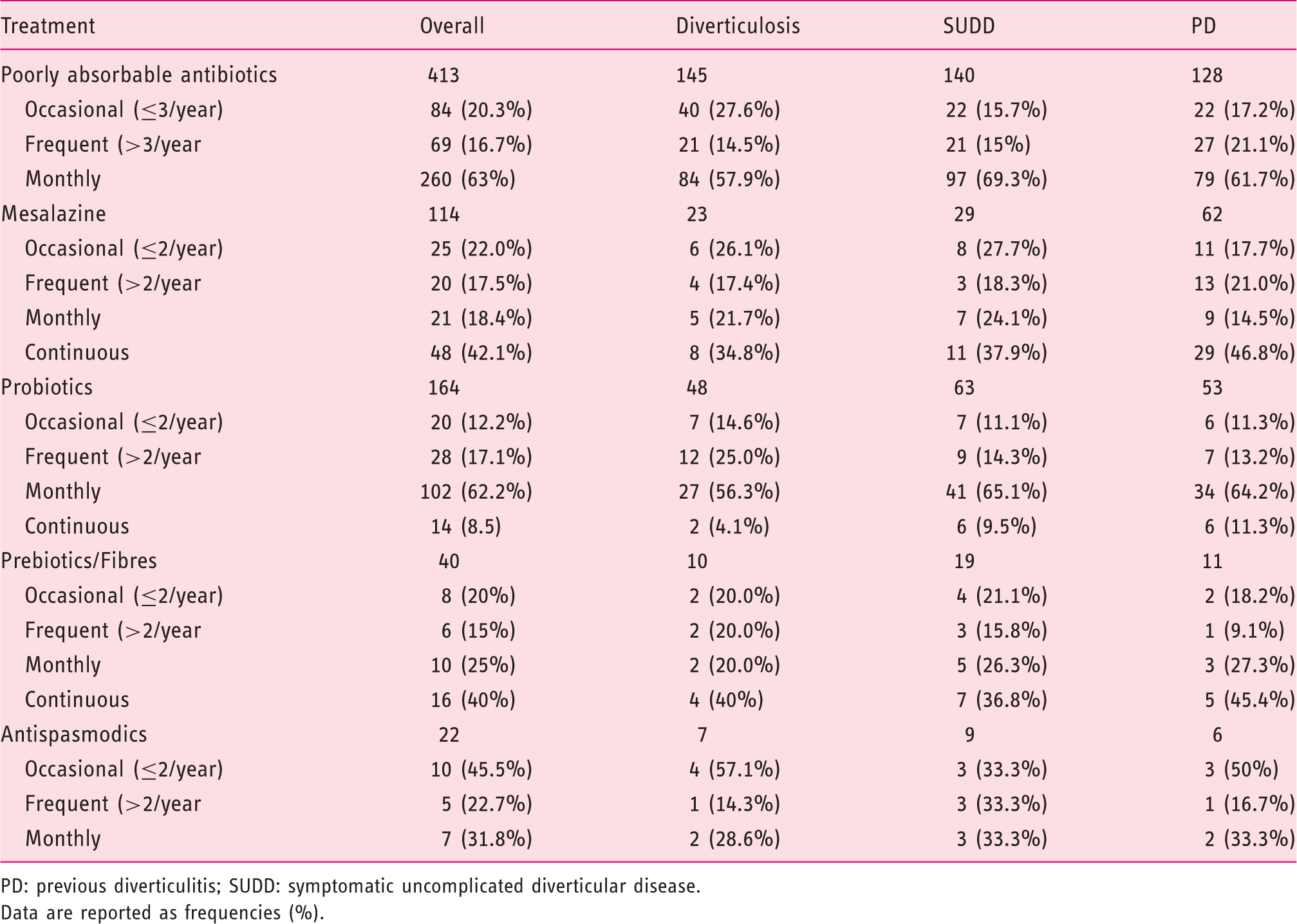
PD: previous diverticulitis; SUDD: symptomatic uncomplicated diverticular disease.
Data are reported as frequencies (%).
Factors associated with treatment for diverticular disease
Factors associated with treatment use in all participants with diverticular disease.
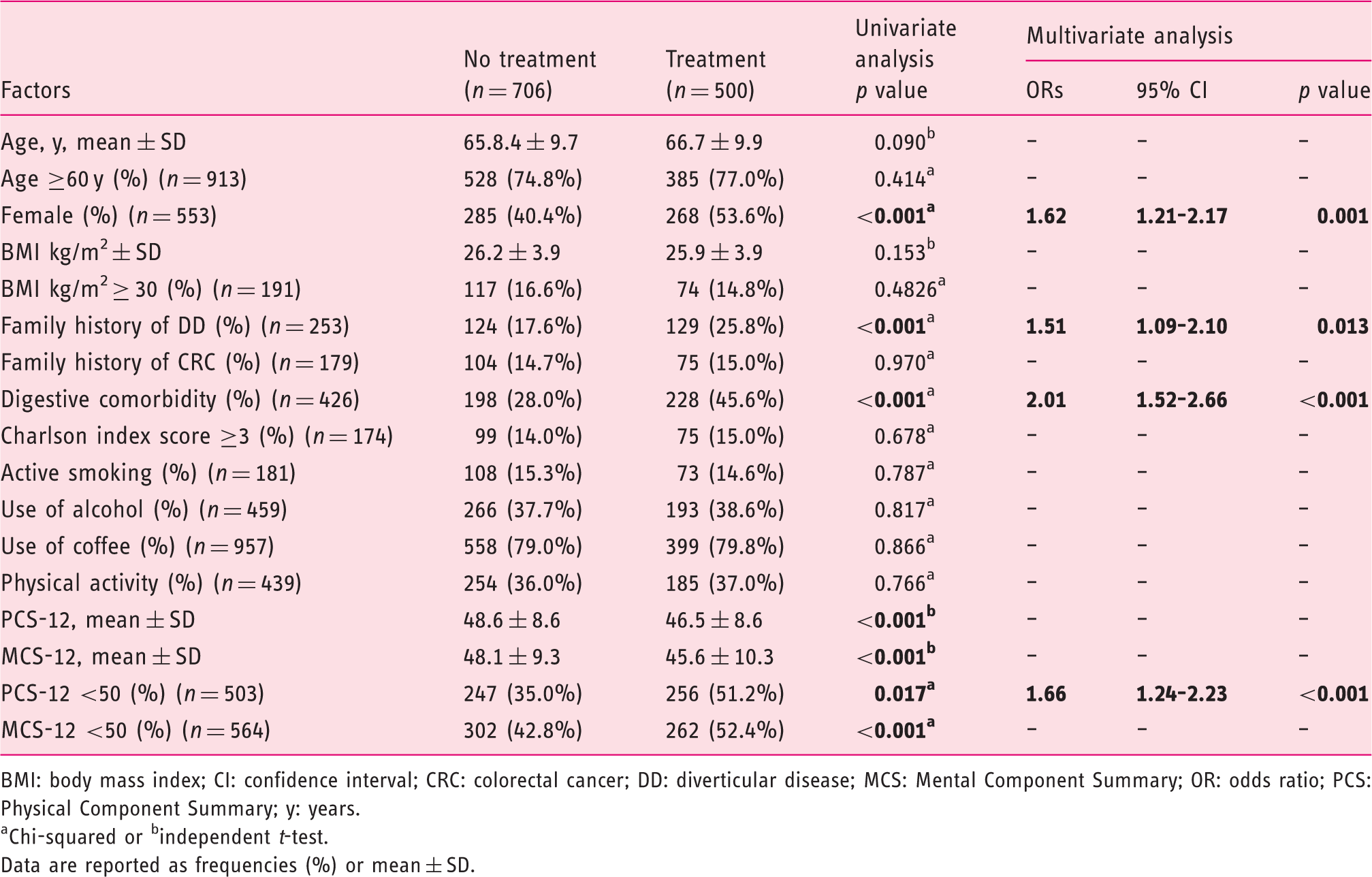
BMI: body mass index; CI: confidence interval; CRC: colorectal cancer; DD: diverticular disease; MCS: Mental Component Summary; OR: odds ratio; PCS: Physical Component Summary; y: years.
Chi-squared or bindependent t-test.
Data are reported as frequencies (%) or mean ± SD.
Factors associated with treatment use in participants with diverticulosis.
BMI: body mass index; CI: confidence interval; CRC: colorectal cancer; DD: diverticular disease; MCS: Mental Component Summary; OR: odds ratio; PCS: Physical Component Summary; y: years.
Chi-squared or bindependent t-test.
Data are reported as frequencies (%) or mean ± SD.
Factors associated with treatment use in participants with SUDD.
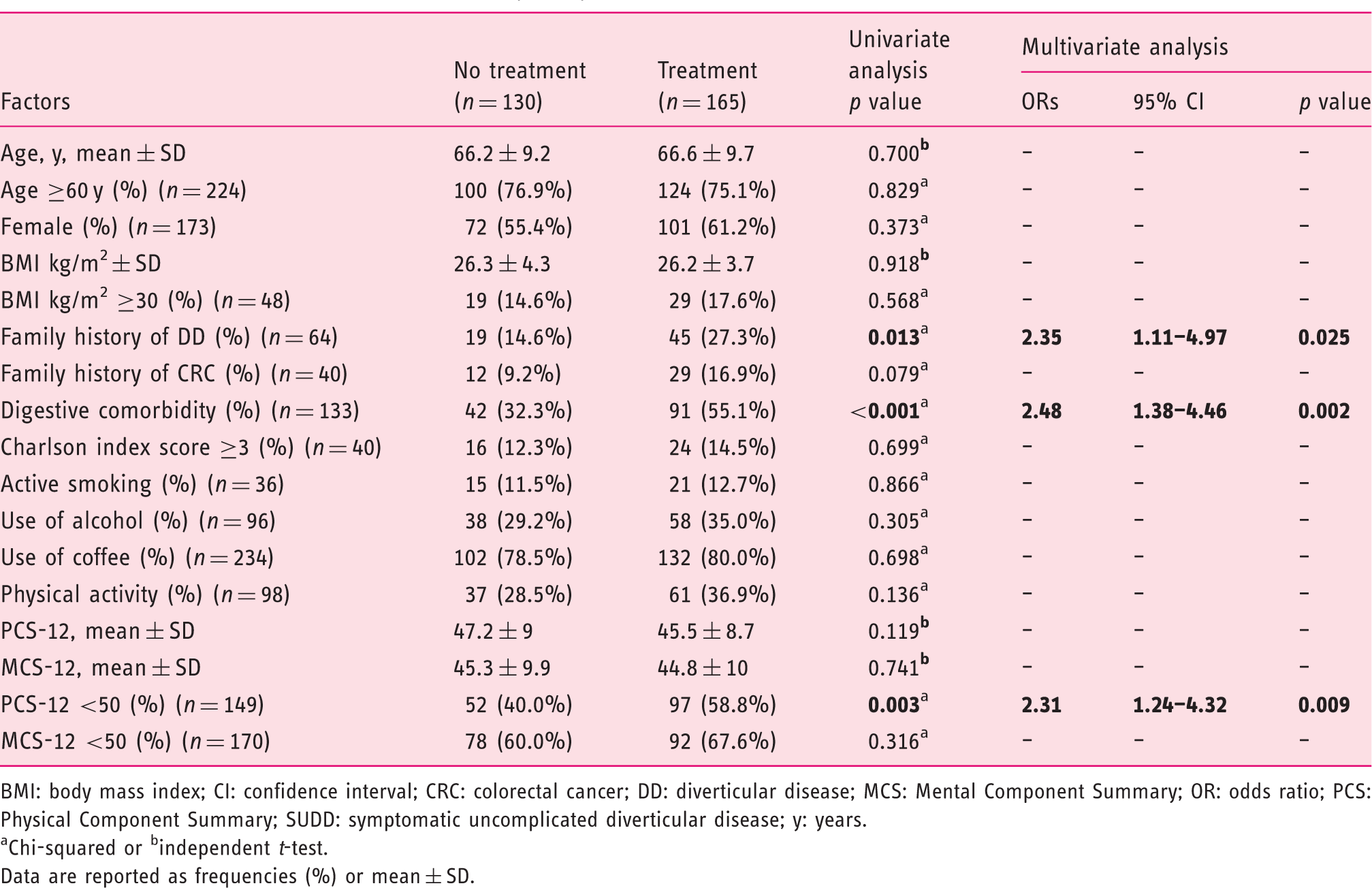
BMI: body mass index; CI: confidence interval; CRC: colorectal cancer; DD: diverticular disease; MCS: Mental Component Summary; OR: odds ratio; PCS: Physical Component Summary; SUDD: symptomatic uncomplicated diverticular disease; y: years.
Chi-squared or bindependent t-test.
Data are reported as frequencies (%) or mean ± SD.
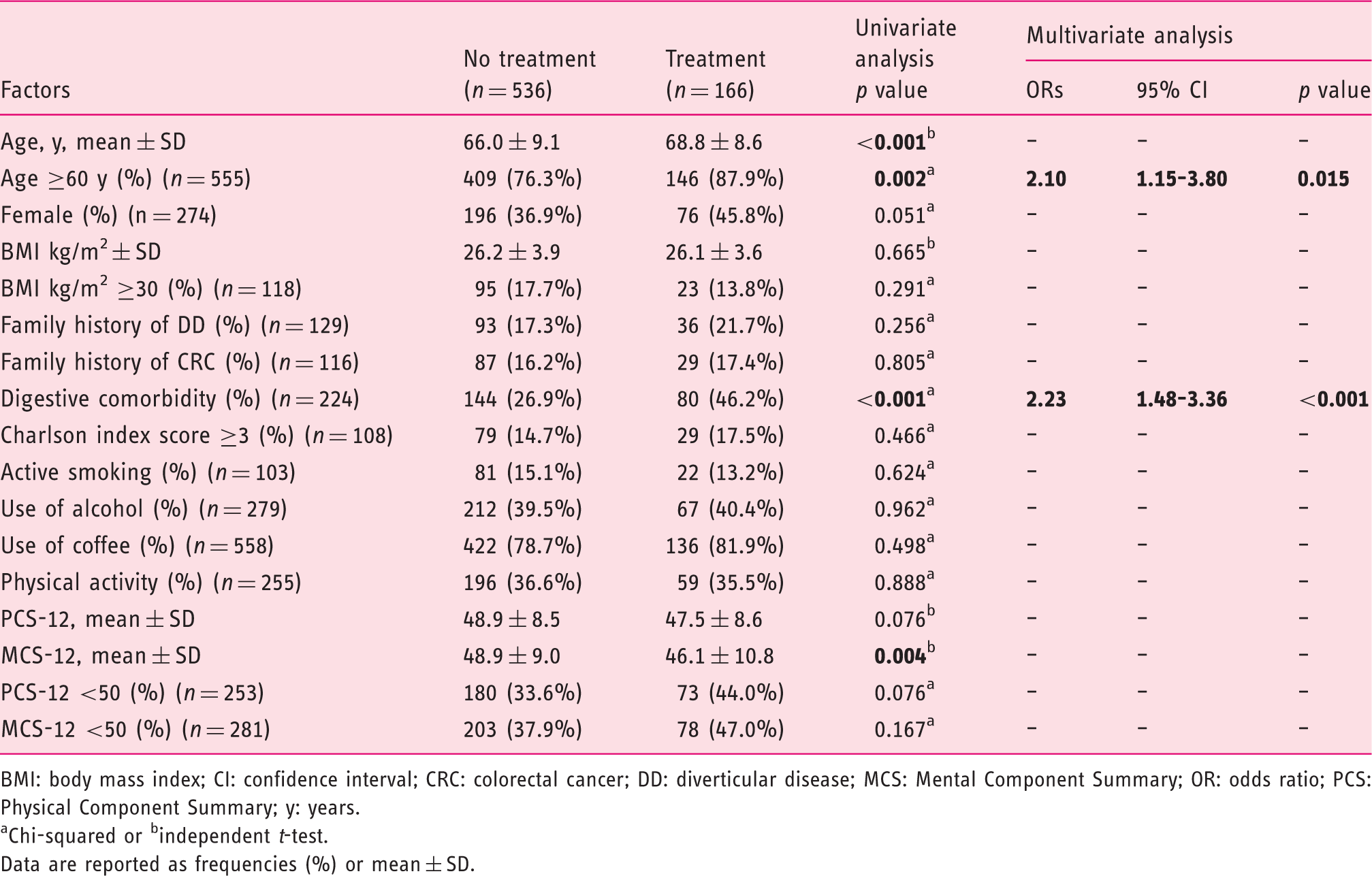
Factors associated with treatment use in participants with PD.
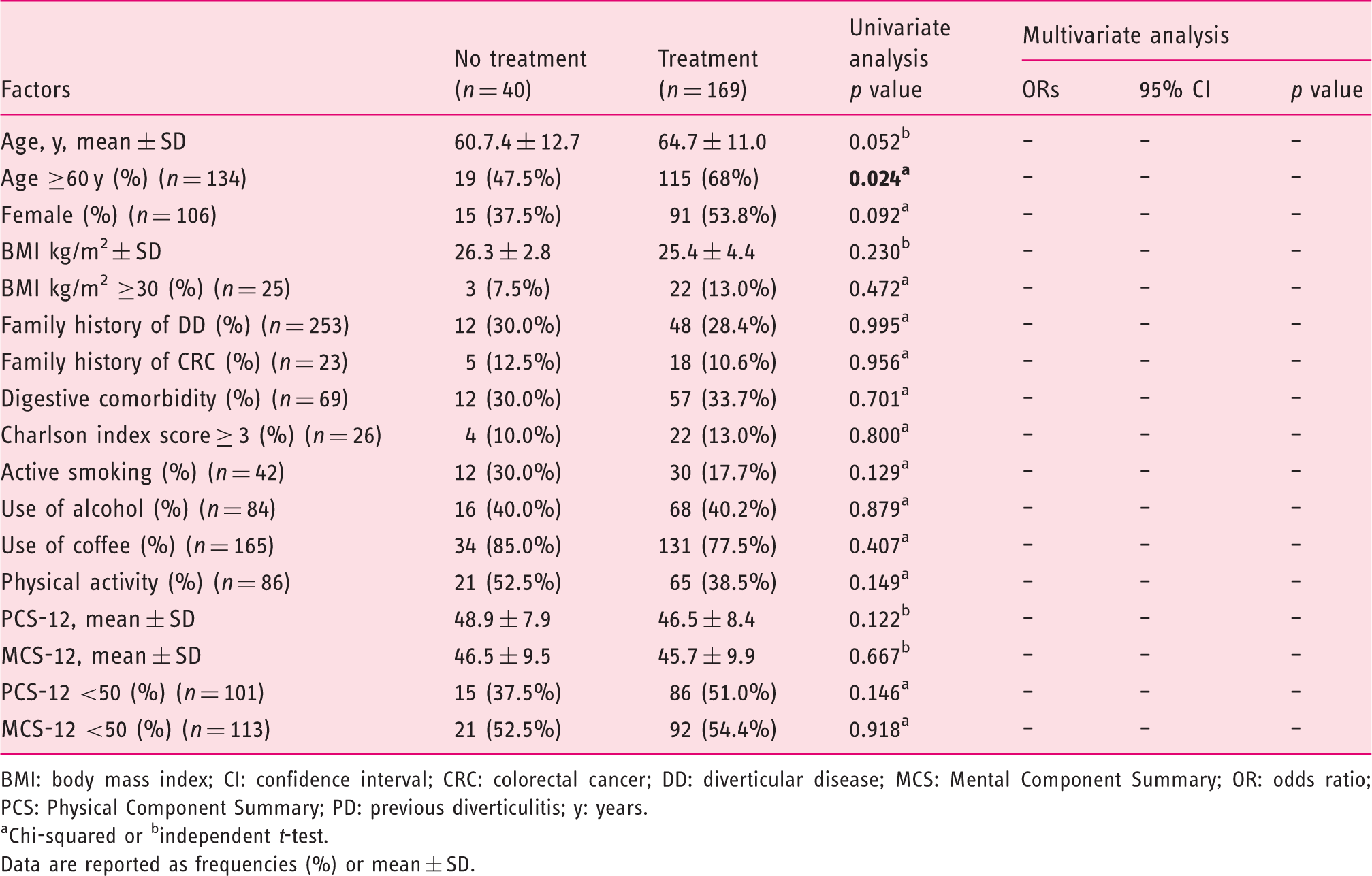
BMI: body mass index; CI: confidence interval; CRC: colorectal cancer; DD: diverticular disease; MCS: Mental Component Summary; OR: odds ratio; PCS: Physical Component Summary; PD: previous diverticulitis; y: years.
Chi-squared or bindependent t-test.
Data are reported as frequencies (%) or mean ± SD.
Discussion
We report the results of the REMAD registry assessing the pharmacological management of patients with different clinical settings of diverticular disease. We showed that 23.6% of patients with asymptomatic diverticulosis, 55.9% of patients with SUDD, and 80.9% of patients with PD were taking or had taken at least one medication in the last year for their clinical condition. The therapeutic armamentarium relies on the poorly absorbable antibiotic rifaximin in the vast majority of cases, but also on mesalazine and probiotics, alone or in different combinations. In all cases, the use of therapies was independently associated with female sex, family history of colonic diverticula, organic digestive comorbidity and impaired physical components of HRQOL, although different factors were implicated in diverticulosis and SUDD. All together our data confirm that the management of diverticular disease remains one of the main challenges in gastrointestinal clinical practice. 8
About one-fourth of our participants with asymptomatic diverticulosis were taking at least one drug. This is in contrast to the results of the Italian Consensus Conference for Colonic Diverticulosis and Diverticular Disease, indicating that there is no rationale for drug treatment of asymptomatic diverticulosis. 3 This approach is probably based on the dogma that diverticulosis is a condition at risk for acute diverticulitis or diverticular bleeding.16,17 Previous studies indicated that, among individuals with diverticulosis, 15%–25% of them will develop acute diverticulitis during their lifetime. 16 In contrast, a recent retrospective study showed that only 4.3% of patients with diverticulosis at baseline develop acute diverticulitis during long-term follow-up. 5 However, the design of this study is suboptimal because of its retrospective nature, and probably for this reason is not able to contradict the common idea that diverticulosis is a condition at high risk of progression. 17 The results of the REMAD registry are expected to definitely clarify whether diverticulosis is a condition at high or low risk for developing diverticulitis or diverticular bleeding. In addition, the high consumption of rifaximin for asymptomatic disease is of concern because of the risks of spreading resistance throughout the population. In the United States, the widespread use of this treatment for irritable bowel syndrome and hepatic encephalopathy has coincided with a marked rise of rifaximin resistance in Clostridium difficile from 8% to 35%, 18 and the resistance can be transferred to staphylococci, potentially making rifampin treatment for foreign-body infection ineffective. 19
More than one-half of our patients with SUDD take medications for this condition. The approaches generally proposed in clinical practices include a high-fibre diet, the use of anti-spasmodics, mesalazine, cyclic poorly absorbable antibiotics such as rifaximin, prebiotics and probiotics.8,9,20 The rationale for the use of anti-inflammatory therapies or approaches targeting enteric bacteria is based on pathophysiological studies showing low-grade inflammation,21,22 and on the hypothesis that bacterial overgrowth in the diverticulum is the initiator of events evolving into symptom generation, inflammation and complications. 23 We have recently shown the presence of dysbiosis involving pro-inflammatory and pathogenetic bacteria in patients with SUDD. The following low-grade inflammation, characterised particularly by macrophages, could contribute to the development of symptoms. 23 A meta-analysis of four randomised studies involving 1660 patients with SUDD showed that rifaximin plus fibre supplementation improves symptoms and prevents complications at one year. 24 However, the methodological quality of these studies was poor, since three of these were open and the only high-quality study took place more than 20 years ago. 25 Although almost all (with the exception of German 26 ) guidelines suggest cyclic rifaximin plus fibre supplementation should be recommended for symptom relief in patients with SUDD,3,27–29 more evidence should be provided to establish the best therapeutic dosage, the frequency of administration and its efficacy alone or in association with probiotics or other compounds. A meta-analysis of six randomised trials including 1021 patients with SUDD demonstrated mesalazine was more effective in symptom relief as compared with placebo, a high-fibre diet and rifaximin together. 30 Given the low quality of available studies, this evidence was considered enough to recommend this anti-inflammatory approach by the majority of international guidelines.3,27,28 The proof of efficacy of probiotics in SUDD is suboptimal since only two high-quality trials are available and, as suggested by a recent systematic review of 11 trials and a total of 764 patients, a meta-analysis cannot be undertaken.31,32
More than 80% of our patients with a previous episode of diverticulitis were taking at least one drug for their condition, the most common regimen of treatment being represented by rifaximin, mesalazine or probiotics, alone or in different combinations. However, mesalamine was not proven to prevent the recurrence of diverticulitis. 33 This aspect was recently addressed by two phase 3, multicentre RCTs, involving 590 and 592 patients (PREVENT 1 and 2, respectively) with at least one episode of acute diverticulitis during the previous 2 years. 10 In both studies, mesalamine was not better than placebo in the prevention of recurrence. 10 Similarly, although positive results have been reported in secondary prevention, the role of rifaximin in this clinical setting requires further investigation.19,25,33
In all the patients with diverticular disease, the use of pharmacological approaches was independently associated with female sex, family history of colonic diverticula, organic digestive comorbidity and impaired physical components of HRQOL. As expected, different factors were involved in diverticulosis and SUDD. In diverticulosis, pharmacological use was associated with older age and presence of organic digestive comorbidity, while SUDD was associated with family history of colonic diverticula, presence of gastrointestinal comorbidity and impaired physical components of HRQOL. This confirms that diverticulosis and SUDD are two distinct conditions with different outcomes3,7,20 and suggests that the presence of organic digestive comorbidity is a common factor involved in pharmacological use probably for the prevention of acute diverticulitis. This is in line with results of studies showing comorbidities are very frequent among patients with diverticulosis 34 and that factors associated with recurrent acute diverticulitis were patient age, female gender, smoking, obesity and, in particular, markedly increased comorbidity score. 35 In contrast, no factors were associated with PD, probably because the vast majority of these individuals take medications. In addition, a type 2 error cannot be excluded as the PD group, given the lower prevalence of this clinical setting, was likely underpowered to detect factors associated. In all the patients with diverticular disease, particularly in those with SUDD, there was an association between treatment use and impaired physical components of HRQOL. Several studies showed diverticular disease was associated with impairment of HRQOL.36,37 We have recently demonstrated that HRQOL is significantly higher in asymptomatic diverticulosis as compared with patients with SUDD or PD who reported similar HRQOL levels. 7 This suggests that patients with SUDD, because of their chronic abdominal symptoms, should be considered as having at least as severe a condition as patients with PD, justifying the broad pharmacological armamentarium used. In addition, our results suggest HRQOL is a major outcome measure also for patients with diverticular disease and one of the main factors involved in the use of therapeutic approaches. This is particularly true when we apply dichotomous scores using as cut-off the mean value of the Italian general population for distinguishing individuals with normal or impaired HRQOL, suggesting a deeper clinical relevance of dichotomous as compared with continuous variables for this outcome measure.
In conclusion, our study demonstrated that patients with diverticular disease take medications based on different clinical settings and that different factors are associated with the use of therapy, particularly the impairment of HRQOL in patients with SUDD. The results of our study reflect real-life Italian diverticular disease management. The great variety of treatments, single or in combination, doses and frequency of administration confirms that effective treatment of diverticular disease represents a difficult task in daily clinical practice.
Footnotes
Acknowledgements
This study was registered under ClinicalTrials.gov under identifier NCT03325829.
Declaration of conflicting interests
C.C. has received consultancy fees and/or speaker fees from Alfasigma/Alfa Wassermann, Almirall, Allergan, Valeas and Sofar. R.C. has served as a speaker and consultant for Alfasigma/Alfa Wassermann, Allergan, Malesci, Almirall, Fresystem, Shire, Sofar, Biocure, Co.GE.DI and Valeas, and has received research funding from Alfasigma/Alfa Wassermann, Fresystem, Sofar and CO.GE.DI. F.P. has served as a speaker for Allergan, Malesci, Menarini and Alfasigma/Alfa Wassermann. B.A. has served as a speaker and consultant for Alfasigma/Alfa Wassermann, Allergan and Malesci, and has received research funding from Alfasigma/Alfa Wassermann, Allergan and Biohit. G.B. has served as a speaker and consultant for Alfasigma/Alfa Wassermann, Allergan, CaDiGroup, Danone, Ironwood, Italchimici, Malesci, Menarini, Noos, Shire, Synergy, Sofar, Yakult and Zespri, and has received research funding from Alfasigma/Alfa Wassermann, Cadigroup, Falk Pharma, IMA, Italchimici, Lorenzatto, Parmalat Sofar, Yakult and Zespri. M.C., P.A. and M.R.B. have nothing to declare.
Ethics approval
The protocol for this study was approved by the coordinator centre University Federico II, Naples, on 24 September 2014 (approval identification no: 161/14) and by independent ethics committees at each centre. The study was carried out according to the Declaration of Helsinki and the principles of good clinical practice.
Funding
This work was supported by Alfasigma, Italy. The funding agency had no role in the study design, collection, analysis, data interpretation or writing of the report.
Informed consent
Written informed consent to participate in this study was provided by all patients.