
Abstract
Background and aims
Making an optimal and lasting submucosal cushion is critical for endoscopic submucosal dissection. The thermo-sensitive binary hydrogels system composed of poloxamer 407 and poloxamer 188 might be an excellent submucosal injection solution considering the unique feature that it remains liquid at room temperature and becomes gelatinous after being injected in the submucosa of the digestive tract. The present study focuses on preparing the thermo-sensitive binary hydrogels system and testing its capacity in mucosal lifting and its role in the endoscopic submucosal dissection procedure.
Methods
Various concentrations of poloxamer 407 and poloxamer 188 were added to normal saline. The gelation temperature viscosity of the thermo-sensitive binary hydrogels system was measured to choose the best formula. The thermo-sensitive binary hydrogels system and normal saline were first compared in extracted porcine stomach. For in vivo study, the thermo-sensitive binary hydrogels system and normal saline were compared for facilitating the endoscopic submucosal dissection procedure.
Results
Among the 46 kinds of thermo-sensitive binary hydrogels system, gelation temperatures of the thermo-sensitive binary hydrogels system I (poloxamer 407/poloxamer 188, 17%/0.5%, w/w) and the thermo-sensitive binary hydrogels system II (poloxamer 407/poloxamer 188, 18%/2%, w/w) were among the ideal range of gelation temperature. The injecting pressure in vitro study of thermo-sensitive binary hydrogels system II was significantly higher than that of thermo-sensitive binary hydrogels system I and normal saline (p < 0.001). Sixteen gastric endoscopic submucosal dissection procedures were performed in a porcine model. The initial volume of normal saline injection (13.88 ± 3.91 ml vs 5.88 ± 3.44 ml, p = 0.001) was significantly larger than the thermo-sensitive binary hydrogels system group. The postoperative wound showed a significant difference in the two groups (p = 0.023) indicating that the thermo-sensitive binary hydrogels system can create a cleaner wound.
Conclusions
Considering the gelation temperature, viscosity, injection pressure, and the height of the mucosal elevation, the thermo-sensitive binary hydrogels system I was the better submucosal injection solution.
Keywords
Key summary
Summarize the established knowledge on this subject
There are various types of submucosal injection solutions for use during endoscopic submucosal dissection (ESD). Normal saline remains the most used solution for mucosal lifting. It diffuses very fast during the procedure and requires repeated injection.
What are the significant and/or new findings of this study?
The thermo-sensitive binary hydrogels system (TBHS) composed of poloxamer 407 (P407) and poloxamer 188 (P188) requires fewer submucosal injections and provides a cleaner wound than normal saline during the ESD procedure.
Introduction
The endoscopic submucosal dissection (ESD) procedure increases the complexity of techniques and the risk of adverse events such as bleeding and perforation compared with endoscopic mucosal resection (EMR).1,2 Assorted safe procedures have been developed to decrease the rate of adverse events. 3 Making an optimal and lasting submucosal fluid cushion to lift the mucosa from the muscularis propria layer is regarded as the best approach to reduce intraoperative or postoperative adverse events. Normal saline (NS) is the most commonly used solution for submucosal injection. The duration of mucosal lifting, however, is limited and intraoperative repeated injections would be inevitable for larger lesions.
The temperature-sensitive hydrogel comes to mind as a way to overcome these problems and might be an ideal solution for submucosal injection. One of the unique properties of it is that it can transform from the fluid state to the gel state in response to the specific temperature, called gelation temperature. Poloxamers are a group of copolymers consisting of polyethylene oxide (PEO) and polypropylene oxide (PPO) units. This group was studied as a drug-delivery system in the late 1950s.4–6
In our research, we tried to develop a thermo-sensitive binary hydrogels system (TBHS) composed of poloxamer 407 (P407; PEO100-PPO70-PEO100) and poloxamer 188 (P188; PEO76-PPO29-PEO76). By adjusting the proportion and concentration of them, we could make the TBHS meet the requirement of submucosal injection. After that, the feasibility, safety, and efficacy of the TBHS would be evaluated in the extracted or living porcine stomach.
Materials and methods
Materials
P407 and P188 were purchased from the BASF Chemical Company. The ideal range of gelation temperature for the TBHS is 25–30℃ since the TBHS should remain liquid and begin to be gelatinized after it is injected in the submucosal part of the digestive tract. All attempts at ESD were performed with a single-channel gastroscope (GIF-H260, Olympus) and hook knife (KD-620LR, Olympus). A 4 mm long transparent hood (D-201–11304; Olympus) was attached to the tip of endoscope for a better visualization and to facilitate dissection. Other equipment included injection needles (23G, Boston), grasping forceps (FG-8U-1, Olympus), snares (SD-230U-20, Olympus), hot biopsy forceps (FD-410LR, Olympus), and clips (HX-610-90, Olympus). A VIO 200D (ERBE, Germany) electrosurgical generator was used as a working station.
All other items of apparatus used were obtained from the Endoscopy Center of Zhongshan Hospital. The experimental protocols were approved by the Animal Care and Use Committee of Zhongshan Hospital, Fudan University (2017-040). All the experimental operations were conducted in the animal laboratory in Zhongshan Hospital.
Animals
Fresh porcine stomachs were purchased from the local slaughter house within two hours after the pigs were sacrificed. Eight miniature pigs (age, 5–6 months old; bodyweight, 25–30 kg) were provided by the Animal Lab of Zhongshan Hospital.
Preparation for TBHS
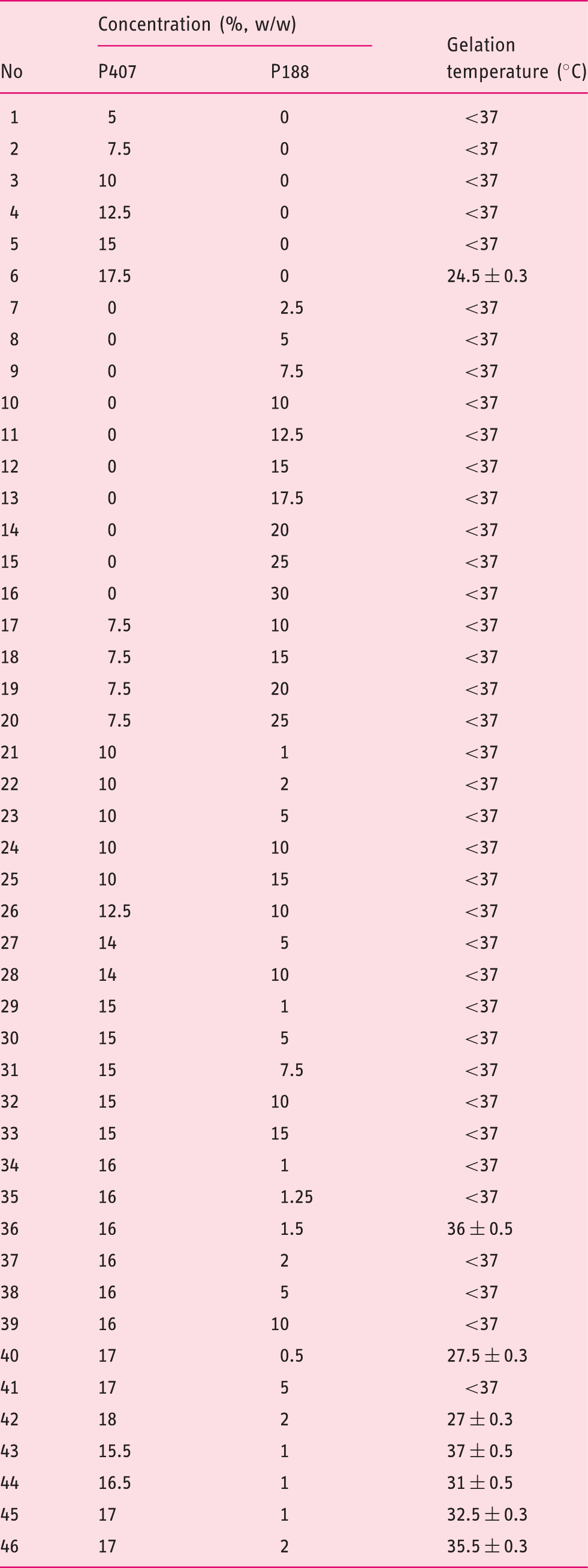
Forty-six different kinds of TBHS and their gelation temperature.
Measurement of the gelation temperature and viscosity
The TBHS with different proportions was applied. The tube inversion method was used to measure gelation temperature.7,8 Two millilitres of the TBHS were sealed in a glass tube. The tube was then heated in the water bath from 15 ℃ to 37 ℃. The temperature of the water bath was raised 0.5 ℃ per min. The gelation temperature was confirmed when there was no fluid after the tube was inverted. The viscosity was measured using the Ubbelodhe viscometer. 9
In vitro study of mucosal elevation capacity in extracted porcine stomachs
NS was tested for comparison with TBHS in our research. We used the upper third part of the porcine stomach due to its thickness and similar histology to the human stomach. 10 The stomach was cut into 5*5 cm squares and stretched flat on a corkboard with pins. A 20 ml syringe connected with a 23-gauge injection needle was applied to inject 5 ml of each solution into the submucosa layer. The injection pressure of the material was measured by pressure gauge (Encore 26 Inflation Device, Boston Scientific, USA). The injections were repeated 10 times and the height of the submucosal cushion was recorded. During the procedure, the extracted porcine stomach was placed in the water bath of 37 ℃.
In vivo study of ESD
To preclude inter-procedure bias, all the ESD procedures were performed by a single endoscopist (M-Y Cai) who has performed more than 200 ESD procedures on gastric mucosal and submucosal lesions. The upper third of the porcine stomach was chosen as the target position for the ESD. One NS ESD and one TBHS ESD were performed in each animal.
A trained veterinarian conducted all the animal preparation and management during the experiment period. Before the ESD procedure, the pigs were fasted for 24 h. General anesthesia with endotracheal intubation was administered during the ESD procedure.
After making several marking dots with the hook knife around the simulated lesion, the submucosal injection solution was injected into the submucosa. The amount of the solution injected depended on the elevation of mucosa. The mucosa was circumferentially pre-cut 5 mm outside the marking dots. Direct dissection of the submucosal layer beneath the lesion was then performed under direct vision to achieve en bloc resection of the specimen. The submucosal injection solution was injected repeatedly during the dissection if necessary. After the removal of the lesion, the postoperative wound was rated by four grades based on visual judgement: grade I, a clear wound without visible bleeding; grade II, oozing a small amount of blood without active bleeding; grade III, moderate amount of oozing requiring washing the wound; grade IV, profuse oozing requiring use of a hemostatic procedure. The hot biopsy forceps were then used to stop the bleeding. The endo cut mode (effect 3, duration 2, interval 4) was used for cutting, and the forced coagulation mode at 50 W (effect 2) was used for precut coagulation and hemostatic treatment. The ESD procedure time was defined as the beginning of the submucosal injection to the extraction of the resected lesion. After the procedure, the animal was kept fasting for one day and a semi-fluid diet for the next three days. The postoperative wounds were observed endoscopically one week after ESD procedures. Experimental animals were euthanized after endoscopic examination by authorized veterinarian.
Statistical analysis
Statistical analysis of the chronological changes in height of the submucosal fluid cushion was carried out by using an analysis of variance with repeated measures. The student's t test was used for groups comparison of quantitative variables and chi-square test was used for comparison of categorical variables. Statistical analysis was conducted using SPSS software (IBM SPSS Statistics 18; SPSS, Chicago, USA), and alpha was set at 0.05, two-sided.
Results
The gelation temperature and viscosity of the TBHS
The ideal range of gelation temperature for submucosal injection is 25–30 ℃. If the gelation temperature is lower than 25 ℃, the TBHS may switch to gel at room temperature and thus its high viscosity may lead to difficulty in submucosal injection. The gelation temperature should be also lower than 30 ℃ since the TBHS should transfer to a gel state immediately after it is injected into the submucosal area of the digestive tract. In this study, we successfully developed 46 kinds of TBHS with different concentrations of poloxamers (Table 1). The gelation temperature of sample no. 40 (P407/P188, 17%/0.5%, w/w) and no. 42 (P407/P188, 18%/2%, w/w) was within the ideal range of gelation temperature (25–30 ℃).
The viscosity of these two TBHS combinations (Figure 1) has shown a rapid increase from 25 ℃ to 35 ℃. This means that after being injected into the submucosal part of the digestive tract, the TBHS may form a long-lasting gel state because of their high viscosity.
The viscosity of no. 40 and no. 42 TBHS between 20–37℃.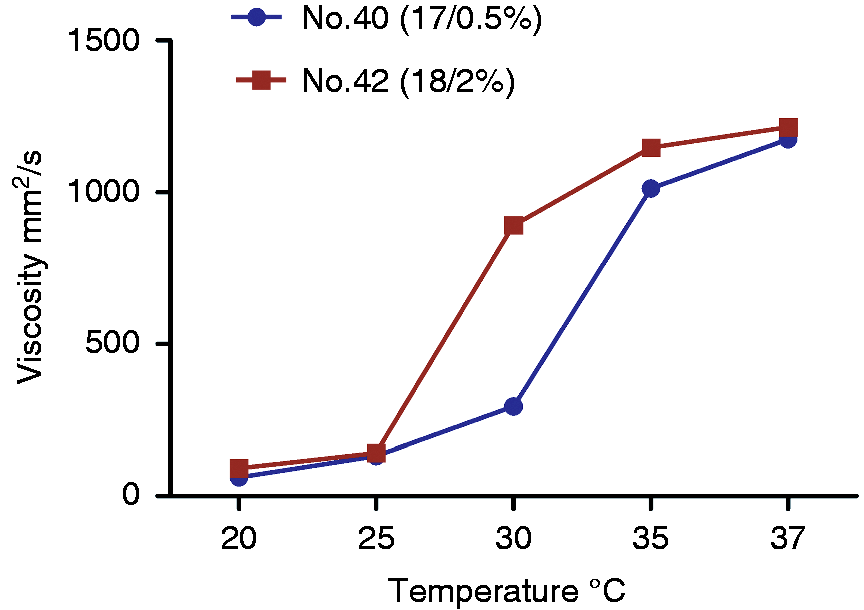
Efficacy comparison for mucosal elevation in vitro
The TBHS I (no. 40) and TBHS II (no. 42) were injected into the submucosa of the extracted porcine stomach to compare their effect on mucosal elevation with NS. The average injecting pressure of TBHS I, II, and NS were 7.4 ± 0.8, 19.2 ± 1.0, and 1.0 ± 0.0 atm, respectively (Figure 2(a)). The injecting pressure of TBHS II was significantly higher than TBHS I and NS (p < 0.05). The TBHS produced better mucosal elevation as expected (Figure 2(b)). The height of the mucosal elevation upon injection of both TBHS solutions lasted significantly longer than that formed by NS (p < 0.05). There is also a significant difference between the mucosal elevations of the two different TBHS solutions (p < 0.05). When we compared the mucosal elevation of the two TBHS solutions (Figure 2(c)), the TBHS II can maintain higher elevation at 45 and 60 min after the submucosal injection (p < 0.05), while there was no significant difference at 0, 15, 30 and 90 min after injection.
(a) The average injection pressure of the submucosal injection between the three groups in extracted porcine stomach models; (b) the height of the mucosal elevation after the submucosal injection between the three groups in extracted porcine stomach models; (c) the height of the mucosal elevation of each thermo-sensitive binary hydrogels system (TBHS) in extracted porcine stomach models. NS: normal saline.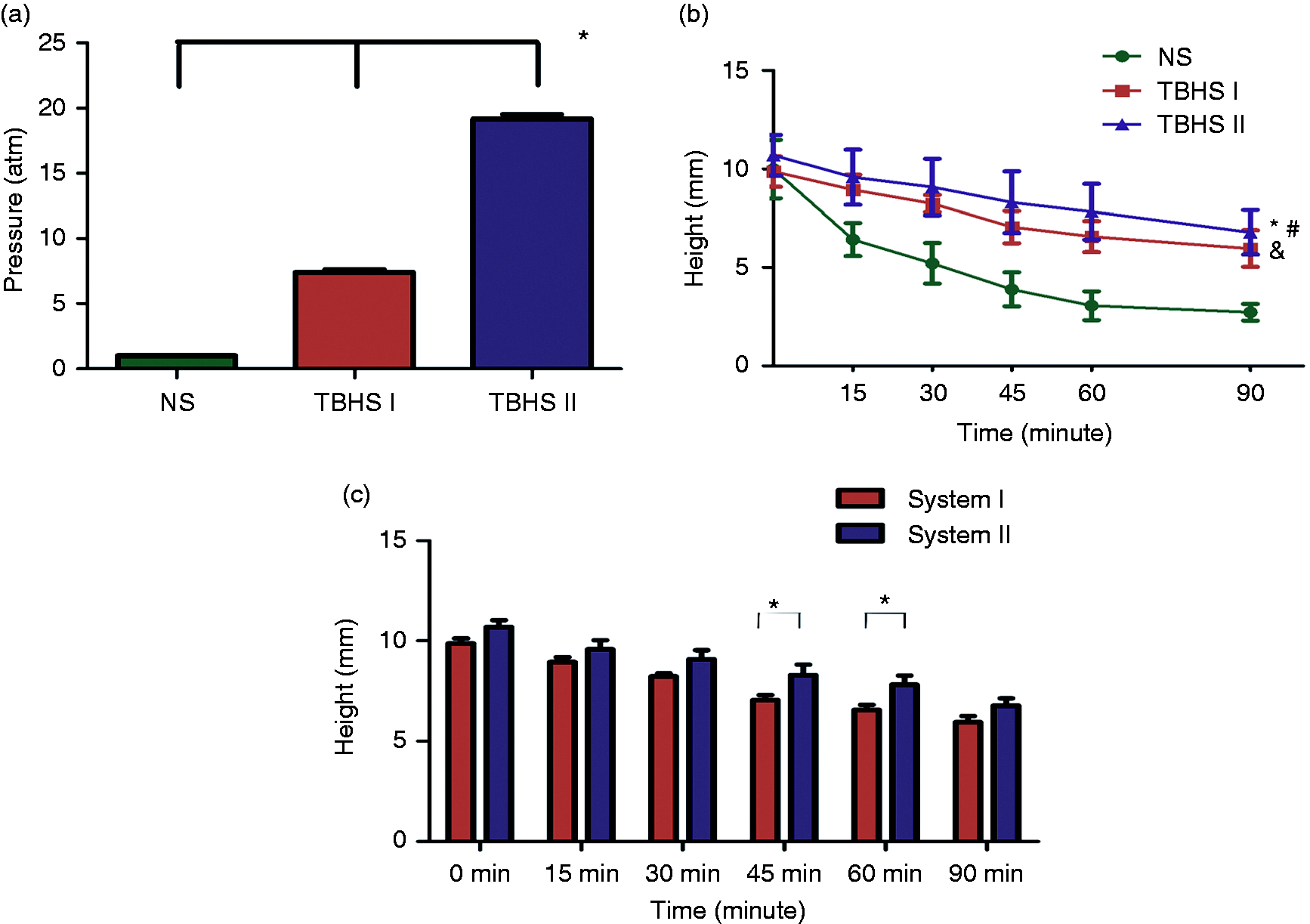
The ESD procedure
A syringe attached with a pressure gauge (Encore 26 Inflation Device, Boston Scientific, USA) was used to perform the submucosal injection. Considering the average injection pressure and the height of the mucosal elevation, the TBHS I was the better submucosal injection solution. A total of 16 gastric ESD procedures were performed. During the ESD procedure facilitated by NS, the intraoperative repeat injection was inevitable since the mucosal elevation was transient. The TBHS-facilitated procedure is shown in Figure 3. The submucosal gel cushion lasted longer than NS so that repeated injection was rarely needed during the operation. All the procedural information of the NS group and TBHS group is summarized in the Table 2.
Endoscopic images of endoscopic submucosal dissection (ESD) procedure with thermo-sensitive binary hydrogels system (TBHS). (a) Submucosal injection; (b) the submucosal cushion of TBHS; (c) to (e) endoscopic submucosal dissection with ESD knives; (f) the postoperative wound. Comparison of endoscopic submucosal dissection (ESD) procedure-related parameters between the two groups. SD: standard deviation; TBHS: thermo-sensitive binary hydrogels system.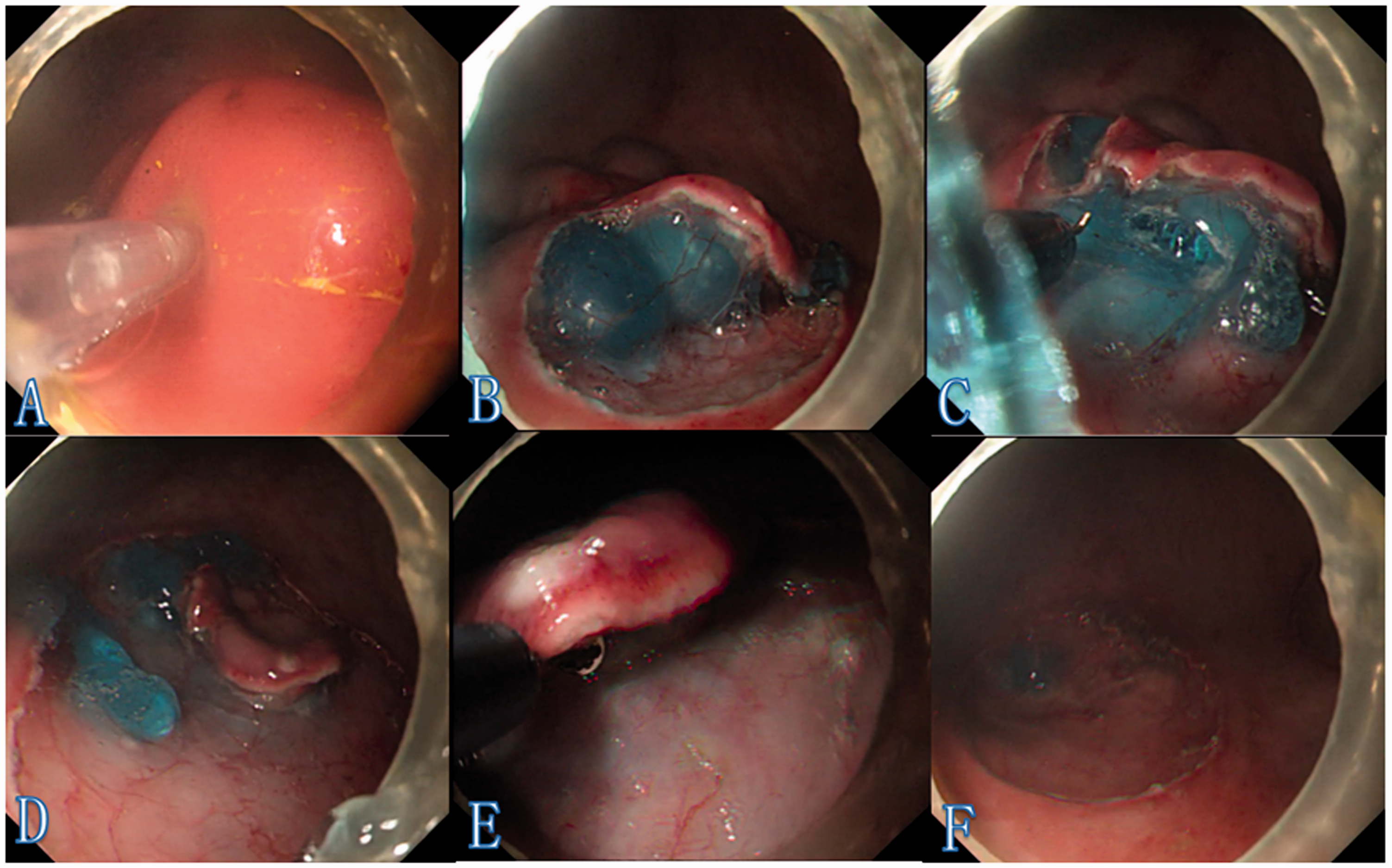
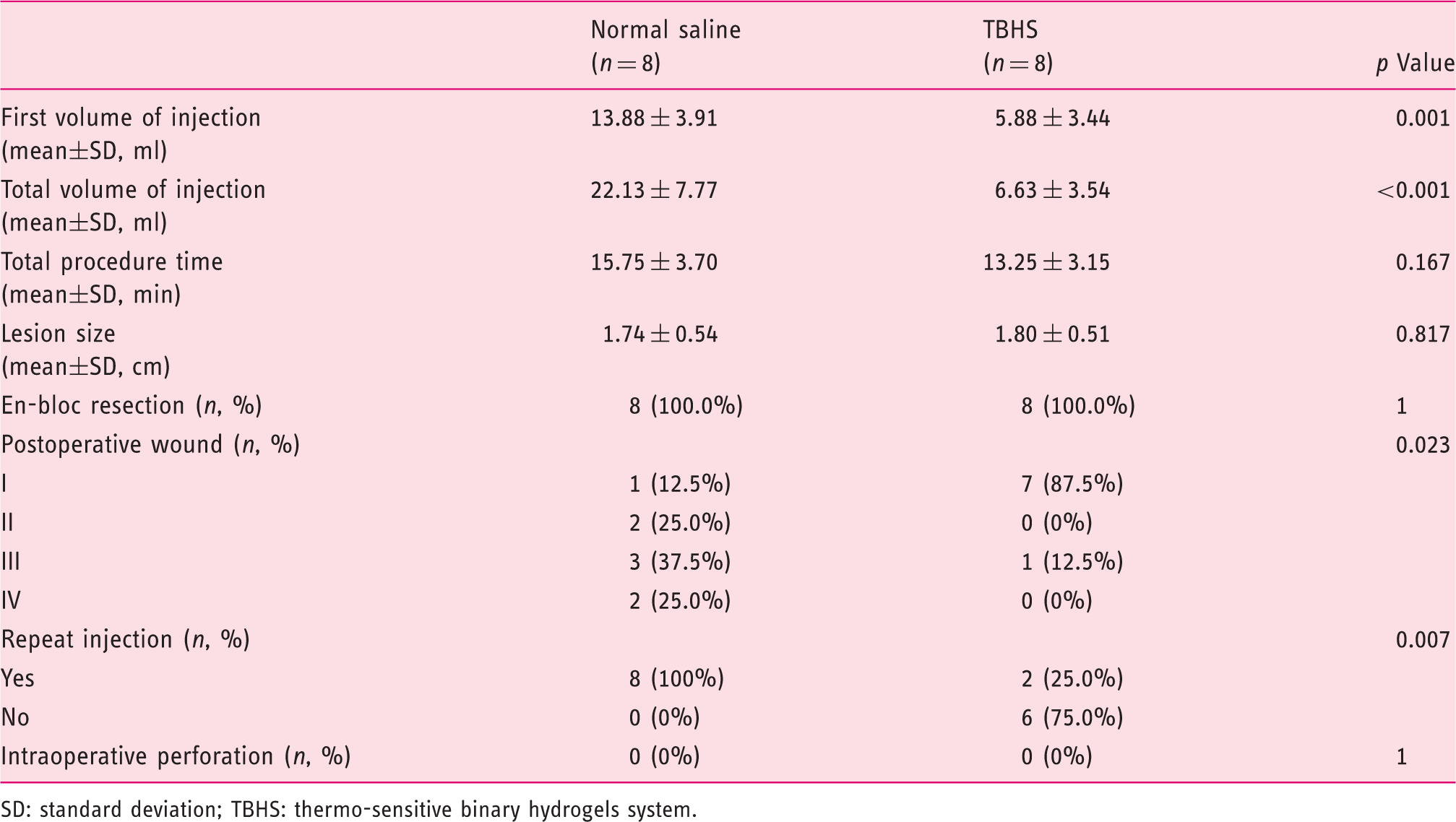
En bloc resection was achieved for all the lesions. There was no significant difference in the total procedure time between the two groups (15.75 ± 3.70 min vs 13.25 ± 3.15 min, p = 0.167). In the NS group, the initial volume of injection (13.88 ± 3.91 ml vs 5.88 ±3.44 ml, p = 0.001) was significantly larger than the TBHS group, suggesting that more volume of NS is needed to create a sufficient submucosal elevation. TBHS could simplify the ESD procedure. During the procedures, only two TBHS cases (25%) needed a repeat injection while all eight NS cases (100%) needed a repeat injection. Most of these repeated injections were performed during the dissection of the submucosal lesion underneath the selected lesion. Thus, the total volume of injection (22.13 ± 7.77 ml vs 6.63 ± 3.54 ml, p < 0.001) was significantly different in these two groups.
The endoscopic postoperative wounds in the NS group were graded as follows: grade I, 1/8 (12.5%); grade II, 2/8 (25.0%); grade III, 3/8 (37.5%) and grade IV, 2/8 (25.0%). In comparison, in the TBHS group, 7/8 (87.5%) were grade I and 1/8 (12.5%) were grade III. The postoperative wound showed a significant difference in the two groups (p = 0.023).
Discussion
In the past few years, scientists have developed a new submucosal injection solution mainly based on two features of the material: osmolality and viscosity.11–14 Although hypertonic solutions may achieve better lesion lifting, Fujishiro et al. found that they might cause not only mucosal damage but also muscularis propria damage due to its high osmolality. 15 This might hold off the healing of postoperative wound and contribute to inaccurate pathological assessment. Sodium hyaluronate provides the best mucosal lifting according to the previous literature.16,17 However, Matsui et al. reported that the use of sodium hyaluronate might exacerbate the spread of residual tumor cells. 18
Taking the viscosity of the material into account, injectable hydrogels have been applied as a submucosal injection solution in several researches. PS137-25, a part of a family of water-soluble poloxamers, was believed to provide a more durable submucosal elevation. 19 But it still needs a balloon dilator gun to facilitate its effect during the injection. Photocrosslinkable chitosan is a viscous solution which can be converted into an insoluble hydrogel by being exposed to ultraviolet irradiation for 30 s. Kumano et al. found that photocrosslinkable chitosan hydrogel is more reliable in ESD procedure than sodium hyaluronate. 20 Obviously, the procedure is complicated since it requires an ultraviolet lamp system.
In the present study, we believe the TBHS composed of P407 and P188 met all the requirements of an ideal submucosal injection solution. The Food and Drug Administration (FDA) guide has listed P407 as an inactive ingredient used in inhalation, oral solution, suspension, ophthalmic or topical formulations. 21 P407 aqueous solution remains in the fluid state and will turn into the gel state above the gelation temperature. This attractive property is thermoreversible and the gelation temperature increases when P407 concentration decreases. 5 The gelation temperature of the TBHS is the most important parameter. It is the temperature at which the TBHS switches to gel from liquid. The combination of P407 and P188 enables the whole hydrogel system to meet the optimal gelation temperature and increase the bioadhesive properties. Akkari et al. reported their binary hydrogels system of P407 and P188 to deliver ropivacaine for the treatment of post-operative pain. 22 The binary hydrogels system caused lower vitro cytotoxic effects, and increased the duration of analgesia. Considering the information from previous related studies, we thought the TBHS composed of P407 and P188 might be an excellent submucosal injection solution.
The TBHS used for ESD has several significant features. The most important feature is that it lasts longer than NS with its high viscosity. After being injected to the submucosal layer, the TBHS converts from liquid state to the solid and high viscosity submucosal gel cushion when it is above the gelation temperature. The cushion made of gel can last longer because it rarely diffuses out of the injection area. In our research, there was no significant difference in the total ESD procedure time between the two groups. The main reason attributed to this is the relatively small lesion in porcine stomach resected in the procedure. Besides, the operator also reduced the operation time with her proficient skills. In fact, a fresh hand might be needed more times for repeated injection during the procedure using NS solutions.
The use of TBHS may reduce intraoperative hemorrhage and lead to a clear visual field. Compared with the NS group, the postoperative wound in the TBHS group was clearer with minimal oozing of blood. The use of the TBHS may also help the endoscopists recognize the vessel clearly (Figure 3(b)). The vessels in the submucosal layer are mainly interspersed in the loose connective tissue. They are probably squeezed out by the solid submucosal cushion made by the gel so that the vessels are covered on the surface of the submucosal cushion. The maintenance of the clear postoperative wound can also save time to achieve hemostasis. Zhang et al. found that P407 could protect the diaphragm from thermal injury in the microwave ablation of hepatic tumors adjacent to the diaphragm. 23 During the ESD procedure, the gel protective layer could reduce electrocautery injury when dissecting the submucosal layer. After the ESD procedure, there is still some TBHS left on the postoperative wound. It reminds us that the initial use of this hydrogel system is for site-specific drug delivery. 24 We might use the TBHS as a drug delivery system to accelerate the wound healing and reduce the postoperative adverse events. The specific formula still needs further study.
During the ESD procedure facilitated by TBHS, we found the unique phenomenon that might be called blunt mechanical dissection induced by the submucosal cushion. The mucosal lesion was self-dissected from the musclaris propria and thus further submucosal dissection was no longer needed. Blunt mechanical dissection along natural lines of cleavage is recognized as a safer and easier approach during surgical dissection of fascial planes. 25 In endoscopic resection, excessive electrosurgical incisions or dissections might cause damage to the muscularis propria by cauterization and the blood supply nearby to the lesion may suffer greater damage. The thermal injury of the muscularis propria and lack of blood supply can lead to perforation. But, by using the TBHS, such risks can be reduced or even avoided, and therefore the level of postoperative adverse events might be decreased.
Compared with hyaluronic acid solution (Hyalgan, US$66/ml), the use of the binary hydrogels system can reduce patient expense. The cost of the material will be reduced to US$2 per ml.
However, the present study has several limitations. First, all the operations were practiced in the porcine stomach model. Esophageal or colonic ESD was regarded as more challenging than gastric ESD due to the thinner wall compared with stomach. Besides, the sample size of this study is limited. A randomized controlled trial might be done in the future.
In conclusion, TBHS has proved feasible and safe for submucosal injection in the porcine gastric ESD, TBHS can simplify ESD procedure by reducing the total submucosal injection volume and repeated injection times. Further studies in clinical settings are awaited.
Footnotes
Declaration of conflicting interests
The authors declare that there is no conflict of interests regarding the publication of this article.
Ethics approval
The experimental protocols were approved by the Animal Care and Use Committee of Zhongshan Hospital, Fudan University (2017-040).
Funding
This study was supported by the Major Project of Shanghai Municipal Science and Technology (16411950400), National Natural Science Foundation of China (81470811,81670483 and Shanghai Engineering and Research Center of Diagnostic and Therapeutic Endoscopy (16DZ2280900).
Informed consent
Not applicable.