
Abstract
Background
Missed oesophageal cancer (MEC) at upper gastrointestinal endoscopy (UGE) is poorly documented.
Objective
The objectives of this study were: (1) to assess the rate, predictors and survival of MEC; (2) to compare MEC and non-MEC tumours.
Methods
This was a retrospective cohort study conducted at four tertiary centres. Oesophageal cancers (ECs) diagnosed between 2008 and 2015 were included. Patients with a premalignant condition (Barrett, achalasia), prior diagnosis of EC or oesophagogastric junction tumour of gastric origin were excluded. MEC was defined as EC detected within 36 months after negative UGE.
Results
123,395 UGEs were performed during the study period, with 502 ECs being diagnosed (0.4%). A total of 391 ECs were finally included. Overall MEC rate was 6.4% (95% confidence intervals (CI): 4.4–9.3%). The interval between negative and diagnostic UGE was less than 2 years in 84% of the cases. Multivariate analysis showed that a negative endoscopy was associated with proton pump inhibitor (PPI) therapy and less experienced endoscopists. MEC was smaller than non-MEC at diagnosis (25 versus 40 mm, p = 0.021), more often flat or depressed (p = 0.013) and less frequently diagnosed as metastatic disease (p = 0.013). Overall 2-year survival rate was similar for MEC (20%) and non-MEC (24.1%) (p = 0.95).
Conclusions
MEC accounted for 6.4% of all ECs and was associated with poor survival. High-quality UGE and awareness of MEC may help to reduce its incidence.
Key summary
Summarize the established knowledge on this subject
Oesophageal cancer is the eighth most common cancer worldwide. Little is known about oesophageal cancer arising in patients with a recent negative endoscopy. What are the significant and/or new findings of this study?
Missed oesophageal carcinoma is infrequent in patients without known premalignant conditions, but accounted for 6.4% of all oesophageal cancers. Survival of patients with missed oesophageal carcinoma is low and not different from non-missed cancer. Proton pump inhibitor (PPI) therapy and an inexperienced endoscopist are independent predictive factors for missed oesophageal carcinoma. High-quality endoscopy and adhering to guideline-based recommendations may reduce its incidence.
Introduction
Oesophageal cancer (EC) is the eighth most common cancer worldwide and the sixth leading cause of cancer-specific mortality with an estimated incidence rate of 456,000 per year. 1 Despite improvements in diagnostic techniques and therapy in recent years, the 5-year overall survival of EC remains below 20% in western countries. 2 Tumour stage at diagnosis is the main prognostic factor in EC patients, and only those with localized disease hold the opportunity to be treated with curative intention. Unfortunately, early symptoms are usually subtle or non-specific, resulting in an unresectable or metastatic disease stage at the time of diagnosis in more than 50% of cases. 3 Recent studies suggest that early EC treated with either surgery or endoscopic resection achieves excellent 5-year survival rates (75–90%).4,5 Therefore, early detection of small lesions and mucosal abnormalities becomes of extreme importance to improve survival.
In the last decade, several studies have questioned the accuracy of endoscopy for early diagnosis of gastrointestinal neoplasms. Interval colorectal cancer has been extensively studied and its prevalence has been estimated to range from 1.8% to 9%. 6 Studies addressing missed upper gastrointestinal tumours have also found that 4.6% to 25.8% of patients had a negative endoscopy within 3 years before diagnosis. 7 Nevertheless, the number of studies is limited, and most of them have focused on gastric cancer or adenocarcinoma arising from previously diagnosed Barrett's oesophagus (BE).7–12 Missed oesophageal cancer (MEC) is a poorly characterized entity in the non-BE population with only a few retrospective studies in this area, mainly from the UK and with data coming from administrative databases.11,13 Indeed, MEC characteristics, risk factors and prognosis remain to be established.
The aims of this study were to : (1) assess the rate, predictors and survival of MEC; and (2) compare the characteristics of MEC patients with those of non-MEC.
Materials and methods
This was a retrospective cohort, observational and analytical study conducted at four tertiary academic hospitals that provide universal public health care assistance to an area with a population of 1.7 million people. The study protocol adhered to the principles of the Declaration of Helsinki and was approved by the Ethics Committee for clinical research of the Hospital Universitario Ramón y Cajal (3 November 2017). Informed consent for upper gastrointestinal endoscopy (UGE) was obtained in all cases. The Ethics Committee determined that written informed consent was not required in this study due to its retrospective design.
Study population and procedures
All patients who underwent UGE between January 2008 and December 2015 at any of the participating centres were considered for the study, and charts were reviewed. Inclusion criteria for the study were as follows: patients with histology proven EC (adenocarcinoma or squamous cell carcinoma) diagnosed at that period in the participating centres. Exclusion criteria were: (1) prior diagnosis of EC, BE or achalasia; (2) gastroesophageal junction (GEJ) adenocarcinomas of gastric origin; (3) patients with no follow-up at the participating centres; (4) patients referred for treatment from other hospitals with no UGE at any of the participating centres; and (5) more than 10% of the variables with missing values (Figure 1).
Study flowchart. MEC: missed oesophageal cancer.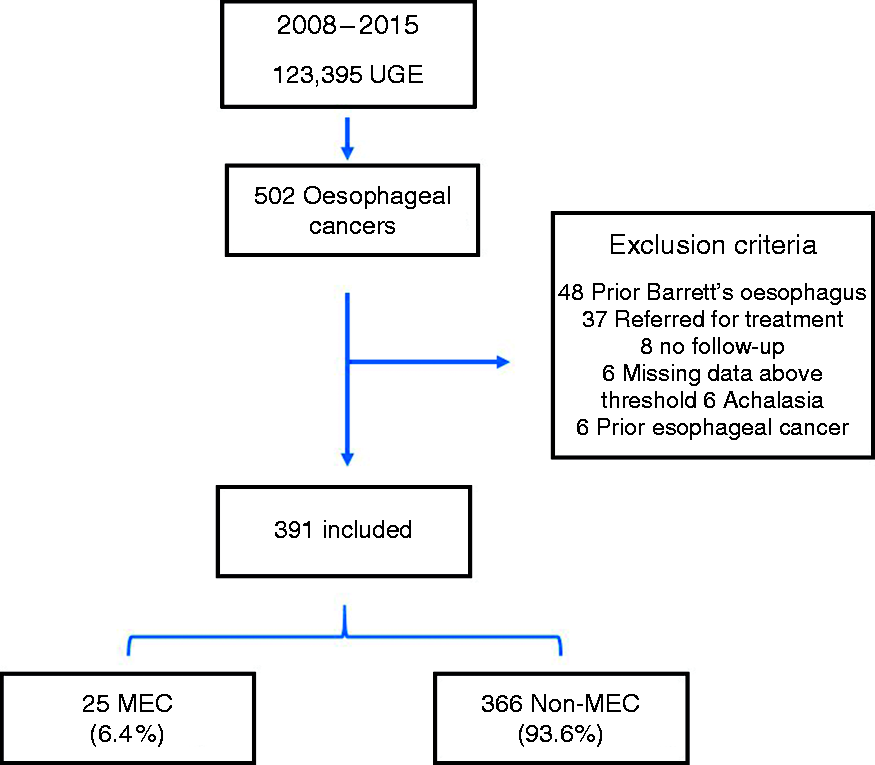
Paper (hospital) and electronic (hospital and primary health care) databases of all EC subjects were independently reviewed by two gastroenterologists at each institution. This search included previous negative UGE performed in other public or private hospitals in the same regions. The following demographic and clinical variables were collected: age, sex, tobacco and alcohol consumption as binary categories, EC family history, previous diagnosis of head and neck or lung cancer, obesity (defined as >30 kg/m2 body mass index (BMI)), American Society of Anesthesiologists physical status classification (ASA), history of food impaction, UGE indication (dysphagia, haematemesis, melaena and constitutional syndrome were considered alarm symptoms) and medication at both initial negative and final diagnostic endoscopy of MEC.
Gastroscopes used for examination were GIF-Q165, GIF-H180, GIF-H190 (Olympus® Optical, Tokyo, Japan), EG-290KP, EG-294 KP, EG-27I10, EG-29I10, EG-1690K, EG-3490K, EG-2790K (Pentax®, Tokyo, Japan) and EG-530FP, EG-250PES (Fujifilm®, Japan). All procedures were performed or directly supervised by a staff gastroenterologist with expertise in UGE using white light.
Date, sedation (endoscopist propofol-based/endoscopist non-propofol based/anesthesiologist), UGE duration (retrieved as global recording time, i.e. time during which endoscopy software is ready for image or video acquisition), urgent or elective setting, inpatient or outpatient, use of conventional and digital chromoendoscopy (Narrow Band Imaging (NBI), i-scan or Fujinon Intelligent Chromo Endoscopy (FICE) as ascertained by written reports and videos and imaging review), and primary diagnosis were collected from both negative and diagnostic endoscopy records. Size of the lesion, as assessed by the endoscopist (millimetres), presence of ulceration, location (proximal, medial, distal third of oesophagus and GEJ) and tumour morphology (depressed, flat, sessile or mass-like) were obtained from the endoscopy report. We used Siewert–Stein classification for GEJ tumours. Main operators were classified as highly experienced (>5 years as a staff gastroenterologist and >1000 UGEs) or less experienced endoscopist (<5 years and <1000 UGEs).
Histologic subtype (squamous cell carcinoma or adenocarcinoma) and grade of differentiation (undifferentiated–poorly differentiated or moderately well differentiated) were also retrieved from pathology reports.
Tumour stage was determined as per the American Joint Committee on Cancer cTNM system 7th edition. 14 Oncologic treatment was recorded as binary outcomes (Yes/No): neoadjuvant therapy, curative-intent surgery, adjuvant therapy and palliative chemotherapy. Survival status was established using the date of EC diagnosis and the time of death or the date of the last medical visit (in-hospital or primary healthcare) on which the patient was alive.
Study endpoints
The primary outcomes were to assess the proportion and characteristics of MEC. Secondary outcomes were to evaluate the differences between MEC and Non-MEC and between negative UGE and diagnostic UGE in non-MEC. In line with previous research in this field, MEC was defined as EC detected within 36 months after negative UGE.7,11,13
The presumed reasons for MEC were categorized as: ‘Missed lesion’ (lesion not seen by the endoscopist), ‘Sampling error’ (when a lesion was detected but biopsy sampling was inadequate) and ‘Inappropriate follow-up’ (when a high-risk lesion was present but no proper monitoring was performed).
Statistical analysis
Mean, standard deviation, median and range were calculated for continuous variables and frequency counts and percentages for categorical data. Ninety-five confidence intervals (CI) for proportions were calculated based on the Wilson method. Data were analyzed using parametric methods for normally distributed continuous data (t-test) and non-parametric methods (Mann–Whitney U test) for non-normally distributed continuous data. Chi-squared and Fisher's exact tests were used for categorical data. To decrease the risk of type I error, only those variables previously reported as risk factors for upper gastrointestinal missed cancer or with plausible physiopathological relation with MEC were included in the univariate analysis. All variables included had a rate of missing values less than 5%. Multivariate analysis was performed by using backward stepwise binomial unconditional logistic regression to: (1) detect predictors associated with negative UGE when compared to diagnostic UGE in non-MEC; and (2) identify factors associated with MEC at diagnosis. When more than one negative UGE was available, the most recent UGE was considered for the analysis.
Variables with p values < 0.05 in univariate analysis were included in logistic regression models. The area under the Receiver Operating Characteristic curve was calculated with non-parametric analysis to evaluate the discriminative ability of the logistic models. Goodness-of-fit was assessed using the Hosmer–Lemeshow´ test and pseudo-R2 Cragg–Uhler (Nagelkerke).
One-year and 2-year survival probabilities were calculated for MEC and non-MEC using the Kaplan–Meier method and compared with the log-rank test. All analyses were two-tailed, and p values less than 0.05 were considered significant. Analyses were performed at the promoting institution (Hospital Universitario Ramón y Cajal, Madrid) using STATA software version 14.1 (StataCorp. Texas, USA).
Results
Characteristics and reasons for MEC of the 25 cases of oesophageal carcinoma with previous negative endoscopy.
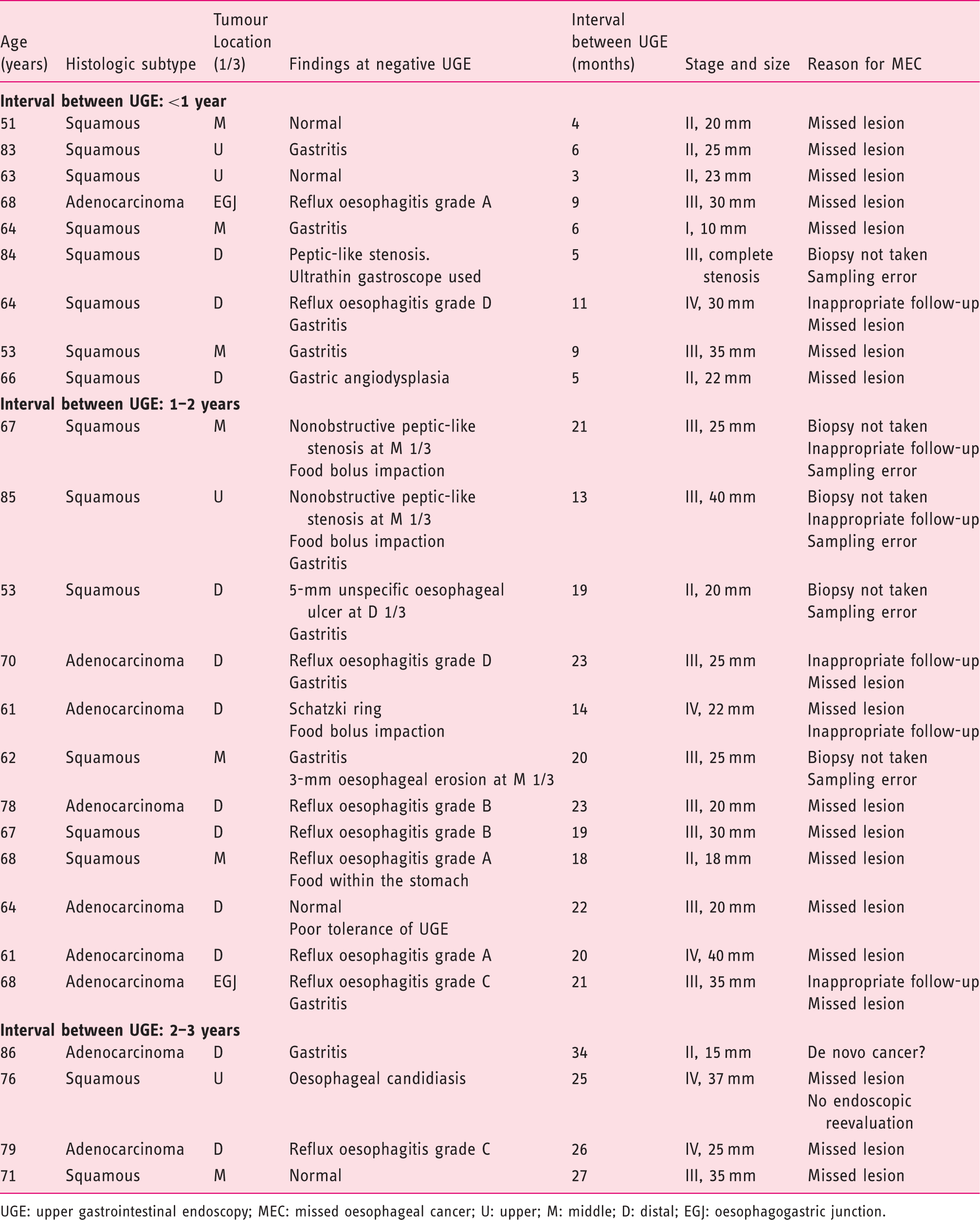
UGE: upper gastrointestinal endoscopy; MEC: missed oesophageal cancer; U: upper; M: middle; D: distal; EGJ: oesophagogastric junction.
Comparative analysis: Initial negative endoscopy in MEC patients versus diagnostic endoscopy in non-MEC patients.
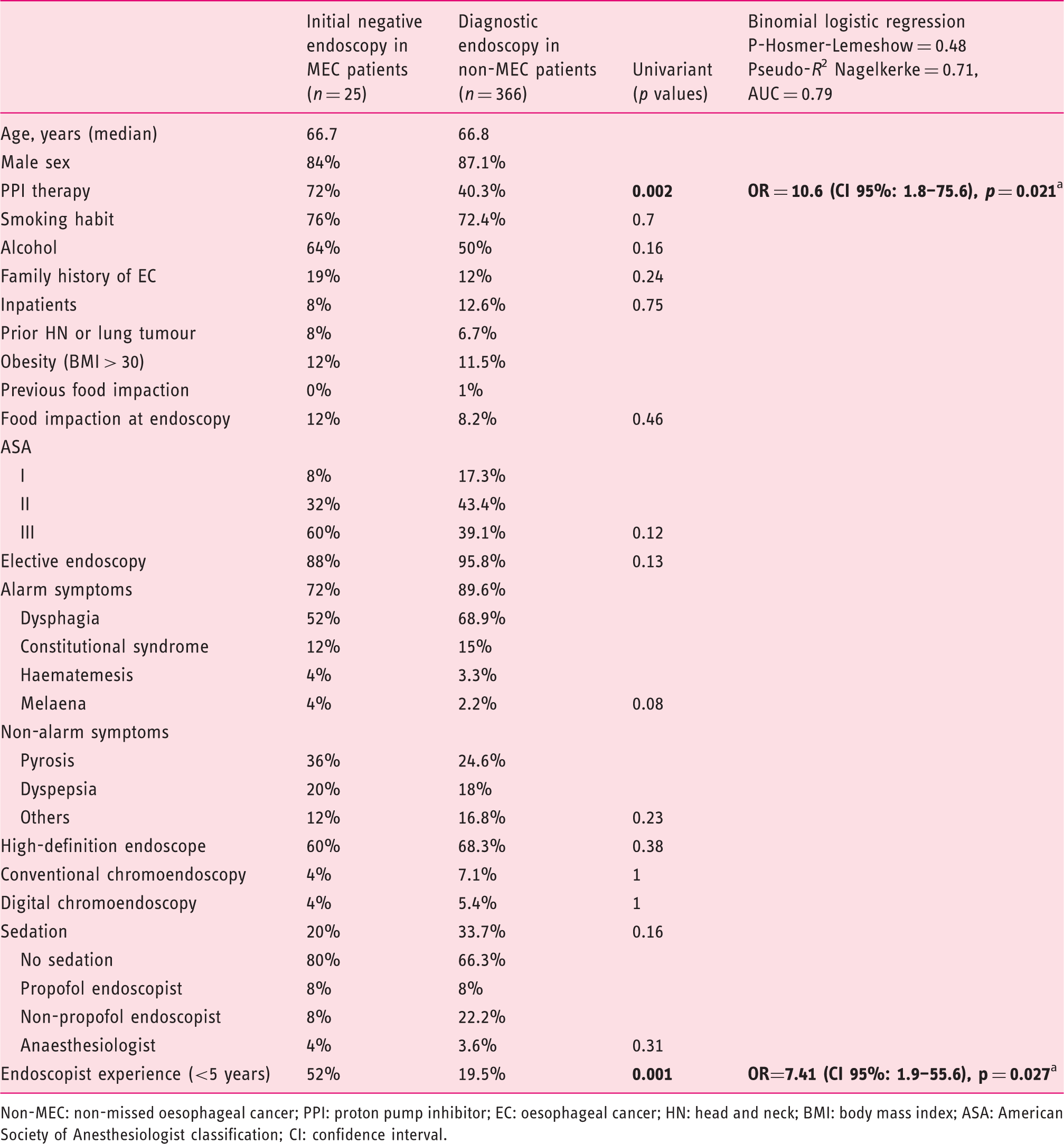
Non-MEC: non-missed oesophageal cancer; PPI: proton pump inhibitor; EC: oesophageal cancer; HN: head and neck; BMI: body mass index; ASA: American Society of Anesthesiologist classification; CI: confidence interval.
Comparative analysis: MEC versus non-MEC at diagnosis.
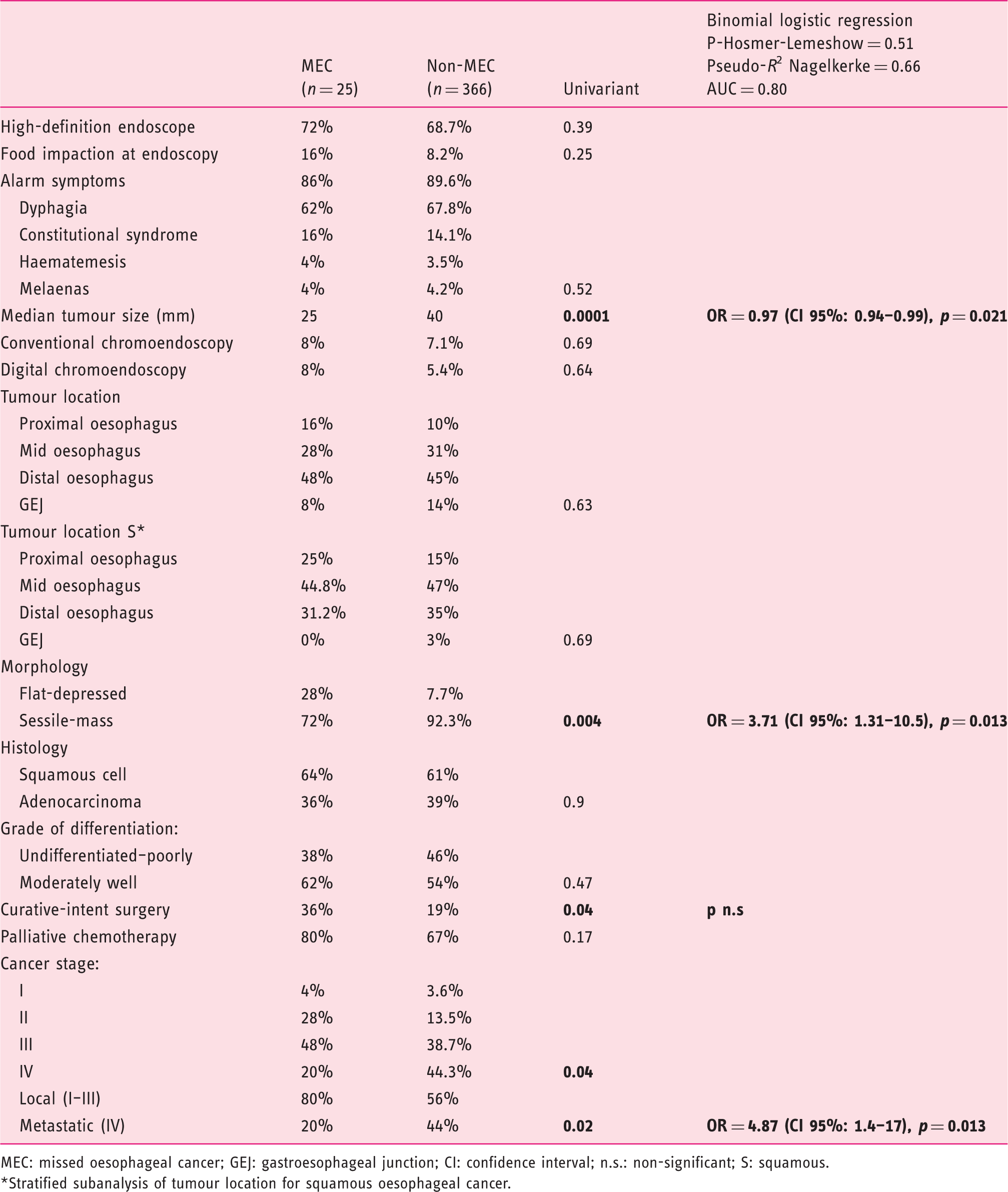
MEC: missed oesophageal cancer; GEJ: gastroesophageal junction; CI: confidence interval; n.s.: non-significant; S: squamous.
*Stratified subanalysis of tumour location for squamous oesophageal cancer.
Survival analysis did not show any significant differences between both groups and it is summarized in Figure 2.
Survival analysis. MEC: missed oesophageal cancer. 95% Confidence intervals given in parentheses.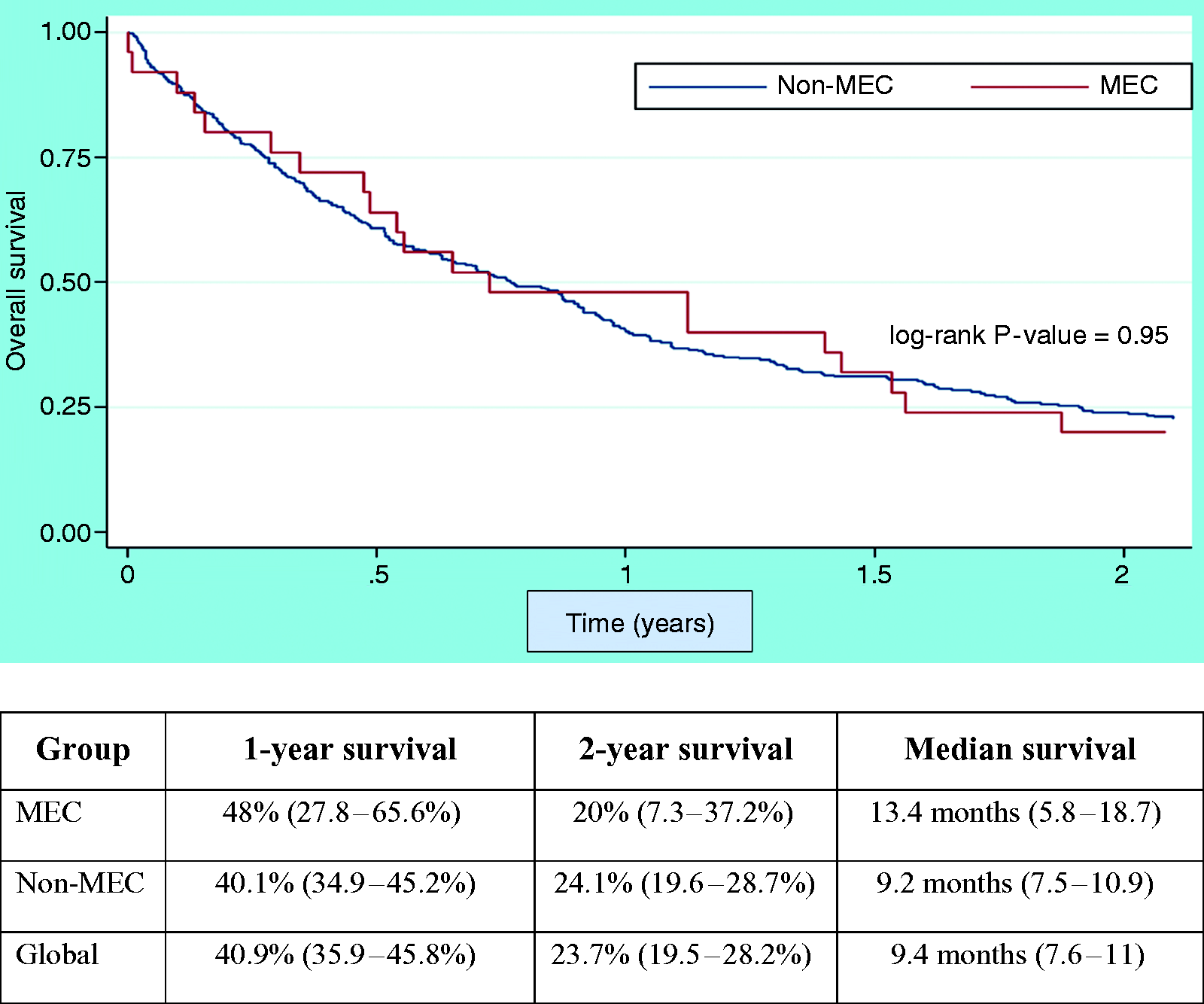
Discussion
Results from this multicentric cohort study support that MEC is relatively frequent at routine UGE in tertiary referral centres, with an overall MEC rate as high as 6.4% (CI 95%: 4.4–9.3%) among newly diagnosed EC. Unfortunately, a head-to-head rate comparison with previous reports may not be possible for several reasons (Supplementary Table 1):
Our study has found that an inexperienced endoscopist and PPI treatment were independently associated with MEC. This last association had been detected in previous investigations and may be explained by the partial mucosal healing of small mucosal lesions in the distal third of the oesophagus by PPI therapy.25,26 Female gender, younger age, non-gastroenterologist endoscopist and increasing comorbidity have also been postulated to increase the likelihood of interval upper gastrointestinal cancer.9,10,12 Noticeably, neither our study (20% MEC versus 33% non-MEC, p = 0.16) nor other investigations have proven that sedation is related to MEC, but some data indicate that moderate sedation increases UGE examination quality and patient satisfaction. 27 The low proportion of patients undergoing sedation for UGE in our study does not represent our current standard practice, where propofol-based sedation has been adopted in recent years. Whether these negative results may be attributable to inadequate statistical power remains unclear, but it may indeed be a possibility. From our perspective, adequate sedation is essential for high-quality UGE, as it may enhance the detection of small lesions and possibly decrease the MEC rate.
Other physician-related factors that have been proposed to explain missed cancers in UGE are not to biopsy benign-like lesions, the presence of oesophagitis, obtaining an insufficient number of biopsies, pathological errors or follow-up delay.12,13 This reinforces the idea that every stricture, ulcer or non-specific oesophageal mucosal abnormality should be biopsied and closely monitored.11,28 When oesophagitis is severe or atypical in appearance, further endoscopic evaluation should be mandatory in the 6–8 weeks after PPI treatment.29,30 Remarkably, inappropriate follow-up or sampling error was documented in 36% of the patients that eventually developed MEC.
It is worth mentioning that the median duration of negative UGE was only 5.9 minutes, which may have contributed to MEC. Teh et al. found that examination times longer than 7 minutes were more likely to detect early gastric cancer and dysplasia;31 indeed, recent quality standard guidelines in UGE support this minimum duration. 28
In our study, only one MEC was diagnosed as a stage I disease, 84% of the cases were diagnosed within 2 years from negative endoscopy and alarm symptoms were common in patients at negative UGE. Besides, MECs were more often encountered as flat or depressed (which could have contributed to missing a lesion), follow-up or biopsy policy were often inappropriate and no differences were found in grade of differentiation.9–13 Altogether leads us to hypothesize that most MECs were actually ‘true MECs’ secondary to an unrecognized lesion rather than new fast-growing ECs.
The proximal oesophagus was previously reported to be associated with MEC8,11 in probable relation with a less careful evaluation of this segment. On the other hand, we found that more than half of MECs were located at the distal third of the oesophagus or the GEJ junction without significant differences with non-MEC. As all adenocarcinomas were in the distal third/GEJ, we performed a stratified analysis to explore the relationship between squamous subtype and location, without significant findings either (Table 3).
Another relevant finding of our study was that despite MECs being smaller and less often diagnosed at stage IV, 1-year and 2-year survival rates remained discouraging. This fact highlights the importance of early diagnosis and the consequences of missing a malignant lesion.
Our study has some limitations that should be acknowledged.
Fourteen patients (2.7%) were excluded from the analysis due to missing data or no follow-up. Nonetheless, missing data are a rule rather than an exception in biomedical research and it remained within acceptable standards in our analysis.32,33
We used the time during which endoscopy software was ready for image acquisition as a surrogate marker of mouth to withdrawal time, since this data was not available. Hence, the median real exploration time for negative UGE was less than 5.9 minutes.
Our MEC rate might be slightly underestimated. The lack of a nationwide cancer registry database in our country prevented us from ascertaining whether patients with a negative UGE at our institution have been subsequently diagnosed with EC at other hospitals. Nonetheless, we consider that the relevance of this fact in our estimations is expected to be low, since healthcare is public and universal in Spain, and patients with EC are ordinarily referred to our centres for treatment.
Finally, the study may be underpowered for the detection of a small difference in survival due to limited sample size.
Among other strengths of our study are that it identifies new predictors of MEC, it provides useful information for clinical practice and represents a recent non-administrative database-based cohort that may contribute to focus the attention on a relevant but often forgotten issue. This problem could be underrated considering that MEC is uncommon at UGE (25 cases out of 123,395 UGEs during a 7-year study period). However, this fact is related to a low incidence of EC in our area and current data indicate that UGE missed cancer rate is above that of colorectal interval cancer. 6 Consequently, research in this field is pertinent and needed.
Future research should focus on what specific measures in UGE may change the current panorama of delay diagnosis. Digital and conventional chromoendoscopy are known to be useful in high-risk groups; nonetheless, they are time-consuming and its application in every single UGE may be unrealistic and likely inefficient. The low use of chromoendoscopy in our study is explained by the small proportion of early neoplasms, the lack of digital chromoendoscopy in some endoscopes and the limited adoption of this technique in our units until recently. Until more data are available, thorough and slow mucosal interrogation of the whole oesophagus, biopsies of any suspicious lesion and bearing in mind that PPI may mask small irregularities are simple and readily available strategies to earlier detection.
In conclusion, MEC represented 6.4% of all ECs. MEC probably arose from unrecognized or misdiagnosed lesions at negative UGE and was associated with physician-related factors. Raising awareness of MEC among endoscopists, adhering to clinical practice guidelines and improvements in UGE quality may help to reduce its incidence and improve prognosis. Further prospective and randomized studies are awaited to identify the most effective strategies to decrease the rate of upper gastrointestinal missed cancer.
Supplemental Material
Supplemental material for Rate of missed oesophageal cancer at routine endoscopy and survival outcomes: A multicentric cohort study
Supplemental material for Rate of missed oesophageal cancer at routine endoscopy and survival outcomes: A multicentric cohort study by Enrique Rodríguez de Santiago, Nerea Hernanz, Héctor Miguel Marcos-Prieto, Miguel Ángel De-Jorge-Turrión, Eva Barreiro-Alonso, Carlos Rodríguez-Escaja, Andrea Jiménez-Jurado, María Sierra-Morales, Isabel Pérez-Valle, Nadja Machado-Volpato, María García-Prada, Laura Núñez-Gómez, Andrés Castaño-García, Ana García García de Paredes, Beatriz Peñas, Enrique Vázquez-Sequeiros and Agustín Albillos in United European Gastroenterology Journal
Footnotes
Acknowledgement
All authors fully approved the final version of the manuscript.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Ethics approval
The study was approved by the Ethics Committee for clinical research of the Hospital Universitario Ramœ Cajal (3 November 2017, code: HRYC: 213-17).
Financial support
This study did not receive any grant or financial support.
Informed consent
Informed consent for upper gastrointestinal endoscopy was obtained in all cases. The Ethics Committee determined that written informed consent was not required in this study due to its retrospective design.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.