
Abstract
This
Keywords
Introduction
Chronic mesenteric ischemia (CMI) requires timely diagnosis and treatment to prevent the development of acute mesenteric ischemia, which is associated with high morbidity and mortality. CMI is a diagnosis that is difficult to establish as symptoms are highly variable and diagnostic tests may be inconclusive. Recently, three guidelines for CMI management have been published: a clinical practice guideline of the European Society of Vascular Surgery (ESVS), 1 criteria on radiological management by the American College of Radiology (ACR) 2 and quality improvement guidelines for endovascular revascularization by the Society of Interventional Radiology (SIR). 3 Gastroenterology guidelines on CMI are lacking. This review provides an overview of available literature on the clinical management of patients suspected of CMI with focus on occlusive arterial CMI.
Clinical presentation
CMI is defined as insufficient blood supply to the gastrointestinal (GI) tract resulting in ischemic symptoms with duration of at least three months. 1 Typical symptoms of CMI include postprandial abdominal pain with food aversion and weight loss. The abdominal pain is classically located in the mid-abdomen or epigastrium and starts usually 20–30 minutes after a meal with a duration of 1–2 hours. Atypical symptoms are constant abdominal discomfort, nausea, vomiting, diarrhea or constipation. 1 Abdominal bruit may be present during physical examination; however, the “classic CMI triad” of postprandial abdominal pain, weight loss and abdominal bruit is only present in 16–22% of CMI patients.4,5
Etiology
Atherosclerotic stenosis of one or more mesenteric arteries is the cause in >90% of CMI cases. 6 Less frequently CMI is caused by vasculitis. Three mesenteric arteries provide blood supply to the intestines: the celiac artery (CA), superior mesenteric artery (SMA) and inferior mesenteric artery (IMA). An extensive collateral circulation exists between these arteries. Asymptomatic mesenteric stenoses are common in the general population and prevalence increases with age. The prevalence of asymptomatic CA and/or SMA stenosis is reported as 3% in patients under 65 years and 18% in patients older than 65 years. 7
Multi-vessel mesenteric stenosis causing CMI is a well-accepted conception, whereas insufficient blood supply caused by isolated mesenteric stenosis is thought to be limited because of abundant collaterals. If the collateral circulation is insufficient, however, revascularization of a single-vessel stenosis will result in symptom relief.5,8–10
The most common cause of isolated CA stenosis is median arcuate ligament syndrome (MALS): anatomical eccentric compression of the CA and/or celiac ganglion by the median arcuate ligament (MAL) and diaphragmatic crura.
11
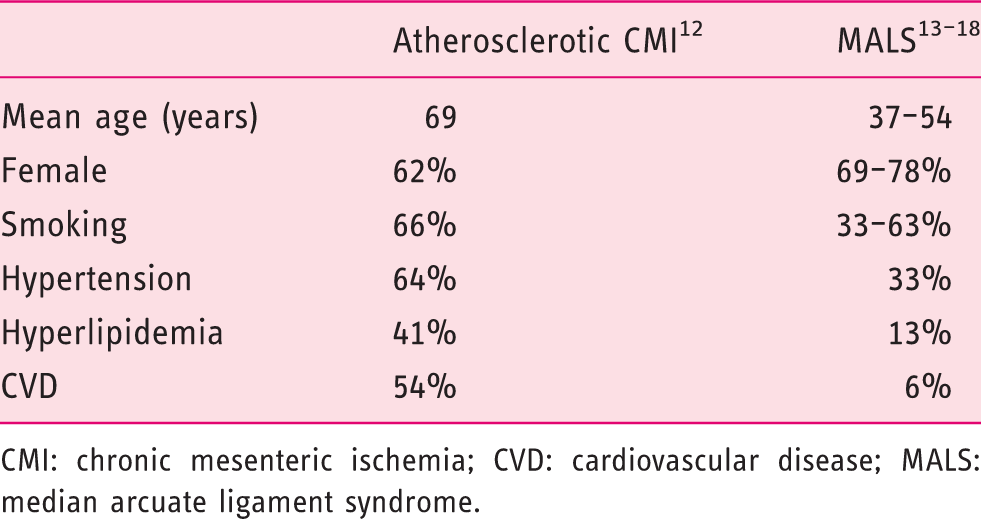
The degree of stenosis caused by the MAL depends on the respiratory cycle. The MAL moves caudally during inspiration, releasing the compression on the CA and increasing compression during expiration (Figure 1), although compression only during inspiration may be observed as well. Characteristics of patients with CMI differ depending upon the underlying cause being MALS or atherosclerosis (Table 1).12–18
A 48-year-old woman presented with postprandial abdominal pain and 10-kg weight loss. Computed tomography angiography (CTA) showed compression of the celiac artery (CA), with increased compression on expiration (a) and less compression on inspiration (b). Patient was planned for surgical release of CA. After successful release, patient had gained 5 kg in weight and was symptom free. CTA 11 months after surgery showed an open CA on expiration (c) and on inpiration (d). Reported prevalence of characteristics of patients with atherosclerotic CMI versus patients with CMI based on MALS. CMI: chronic mesenteric ischemia; CVD: cardiovascular disease; MALS: median arcuate ligament syndrome.
Chronic non-occlusive ischemia (NOMI) or “migraine abdominale” 19 is characterized by symptoms of CMI in the absence of a vascular stenosis and is diagnosed in up to 13–16% of all CMI patients. 10 Several pathophysiological mechanisms causing chronic NOMI have been suggested: underlying conditions such as cardiac and pulmonic insufficiency, shunts, occlusion of smaller arteries due to spasms or micro-emboli, and autonomic dysfunction. Therapy is directed to ameliorate the adverse effects of the underlying pathophysiological mechanism that is vasodilating medication in case of autonomic dysfunction or optimizing oxygen supply to the GI tract in case of underlying cardiac or pulmonic disease. Successful treatment of these patients, however, is challenging because the etiology of chronic NOMI is not fully unraveled yet.
Diagnosis
In the absence of a golden standard test, the diagnosis of CMI is established by consensus in a multidisciplinary meeting attended by vascular surgeons, gastroenterologists and (interventional) radiologists.1,20 The consensus diagnosis is based on clinical symptoms, radiological evaluation of the mesenteric vasculature and, if available, functional assessment of mucosal ischemia.21–23 The value of symptoms alone is limited for the prediction of the diagnosis of CMI.4,24,25
Computed tomography angiography (CTA) is the primary imaging modality in patients with a moderate or high suspicion of CMI to assess the mesenteric arteries and to detect other intra-abdominal pathology according to the ESVS guidelines. 1 CTA depicts various atherosclerotic plaque components such as soft plaque and calcifications with a sensitivity for mesenteric artery stenosis of 100% and a specificity of 95%. 26 Current magnetic resonance angiography (MRA) techniques seem not as accurate as CTA, especially for the IMA and smaller branch vessels. 27 When CTA is not feasible, that is in the presence of contrast allergy or renal insufficiency, MRA can be used as an alternative according to the ACR guidelines. 2 Duplex ultrasound (DUS) can be used as first screening imaging modality to identify a mesenteric artery stenosis. DUS identifies a ≥ 70% CA stenosis with a sensitivity of 72–100% and a specificity of 77–90% and a ≥ 70% SMA stenosis with a sensitivity of 72–100% and a specificity of 84–98%.3,28 However, DUS is operator dependent, technically challenging and the flow velocities of the evaluated artery could be influenced by respiration, the presence of concomitant stenosis in other mesenteric vessels, and existing stents. Digital subtraction angiography (DSA) is reserved for treatment of occlusive mesenteric artery disease and is replaced by CTA as diagnostic modality. Plain abdominal X-ray has no role in the diagnosis of CMI.
Dynamic imaging is important to detect a CA stenosis caused by MALS because the grade of stenosis varies with respiration in contrast to atherosclerotic stenosis. CTA, MRA, DUS or DSA during both inspiration and expiration phases are sufficient.
A functional test to prove actual GI ischemia is needed because of the high prevalence of mesenteric stenosis in the asymptomatic general population and the large overlap of symptoms of CMI with many other disorders. Visible light spectroscopy (VLS) performed during upper endoscopy allows measuring of the oxygen saturation of the upper GI mucosa using a fiber-optic catheter passed through the accessory channel of the endoscope connected to the VLS oximeter (T-Stat 303 Microvascular Oximeter; Spectros, Portola Valley, California).
29
The sensitivity of VLS measurements for the diagnosis of CMI is 90% and the specificity is 60%.
30
The VLS measurements are reproducible in clinical practice with fair to good intraobserver and interobsever reliability.
31
Tonometry is another functional test that measures luminal partial pressure of carbon dioxide (PCO2) by a nasogastric and nasojejunal catheter attached to a capnography (Tonocap). Luminal PCO2 increases during mesenteric ischemia. Exercise tonometry is performed during a bicycle test (sensitivity 78%, specificity 92%
10
) and 24-hour tonometry is performed using test meals as provocation (sensitivity 76%, specificity 94%
23
). A functional test is not needed in the work-up of the most common CMI suspected patients with typical symptoms and multi-vessel disease (Figure 2). However, especially in the work-up of single-vessel disease a functional test is a prerequisite. It is therefore recommended to refer these patients to a specialized center to undergo functional testing. Research is in progress to develop simple and reliable functional tests that can be widely applied.
Algorithm for clinical management of chronic mesenteric ischemia.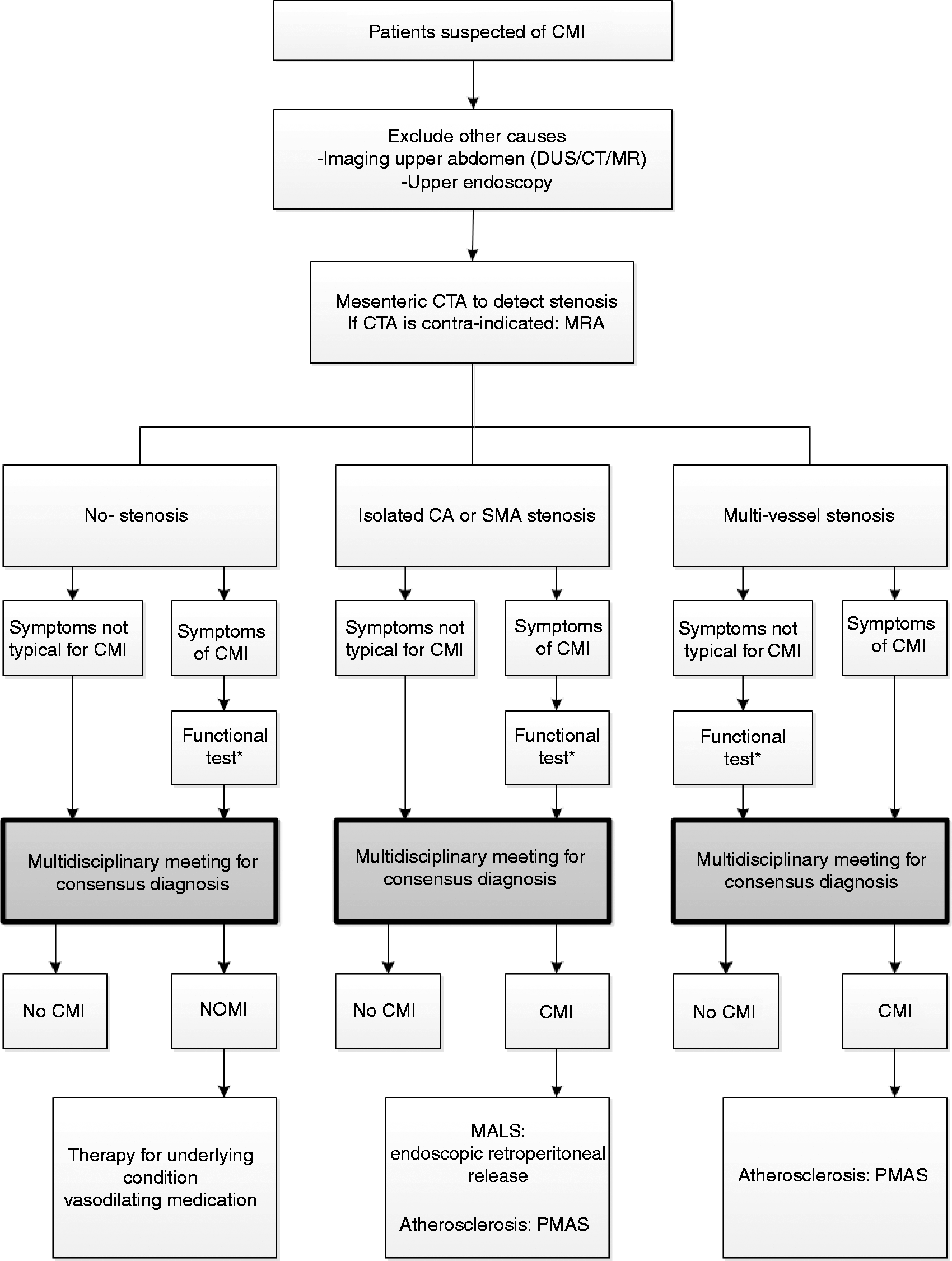
Laboratory tests such as leukocytes, D-dimer, lactate and C-reactive protein are not useful for detection of CMI.1,32,33 Because CMI is a state of transient ischemia episodes induced by eating, fasted marker levels are presumably not sufficient to indicate CMI. In a study in which several serum markers before and after a meal were determined in patients suspected of CMI, a significant increase of D-dimer was reported in 32 CMI patients after a meal in contrast with 8 patients without CMI. 32 Another study in 49 CMI-suspected patients reported a significant increase in intestinal fatty acid–binding protein levels in patients with a positive tonometry result after a meal in contrast with patients with a normal response after a meal. 33 Further research and larger studies are needed to potentially identify a sensitive and specific biomarker for detecting CMI.
In contrast to a diagnosis of acute ischemic colitis, endoscopic assessment of the mucosa by visual appraisal or taking biopsies plays no crucial role in detecting CMI. In CMI patients atrophy of the duodenal mucosa and non-Helicobacter pylori/non-nonsteroidal anti-inflammatory drug gastric or duodenal ulcers are observed in a minority of cases. 24 Histological examination of biopsy samples are not discriminative for the diagnosis of CMI. 34 Nevertheless, an upper endoscopy remains indicated in CMI-suspected patients to exclude alternative diagnoses, such as peptic ulcer.
Multi-vessel stenoses and classic symptoms will lead to a straightforward diagnosis of CMI. In case of single-vessel disease careful investigation for alternative causes is warranted. 1 Exclusion of other etiologies by imaging of the upper abdomen (DUS/computed tomography (CT)/magnetic resonance (MR)) for gallstones and pancreatitis and upper endoscopy in patients suspected of CMI is important to prevent overtreatment (Figure 2). When a consensus diagnosis of occlusive CMI is established in the multidisciplinary meeting, patients are planned for revascularization therapy. A definitive diagnosis of CMI is proven when technically successful treatment results in durable symptom relief.
Therapy
Revascularization is indicated in patients with occlusive CMI to relieve symptoms, improve quality of life, restore normal weight and improve survival by preventing bowel infarction (acute-on-chronic mesenteric ischemia).
1
The challenge is to select the patient with mesenteric stenosis who will benefit from treatment. Revascularization is accepted in case of symptomatic multi-vessel stenosis (Figure 3). Because the presence of the mesenteric collateral circulation is assumed to prevent single-vessel CMI, revascularization is up for discussion in case of single-vessel stenosis (Figure 1 and Figure 4). However, after careful selection by multidisciplinary consensus and functional assessment persistent symptom relief was reported in 73% of symptomatic patients diagnosed with single-vessel CMI based on a solitary CA or SMA stenosis.
9
A 69-year-old woman presented with postprandial abdominal pain and 10-kg weight loss over three months. A significant stenosis of the celiac artery (CA) and superior mesenteric artery (SMA) was shown on computed tomography angiography (CTA) (a). A consensus diagnosis of multi-vessel chronic mesenteric ischemia was established and patient was planned for endovascular revascularization. The CA and SMA were successfully stented. CTA 6 months after revascularization showed open stents (b). The patient was free of symptoms and her weight increased by 12 kg. A 50-year-old man presented with postprandial abdominal pain and 13-kg weight loss. Computed tomography angiography (CTA) showed a significant stenosis of the superior mesenteric artery (SMA) and <50% celiac artery stenosis (a). His mucosal saturation levels were decreased as detected by visible light spectroscopy. A consensus diagnosis of single-vessel chronic mesenteric ischemia was established and patient was planned for stent placement of the SMA. CTA 6 months after revascularization showed an open SMA stent (b). The patient was free of symptoms and his weight increased by 7 kg.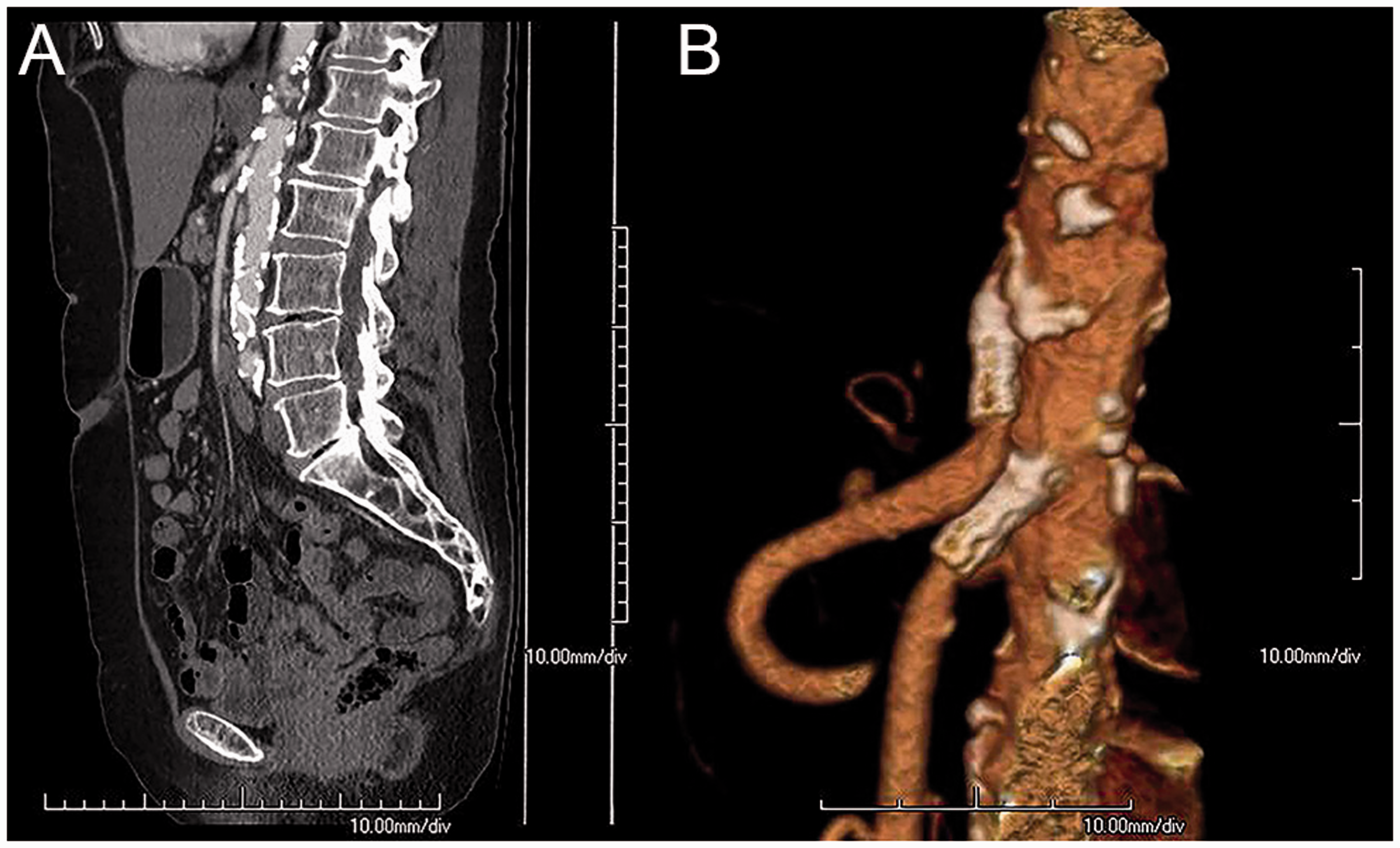

Open surgical revascularization has been the standard therapy modality for years. However, endovascular revascularization is less invasive and has become the therapy of choice in most centers over the past two decades.1–3 The number of endovascular procedures performed for CMI in the USA has increased significantly from 0.6 per million in 2000 to 4.5 per million in 2012 (p < 0.01). 35
Prospective studies comparing percutaneous transluminal angioplasty (PTA) alone with primary stenting are lacking. However, in parallel to renal artery stenosis and the advantage of stent placement over PTA in this patient group, endovascular therapy for mesenteric stenosis consists of stent placement according to the ESVS and SIR guidelines.1,3 Mesenteric stenoses are usually located at the ostium and are therefore prone to recoil after PTA.3,36,37 The endovascular approach is transbrachial or transfemoral, but a transradial approach for percutaneous mesenteric artery stenting (PMAS) is recognized as a safe alternative to the transbrachial approach. 38 Bare-metal stents are standard care but retrospective data have reported better primary patency rates when using covered stents. 39 Outcome of a Dutch randomized multicenter clinical trial (NCT02428582) is currently awaited to confirm the superiority of covered stents for PMAS.
Open surgical revascularization can be considered if endovascular approach has failed, if endovascular revascularization is technically not possible due to extensive occlusion and calcification and contraindications to radiation or contrast media, or if revascularization is needed in young patients with complex non-atherosclerotic lesions caused by vasculitis or mid-aortic syndrome. 1 Open surgical revascularization can be performed antegrade (from the supraceliac aorta), or retrograde (from the iliac artery), or hybrid with open access to the SMA and retrograde stenting. Autogenously revascularization techniques are first choice but a prosthetic conduit can be used as bypass for one or more vessels as well.
Overall technical success rates of endovascular mesenteric revascularization varied from 85–100% versus technical success rates of surgical revascularization of 97–100%.3,6,40 Relative contraindications for endovascular revascularization associated with lower technical success rate and/or increased procedural complications are highly tortuous aorta-iliac arteries, long-segment occlusion, small-diameter distal vessels and heavily calcified stenosis. 3 It should be emphasized that ostial occlusion does not exclude PMAS. In a study of 185 CA and SMA vessels treated with PMAS, 21% of the revascularized vessels (9 CA and 30 SMA) were occluded prior to PMAS. 41
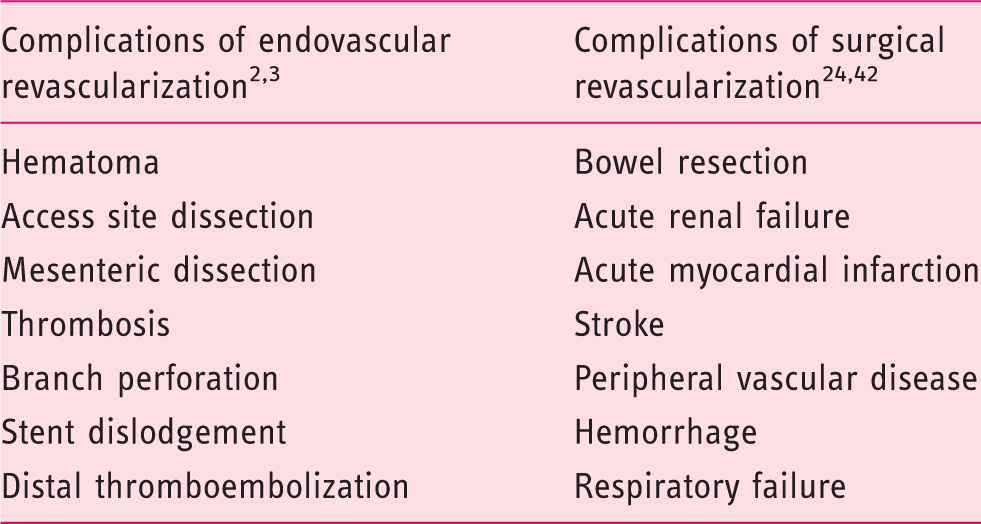
Reported type of complications of mesenteric endovascular revascularization versus mesenteric surgical revascularization.
The therapy for MALS consists of surgical release of the MAL, adjacent crus of the diaphragm and removal of the celiac plexus (Figure 4). If stenosis of the CA persists after adequate surgical release, additional bypass surgery or endovascular therapy is performed. 43 An endoscopic retroperitoneal release is favorable because this has proved feasible and less invasive with comparable short-term results with the open procedure. 17 PMAS is contraindicated as primary therapy for MALS, because of the high risk of stent fracture resulting in restenosis. 3
Clinical outcome after treatment
Repeated follow-up after therapy for CMI might be considered to detect symptomatic restenosis according to the ESVS guidelines. 1 Routine repeated imaging after therapy may show restenosis, but the benefit of treating asymptomatic restenosis is unknown. Antiplatelet therapy is recommended after revascularization and dual antiplatelet therapy may be considered for 3–12 months.1–3
In-stent stenosis can be seen in 28–36% of endovascular-treated patients within 2 years after PMAS. 3 This number is lower after surgical revascularization with 0–25%.6,40 Independent predictors of restenosis after mesenteric revascularization are endovascular revascularization, prior mesenteric intervention, female gender and small (<6 mm) SMA diameter. 44 Severe mesenteric calcification, occlusions, longer lesions and small vessel diameter are associated with an increased risk of distal embolization, restenosis and reinterventions after endovascular revascularization. 40
The 1-year and 5-year primary patency rates and primary assisted patency rates of surgical versus endovascular revascularization for CMI.
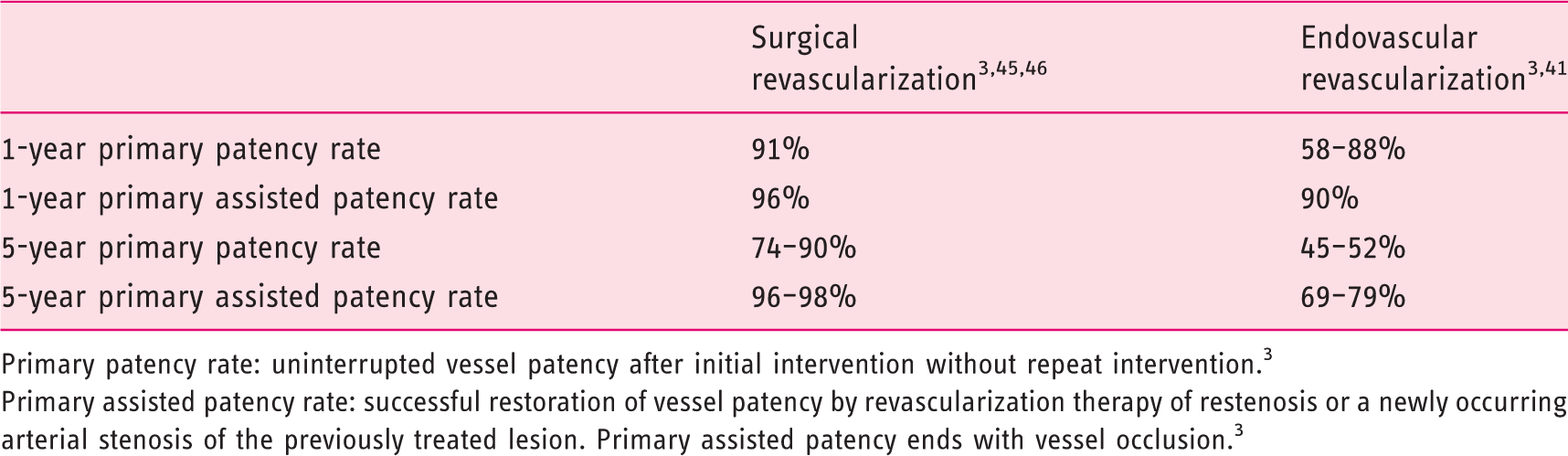
Primary patency rate: uninterrupted vessel patency after initial intervention without repeat intervention. 3
Primary assisted patency rate: successful restoration of vessel patency by revascularization therapy of restenosis or a newly occurring arterial stenosis of the previously treated lesion. Primary assisted patency ends with vessel occlusion. 3
A recently published meta-analysis included 100 observational studies to compare endovascular revascularization (10,679 patients) and open surgical revascularization (8047 patients). 12 Risk of in-hospital complications was significantly increased in the open surgical revascularization group (relative risk (RR) 2.19, 95% CI 1.84–2.60). The risk of 3-year recurrence was lower in the patients treated with open surgery than in the patients treated with endovascular approach (RR 0.47, 95% CI 0.34–0.66). The 3-year survival rate was not significantly different (RR 0.96, 95% CI 0.86–1.07). The ESVS guidelines recommend to offset the superior long-term results of open revascularization against the possible early benefits of endovascular revascularization in the absence of randomized controlled trials. 1
Immediate symptom relief is reported in 90–98% of surgical-treated patients and remains excellent after 5 years with 89–92%. 6 After endovascular revascularization, immediate symptom relief was reported in 87–95%, symptom relief after 3 years in 61–88%, and in 51% after 5 years. 6
A retrospective analysis of prospectively collected data (10,920 endovascular revascularized patients versus 4555 surgical revascularized patients) showed that endovascular revascularization is associated with a significantly lower in-hospital mortality rate of 2.4%, shorter length of hospitalization by 10 days, and lower costs of hospitalization with a saving of $25,000 compared to surgical revascularization. 47
Conclusion
This review provides an overview on the current clinical management of CMI, which is summarized in an algorithm (Figure 2). Although the exact incidence of CMI is unknown, it is expected that the incidence will increase in the upcoming years due to the aging population and the increasing prevalence of cardiovascular disease in Europe. Cardiovascular disease patients have an increased life expectancy due to the improved diagnostics and better therapeutic opportunities, but these patients are also prone to develop mesenteric atherosclerosis. Patients with CMI present usually with GI symptoms. The diagnostic work-up of the patient suspected of CMI and therapeutic management is multidisciplinary. Early diagnosis is important to timely treat, improve quality of life and to prevent acute-on-chronic mesenteric ischemia.
Footnotes
Author contributions
LJDD: planning and drafting the manuscript; DN: planning and critical revision of the manuscript; ACV, JJK, RHG, HJMV, AM and MJB: critical revision of the manuscript. All authors approved the final draft submitted.
Declaration of conflicting interests
HJMV is a consultant for Medtronic, WL Gore, Endologix and Arsenal AAA. AM has a proctorship for Terumo and Merit Medical. All other authors declared no potential conflicts of interest for the research, authorship, and/or publication of this article.
Ethics approval
Not applicable
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Informed consent
Not applicable