
Abstract
Background
The prevalence and frequency of oesophageal symptoms suggestive of a functional oesophageal disorder according to the Rome IV criteria are unknown.
Objective
We aimed to describe the prevalence and risk factors for oesophageal symptoms compatible with functional oesophageal disorders in the general population.
Methods
Data were analysed from a population-based online survey of 6300 individuals aged ≥ 18 years in the USA, UK and Canada with equal demographic proportions across countries. Questions included the Rome IV diagnostic questionnaire, demographics, medication, somatization, quality of life, and organic gastrointestinal (GI) disease. Multivariate analysis was used to identify factors independently related to oesophageal symptoms.
Results
Data from 5177 participants (47.8% female; mean age 46.7 years) were available for analysis. Symptom prevalence was 8.1% for globus, 6.5% for heartburn, 4.5% for dysphagia and 5.2% for chest pain, and 17.0% reported at least one oesophageal symptom. Oesophageal symptoms were independently associated with younger age, female gender, previous abdominal surgery and the presence of other functional GI disorders. Reporting oesophageal symptoms was associated with reduced quality of life.
Conclusion
Oesophageal symptoms are common in the general population and important predictors include other functional GI disorders, age and gender. Oesophageal symptoms are associated with poorer quality of life.
Keywords
Key summary
Current knowledge:
Oesophageal symptoms result in high healthcare utilization and reduced quality of life. Functional oesophageal disorders are a common cause of symptoms but the prevalence in the general population is largely unknown. No studies describing the overall frequency of oesophageal symptoms compatible with the Rome IV criteria in the general population are available.
Key findings of this study:
We provide the first report of the population prevalence of the four symptoms used to define Rome IV functional oesophageal disorders. Important predictors of these symptoms are the presence of non-oesophageal functional gastrointestinal disorders, younger age, previous abdominal surgery and female gender.
Introduction
Oesophageal symptoms account for a significant proportion of healthcare utilization, have a significant impact on social and leisure activities, and result in reduced quality of life (QoL).1,2 Furthermore, there is an economic impact, both for the affected individual and society in general, since work capacity may be reduced in those affected by these symptoms.3,4 Many of these individuals suffer from gastroesophageal reflux disease (GERD), but a large proportion have an oesophageal disorder that is part of the spectrum of functional gastrointestinal (GI) disorders (FGIDs) currently defined by the Rome IV criteria. 5 These oesophageal disorders are characterized by chronic or frequently recurring symptoms of presumed oesophageal origin in the absence of identifiable structural, inflammatory, motor or metabolic mechanism causes. The prevalence of functional oesophageal disorders in the general population is largely unknown, even though several studies have described the prevalence of non-cardiac chest pain, 6 GERD 7 and oesophageal symptoms using different methodologies.8,9 Studies that evaluate the overall frequency of oesophageal symptoms compatible with functional oesophageal disorders defined by the Rome IV criteria 10 in the general population and how they manifest clinically are lacking.
We aimed to describe the prevalence of oesophageal symptoms in the general population in three culturally similar English-speaking countries and to identify risk factors for symptoms compatible with functional oesophageal disorders as defined by Rome IV criteria. 10 We also aimed to assess the association of oesophageal symptoms with measures of QoL and healthcare utilization.
Methods
Online survey
The study utilized data from an online survey of 6300 individuals aged ≥ 18 years in the USA, UK and Canada (2100 in each country). Subjects were recruited by a global market survey company (Qualtrics Inc., Provo, Utah) and asked to respond to a ‘health survey’ with no specific mention of GI symptoms. Written informed consent was obtained from subjects prior to participation in the study and they were asked to answer questions including the Rome IV diagnostic questionnaire for adults, demographic data (age, gender, ethnicity and living conditions), medical history (GI diseases, history of abdominal surgery, medications and healthcare utilization), QoL, non-GI symptoms (somatization) and psychosocial factors.
By use of quota-based sampling, equal proportions of sex (50/50%), age group (40% age 18–39, 40% age 40–64 and 20% age 65+) and education distributions (maximum 30% of the study population with a college degree or equivalent) across countries was ensured. Inconsistent responders (identified by repeated symptom questions) and responders who answered in a random manner were eliminated from the data set in a rigorous process, as were individuals who completed the survey unreasonably quickly. Details have been reported elsewhere11–14 (comparability in the supplement12). Before data collection started, the study was reviewed by the ethical committee in North Carolina, USA, and was approved but was deemed not to formally require an ethical approval as the subjects were completely anonymous. The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki.
Oesophageal symptoms and Rome IV diagnosis
The prevalence and frequency of oesophageal symptoms in the past 3 months, and their consistency with a diagnosis of a functional oesophageal disorder, were assessed based on responses to the Rome IV diagnostic questionnaire. 14 The Rome IV functional oesophageal disorders are: functional chest pain, functional heartburn, reflux hypersensitivity, globus and functional dysphagia. 10 As combinations of endoscopy, pH monitoring and oesophageal manometry are required for the clinical diagnosis of oesophageal disorders, we were able to describe oesophageal symptoms compatible with functional oesophageal disorders only. 10 We used the minimum diagnostic frequency cut-off for each of the oesophageal symptoms, used to define the functional oesophageal disorders according to Rome IV, to classify symptoms as present (at least weekly for dysphagia, chest pain and globus, and twice weekly for heartburn) or not. 10 However, we also described the frequency of survey responders with symptom constellations compatible with a functional oesophageal disorder according to the Rome IV definition.
Somatization and QoL
QoL during the month prior to the survey was assessed by the Short Form (SF)-8 questionnaire. 15 The SF-8 is similar to the SF-36v2 16 but is condensed to eight items, one for each domain. A physical component summary (PCS) score and a mental component summary (MCS) score can be calculated from the SF-8 results. The PCS score ranges from 10–67 (10 is very poor and 67 excellent QoL). The MCS score ranges from 8–70 (8 is very poor and 70 excellent QoL). 15
Somatization, or non-GI symptom severity, was assessed with the Patient Health Questionnaire (PHQ)-12, 17 which is a shortened version of the PHQ-15, 18 but with the three questions on GI symptoms excluded. The questionnaire assesses how bothersome 12 non-GI somatic symptoms were in the past month, each rated on a three-point scale (0 = ‘not bothered at all’, 1 = ‘bothered a little’ and 2 = ‘bothered a lot’). The maximum score is 24 points.
Statistics
The Mann–Whitney U test or Students t-test was used for group comparisons for continuous variables. χ2 analyses were used for dichotomous variables. In order to identify variables that were independently associated with specific oesophageal symptoms, we calculated Spearman correlation coefficients between the specific oesophageal symptoms and other variables in the survey. Variables with a significance level of p ≤ 0.1 in the univariate analyses were then entered into a multivariate analysis (logistic regression) and variables with a p-value of < 0.05 in that analysis were considered significant. We either excluded variables with significant overlap or merged them into a single variable (such as presence of an FGID instead of several different subgroups of FGIDs). We also excluded variables in the multivariate analysis not considered to be risk factors for developing an oesophageal symptom, but were more likely to reflect the effect of having one, such as being treated with a proton pump inhibitor or visiting a doctor.
The number of different regions of the GI tract where the patient had FGIDs according to the anatomical groupings of diagnoses in the ROME IV criteria, excluding the oesophagus (maximum three: anorectal, gastroduodenal and bowel disorder), was used for further analyzes.
Individuals who had previously been diagnosed by a doctor with GERD or acid reflux were excluded from the primary study sample. However, we also re-ran our analyses with these individuals included.
We also tested the hypothesis that an increasing frequency of any oesophageal symptom would be associated with worsening QoL and more severe non-GI somatic symptoms (PHQ-12), by using analysis of variance with linear contrast analysis to look for a linear trend, with effect sizes demonstrated as partial eta squared (η2); small effect size 0.01, medium effect size 0.06 and large effect size 0.14). 19 Statistical analyses were conducted using the IBM SPSS Statistics software, version 21 for Windows.
Results
Population
We included data from 5177 participants in the primary analysis (Figure 1), after excluding 369 inconsistent responders (6%) and 754 who reported a previous GERD diagnosis (12%). The mean age was 46.7 (range 18–92) years and 47.8% were female.
Flow chart of study selection.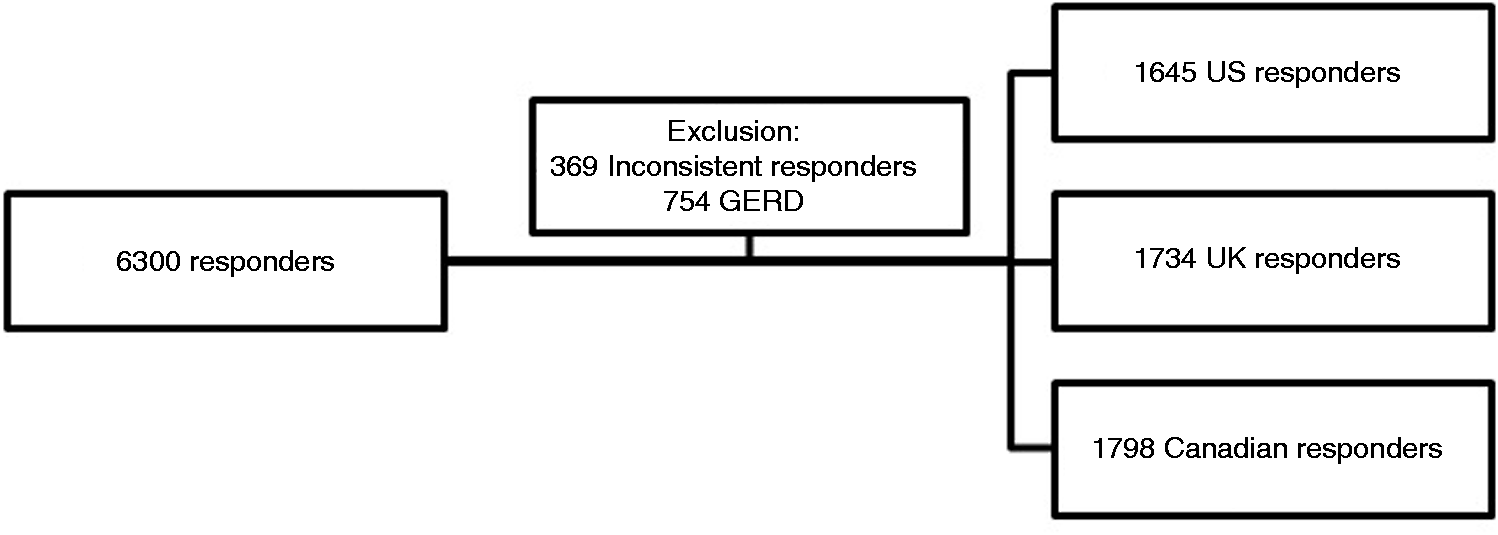
Prevalence of symptoms
Globus was the most prevalent oesophageal symptom with 8.1% (n = 420), followed by heartburn 6.5% (n = 334), chest pain 5.2% (n = 269) and dysphagia 4.5% (n = 233) (Figure 2). In all, 17.0% (n = 881) had at least one oesophageal symptom. Of these, 621 (12.0%) had only one symptom, 170 (3.3%) two, 65 (1.3%) three and 25 (0.5%) had all four symptoms.
Prevalence of oesophageal symptoms.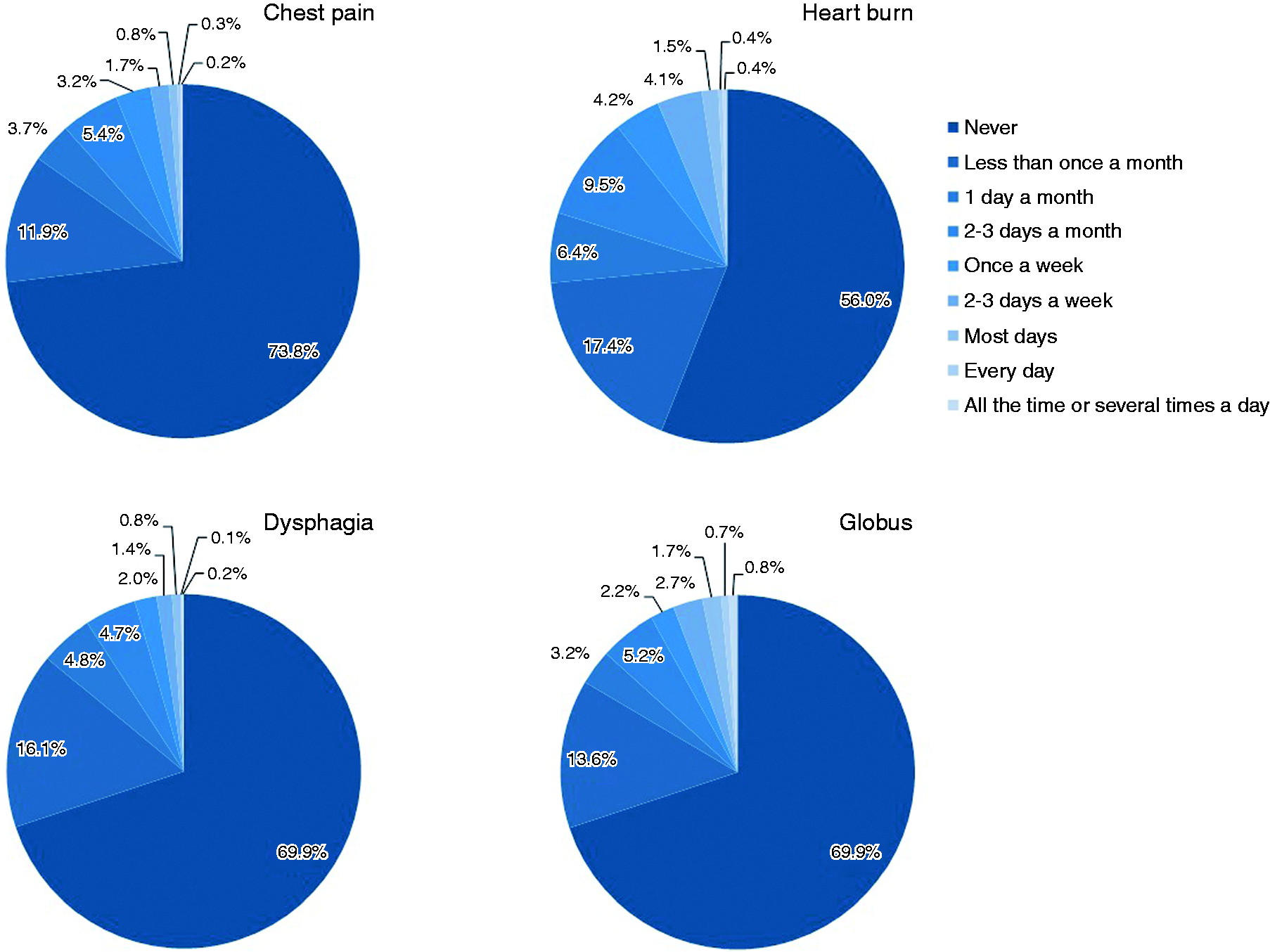
The prevalence of globus (USA 8.0%, Canada 8.9% and UK 7.4%; p = 0.24) and chest pain (USA 3.6%, Canada 2.6% and UK 2.7%; p = 0.16) did not differ among the three countries. However, heartburn (USA 8.9%, Canada 6.0% and UK 4.6%; p < 0.001) and dysphagia (USA 6.0%, Canada 3.5% and UK 4.1%; p = 0.001) showed a different distribution between the countries with the highest prevalence rate in the USA. The prevalence of symptoms that clustered in constellations with a symptom duration consistent with oesophageal disorders as defined by the Rome IV criteria 10 was 1% for globus, 3.2% for functional dysphagia, 0.7% for reflux hypersensitivity, 0.8% for functional chest pain and 1.1% for functional heartburn.
Factors associated with oesophageal symptoms
Factors independently associated with presence of oesophageal symptoms.
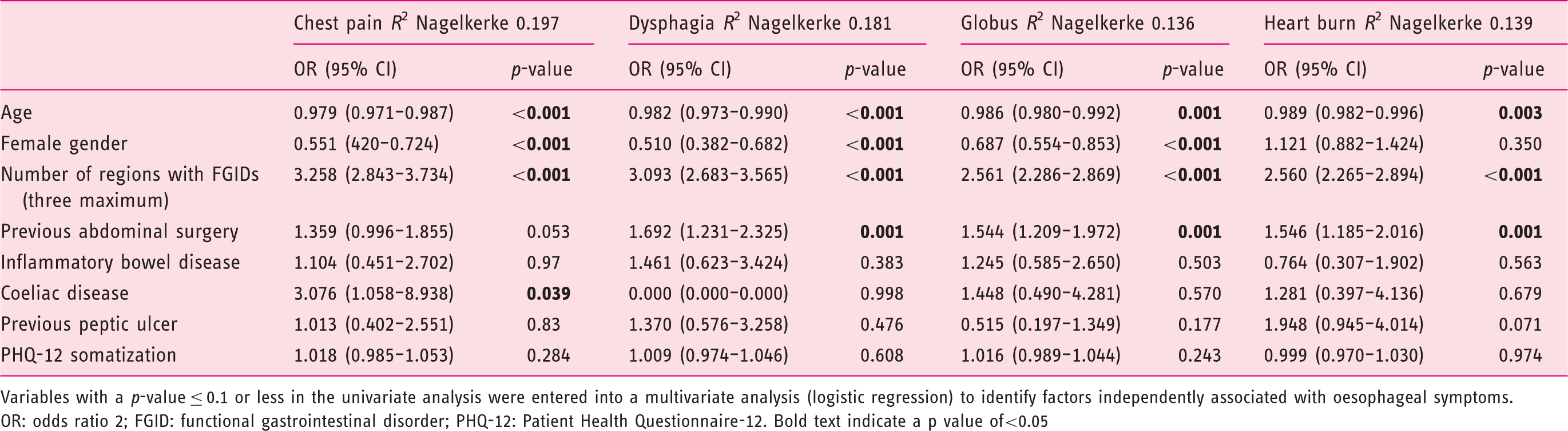
Variables with a p-value ≤ 0.1 or less in the univariate analysis were entered into a multivariate analysis (logistic regression) to identify factors independently associated with oesophageal symptoms.
OR: odds ratio 2; FGID: functional gastrointestinal disorder; PHQ-12: Patient Health Questionnaire-12. Bold text indicate a p value of<0.05
With increasing numbers of regions with an FGID, a gradual increased in the proportion of subjects reporting oesophageal symptoms could be detected (p < 0.001 for all symptoms, Figure 3).
Relationship between the number of regions with functional gastrointestinal disorders (oesophageal disorders excluded) in patients and the corresponding percentage of subjects reporting an oesophageal symptom, p < 0.001 for all.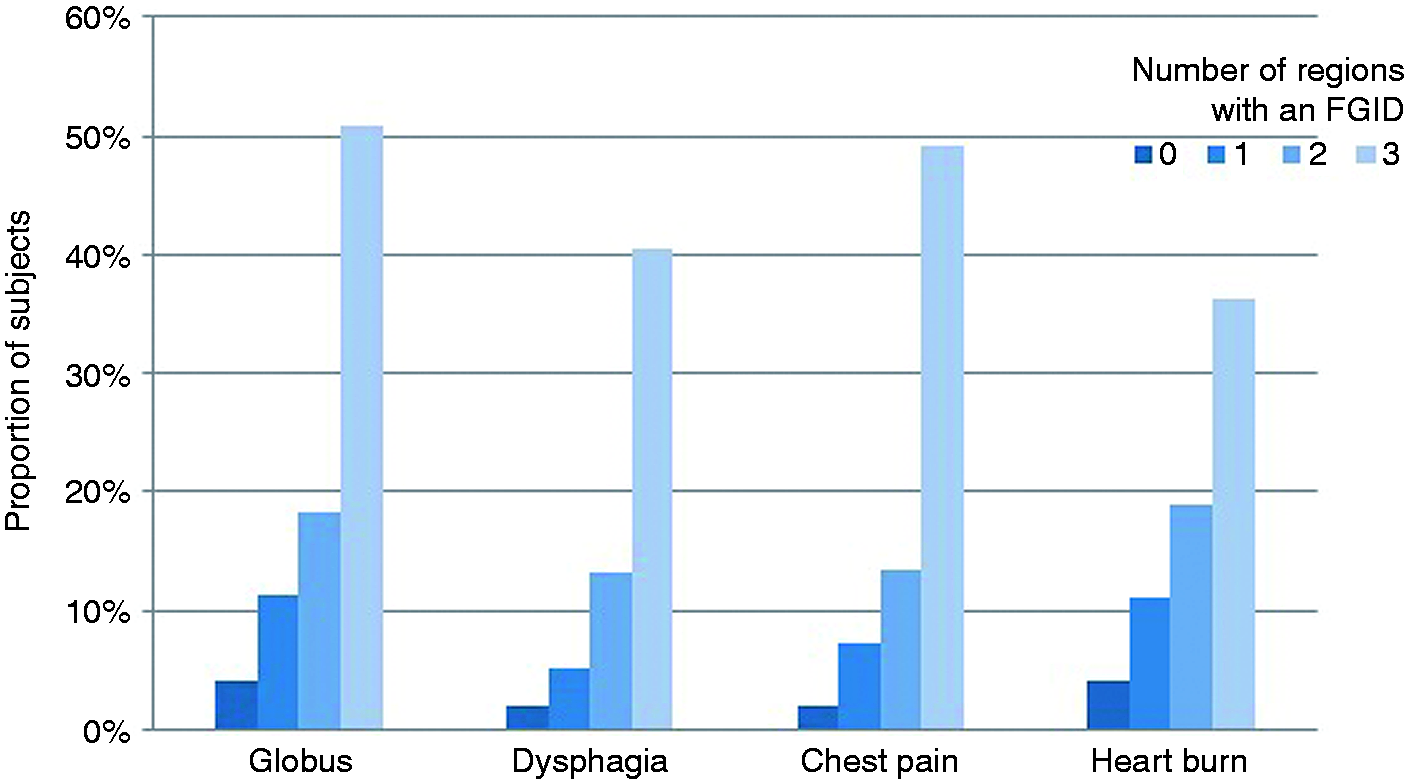
Comparison of overall characteristics between subjects with oesophageal symptoms and subjects without oesophageal symptoms.
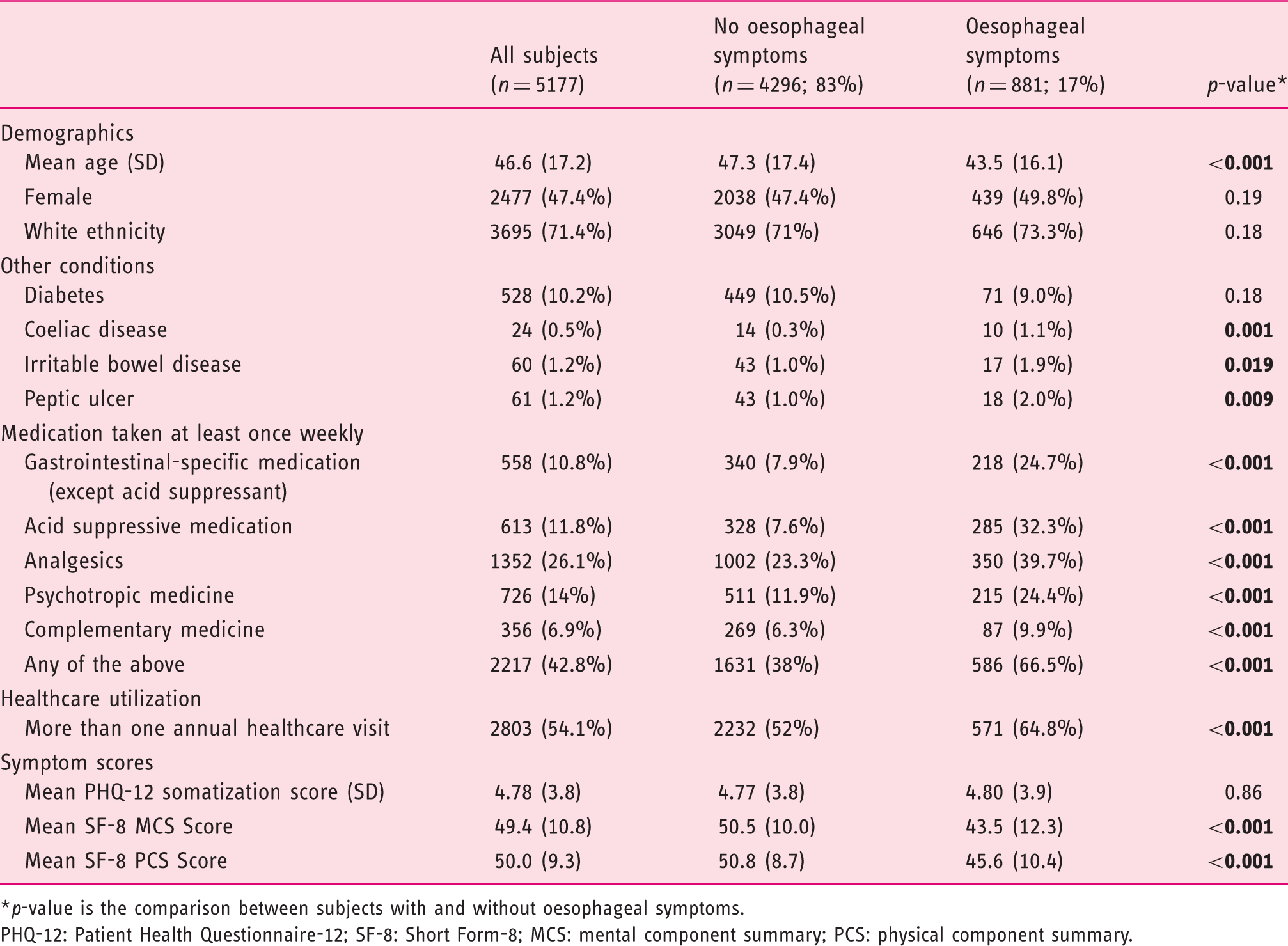
p-value is the comparison between subjects with and without oesophageal symptoms.
PHQ-12: Patient Health Questionnaire-12; SF-8: Short Form-8; MCS: mental component summary; PCS: physical component summary.
Oesophageal symptoms, QoL, healthcare utilization and non-GI symptoms
Partial η2 in symptom frequency, quality of life and Patient Health Questionnaire-12.
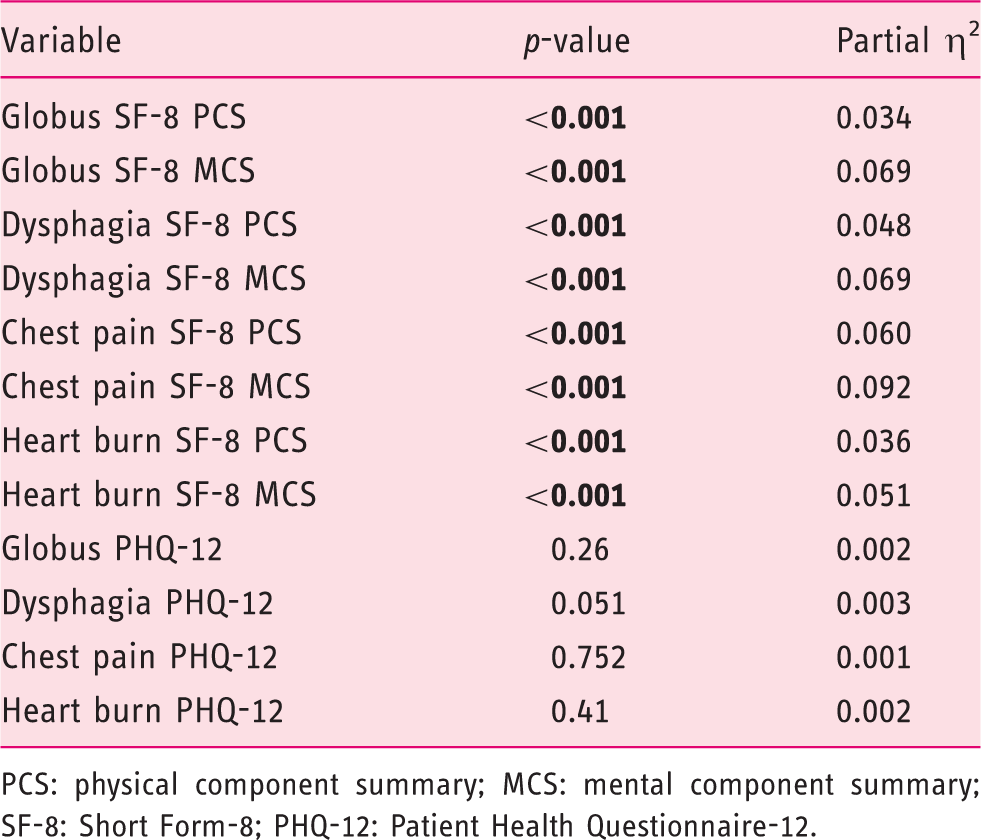
PCS: physical component summary; MCS: mental component summary; SF-8: Short Form-8; PHQ-12: Patient Health Questionnaire-12.
In our subject sample, 965 (18.6%) of all responders had seen a doctor because of concerns with their GI health problems. This percentage was significantly higher for individuals with any of the oesophageal symptoms compared with subjects without oesophageal symptoms: 33 vs 17% for those with globus, 31 vs 18% for heartburn, 39.5 vs 18% for dysphagia and 37 vs 18% for those with chest pain (p < 0.001 for all).
The median PHQ-12 score in our cohort was 4 (range 0–24). In contrast to QoL scores, there were no significant linear trend effects between the frequency of any of the oesophageal symptoms and PHQ-12 scores (Table 3).
Discussion
In this study, we present data on oesophageal symptoms in a large representative sample of the general population of adults in three English-speaking countries with comparable age, gender and educational distributions. Symptom prevalence ranged between 4.5–8.1% depending on the symptom, and a prevalence of symptom constellations compatible with a diagnosis of a functional oesophageal disorder ranged from 0.8–3.2% depending on the disorder. The most important factors associated with oesophageal symptoms were younger age, female gender and overlap with other FGIDs. Importantly, having oesophageal symptoms was clearly associated with reduced physical and mental QoL, and increased healthcare utilization.
In this study, the strongest risk factor for reporting oesophageal symptoms was overlap with GI symptoms compatible with other FGIDs, which is consistent with prior research that showed that oesophageal symptoms suggestive of GERD are excessively common in patients with irritable bowel syndrome (IBS). 8 Although the frequency varies widely between studies, about a fourfold increase is seen overall. The wide variability in frequency estimates is most likely due to differences in diagnostic criteria of GERD and the different minimum frequency of symptoms required for the diagnosis of GERD-like symptoms. 20 Dyspepsia 21 and globus 20 have also been shown to overlap with GERD symptoms, while globus has been shown to overlap with IBS. However, these studies had small sample sizes and were likely to have problems with selection bias. However, there are some more recent studies that have shown that FGIDs commonly overlap.22–24 The cause for this overlap between oesophageal symptoms and FGIDs in other GI tract regions is not known, but a generalized visceral hypersensitivity in the GI tract,25,26 disturbed brain–gut interactions, 27 and comorbid psychological disturbances and somatization12,28 may explain this overlap.
Some other associations and also lack of associations seen in this study were noteworthy. Previous abdominal surgery was found to be associated with symptoms compatible with a functional oesophageal disorder, which is in line with previous studies that have reported that abdominal surgery can contribute to symptoms in FGIDs, in particular for bowel disorders.29,30 Somatization has also been found to be associated with increased severity of GI symptoms, including oesophageal symptoms, in previous studies.31,32 However, this could not be confirmed in the present study. The reason for this is unclear. Dysphagia and heartburn were significantly more common in the USA than in the UK and Canada, and patients from USA also reported more oesophageal symptoms overall. A possible explanation could be the significantly higher prevalence of obesity in the USA compared to the UK and Canada. 33 However, we did not have access to body mass index data on the study participants and this could not be correlated with symptoms. In our study, we found that suffering from oesophageal symptoms is associated with reduced QoL, increased healthcare consumption and some non-GI conditions such as previous abdominal surgery, peptic ulcer disease and coeliac disease. This is, to some extent, also consistent with other previous studies.1,2,6,22
Our study has several strengths. We included patients from three native English-speaking countries with similar demographics, to minimize language and demographic effects. To date, validated translations of the Rome IV questionnaire have not been available for global use. We used the entire Rome IV diagnostic questionnaire, allowing us to assess the impact of FGIDs in multiple regions of the GI tract. In addition, a broad range of questions regarding other important lifestyle, medical and general health factors were included in the survey and used in our analyses to further understand associations with oesophageal symptoms.
Our study also has limitations. It was an online survey with self-reported symptoms, and no objective evaluation of whether an organic disease could explain the symptoms was present. The new Rome IV criteria require an endoscopic evaluation, 24-hour pH monitoring and manometry to make a diagnosis of a functional oesophageal disorder, which was unavailable in our cohort. 10 Even though we tried to include a representative cohort from the general population, some sectors of the population were less likely to be represented in the study population. People without internet access and non-English speaking minorities were unable to participate for obvious reasons. However, as we have reported elsewhere in detail, our survey samples in each of the countries were representative of their respective national adult populations. 12 Finally, another limitation is that most of the symptoms that we analysed could have been caused by GERD. 6 Even though we excluded participants who had previously been diagnosed with GERD, it is possible that some of the symptoms included in our results were caused by undiagnosed GERD.
In this study, we have provided the first report of the population prevalence of the four symptoms used to define Rome IV functional oesophageal disorders and identified some of the important predictors of these symptoms. We also demonstrated the relevance of these symptoms from the patients’ and societies’ perspective, since they are associated with substantial healthcare consumption and reduced QoL. Further studies are needed in order to confirm these results in other populations.
Footnotes
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Ethics approval
Before data collection started, the study was reviewed by the ethical committee in North Carolina, USA, and was approved but was deemed not to formally require an ethical approval as the subjects were completely anonymous. The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki.
Informed consent
All participants indicated thier informed concent at inclusion.