
Abstract
Background
Perforation is the most serious complication of esophageal foreign bodies. Studies examining the association between diabetes and esophageal foreign body-induced perforation are largely non-existent.
Objectives
The purpose of this study was to identify the risk factors for esophageal foreign body-induced perforation.
Methods
A retrospective chart review of patients with esophageal foreign bodies between January 2012–January 2017 was performed at the Chinese People's Liberation Army General Hospital. The patients were divided into two groups: those complicated with perforation and those without perforation. Date on patient demographics, symptoms, foreign bodies, and diabetes were collected and analyzed. Study-specific odds ratio and 95% confidence intervals (CI) were estimated using multivariable logistic regression models.
Results
Of 294 patients with esophageal foreign bodies (41.84% male, mean age, 56.73 years), 33 (11.22%) complicated by perforation. Diabetes (odds ratio = 6.00; 95% confidence interval = 1.72–20.23), duration (>24 h) of foreign bodies retention (odds ratio = 4.25; 95% confidence interval = 1.71–10.86), and preoperative fever (odds ratio = 8.19; 95% confidence interval = 3.17–21.74) were strongly associated with an increased risk of perforation, whereas the sensation of a foreign body (odds ratio = 0.32; 95% confidence interval = 0.09–0.92) was a protective factor of perforation. Glucose level was not observed to have an association among patients with or without perforation.
Conclusions
Diabetes and duration of foreign body retention increase risk for esophageal foreign bodies complicated by perforation, and cases with elevated armpit temperature may represented a more likely perforation compared with those without fever.
Key summary
Summarize the established knowledge on this subject
EFB incurred perforation is related to pointed FBs, duration of FB impaction, and specific kind of FBs. Perforation is the most serious complication of esophageal foreign body, early diagnosis and treatment is the key to the management of EFB-induced perforation.
What are the new findings of this study?
Diabetes was strongly associated with an increased risk of EFB perforation. Armpit temperature was a readily available variable to assess perforation, cases with fever represented a more likely perforation compared with those without fever. FB itself was the fundamental factor leading to acute esophageal perforation, whereas diabetes may play a major role in delayed perforation.
Introduction
The esophagus is the most common lodgment site of ingested foreign bodies (FBs) and is vulnerable to complications such as esophageal perforation, especially in the upper esophagus.1–3 Esophageal foreign body (EFB) is a common emergency but occurs incidentally in adults, may be associated with a series of risk factors include cancer, stricture, eosinophilic esophagitis (EoE), mental retardation and bulimia.4–6 In many cases, FB ingestion is a benign course, and most of the ingested objects will pass spontaneously through the gastrointestinal tract without complications. The majority of the remaining FBs can be removed by endoscope, and a tiny minority require surgical treatment in cases with complications that cannot be resolved endoscopically or after unsuccessful attempts to remove by endoscope.4,7,8 Once complicated by perforation, life-threatening issues (such as severe mediastinitis, thoracic infections, life-threatening hemorrhage, etc.) may follow.9–13 Early diagnosis and emergency management will effectively shorten hospital stays, reduce mortality, and improve prognosis.11,14
Diabetes is associated with a number of complications including heart attacks, strokes, kidney disease, blindness, and foot ulcers, which have roots in damage to small blood vessels, arteries and nervous system.15,16 We noted that many patients with FBs that incurred perforation had a history of type 2 diabetes, but lacked studies examining the association between diabetes and EFB-induced perforation.
In previous reports,4,6,7,17 long duration of impaction, battery or magnet, FBs with a sharp wedge were considered risk factors for perforation. However, these studies have several limitations. First, included factors paid too much attention to the characters of FBs, but ignored the patients’ general condition such as type II diabetes or hypertension.6,17,18 Second, most studies lacked a definite definition on perforation, and details on source population and excluded cases.16,18 Third, some studies are limited by relatively small case numbers or inability to adjust for known confounders in their analyses. 19 Fourth, most studies did not separately analyze children and adults who have significant differences in the kind of FBs.2,3 However, the most important issue seems to be availability of the conclusions to evaluate patients’ condition. After all, we cannot confirm exactly what the FB is and whether it has a sharp wedge before endoscopy or radiological evaluation. Inaccurate estimation may lead us to choose an inappropriate examination, and an inappropriate examination may lead to misdiagnosis (e.g. choosing plain radiography to check patients with non-bony FBs), difficulties for further examination and management, or even worsening of condition (e.g. choosing a barium swallow test to check patients with esophageal perforation).
This retrospective study aimed to identify risk factors for EFB complicated by perforation and determine the association between diabetes and perforation.
Materials and methods
Source population
All data of patients with diagnosis of FB in esophagus or esophageal perforation or esophageal fistula, over the age of 18 years, confirmed by endoscopy or surgery, admitted to the Chinese People's Liberation Army (PLA) General Hospital between January 2012–January 2017, were obtained from hospital electronic medical records database. Given that the majority of patients in our center were adult, we set the age over 18 years to reduce admission rate bias and improve homogeneity to a certain extent. The source population for this investigation consisted of all cases eligible for inclusion. Cases were excluded from the current study if diagnosed with FB in non-esophageal location; FB passed spontaneously or vomited; no FB was found by endoscopy or surgery; or, cases without integral data.
The protocol for the study was approved by Ethical Review Boards of the Chinese PLA General Hospital on 30 November 2017. Our study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in prior approval by the institution's Human Research Committee. After careful and rigorous review, our application for exemption from written, informed consent was approved by the same Ethical Review Boards.
Definitions, data collection
EFB was defined as a FB that was accidentally or deliberately swallowed into the esophagus, unable to pass spontaneously or be vomited consciously, and must be extracted by endoscopy or surgical procedure. Esophageal perforation was defined as the whole layer penetrating injury of esophagus.
Pertinent demographic data that were extracted and analyzed included age, gender, body mass index (BMI), main symptoms at admission, preoperative temperature and glucose level, as well as whether the patients suffered from type II diabetes and hypertension or not. The preoperative temperature was defined as the top armpit temperature from ingested to extracted FBs. A test of glucose level was performed within 24 h before the operation, extracted the unique value or the value before hospitalization provided that multiple values were eligible to avoid interference from operative treatment or bias resulted from thoughtlessness in design. Cases of type II diabetes and hypertension were defined by the diagnosis in the medical records. Pertinent information on FBs was extracted and analyzed, and included type, duration, location, and whether complicated by penetrating injury. FB type was recorded and classified into jujube pit, bony FB, denture, others, respectively. Bony FB referred to bone from fish, chicken, duck, pork, and beef. Others included metal, broken glass, packaged drug, etc. The duration of impaction within 24 h was recorded by the hour, otherwise by the day or specific hours. Location was recorded using the distance between FB and incisor and classified into upper, middle, and lower.
To minimize missing values, we conducted a follow-up on the patients who lacked information on type II diabetes and hypertension in their medical record (see Supplementary Material). Given the purposes of this study were assessment and identification of the risk factors for FB-incurred penetrating injury, irrelevant factors such as duration of endoscopic procedure or surgical intervention, and days of hospitalization were not included.
Expert review
We organized an expert surgery panel, which consisted of three expert surgeons with a minimum of 10 years’ experience dedicated to esophageal surgery. They were to evaluate whether the suspected cases complicated by penetrating injuries by independently reviewed medical records, separately assess evidence on perforation, discuss together and finally list the results and evidence. The main evidence comprised explicit description in endoscopy reports or operation records, imaging findings and diagnoses, as well as clinical diagnosis based on comprehensive manifestations in suspected cases. Cases without enough evidence to justify whether complicated by perforation were excluded (see Supplementary Material). Then, we divided the cases into two groups according to the presence of perforation.
Data analysis
Mean and standard deviation (SD) were used for normally distributed quantitative variables. Median and interquartile range (IQR) were used for quantitative variables with a skewed distribution. To determine risk factors for FB-incurred perforation, quantitative variables were analyzed using Student t test, or Wilcoxon rank-sum test when appropriate. Categorical variables were performed using percentages and analyzed using the χ 2 test or Fisher’s exact test when appropriate. For quantitative variables with a skewed distribution, medians were compared by using the Wilcoxon rank-sum test. Potential risk factors were identified on univariate analysis and valuable factor in theory such as glucose level, were included in multivariate analysis. Then, multivariate analysis assessing risk factors for perforation was performed with binary non-conditional logistic regression. A two-sided p value less than 0.05 was considered to indicate statistical significance in each analysis. All statistical analyses were performed using statistical software package R v.3.4.0.
Results
Patients
In total, 353 consecutive EFB patients who were admitted to our service in the Chinese PLA General Hospital were identified by automatic search in this study. As shown in Figure 1, a total of 59 cases were excluded in turn after manual review according to the exclusion criteria depicted in the Methods section, and 294 patients were finally included in this retrospective analysis. Of these, 33 cases were confirmed as complicated by perforation.
Flowchart of patients in this study. EFB: esophageal foreign body; FBs: foreign bodies.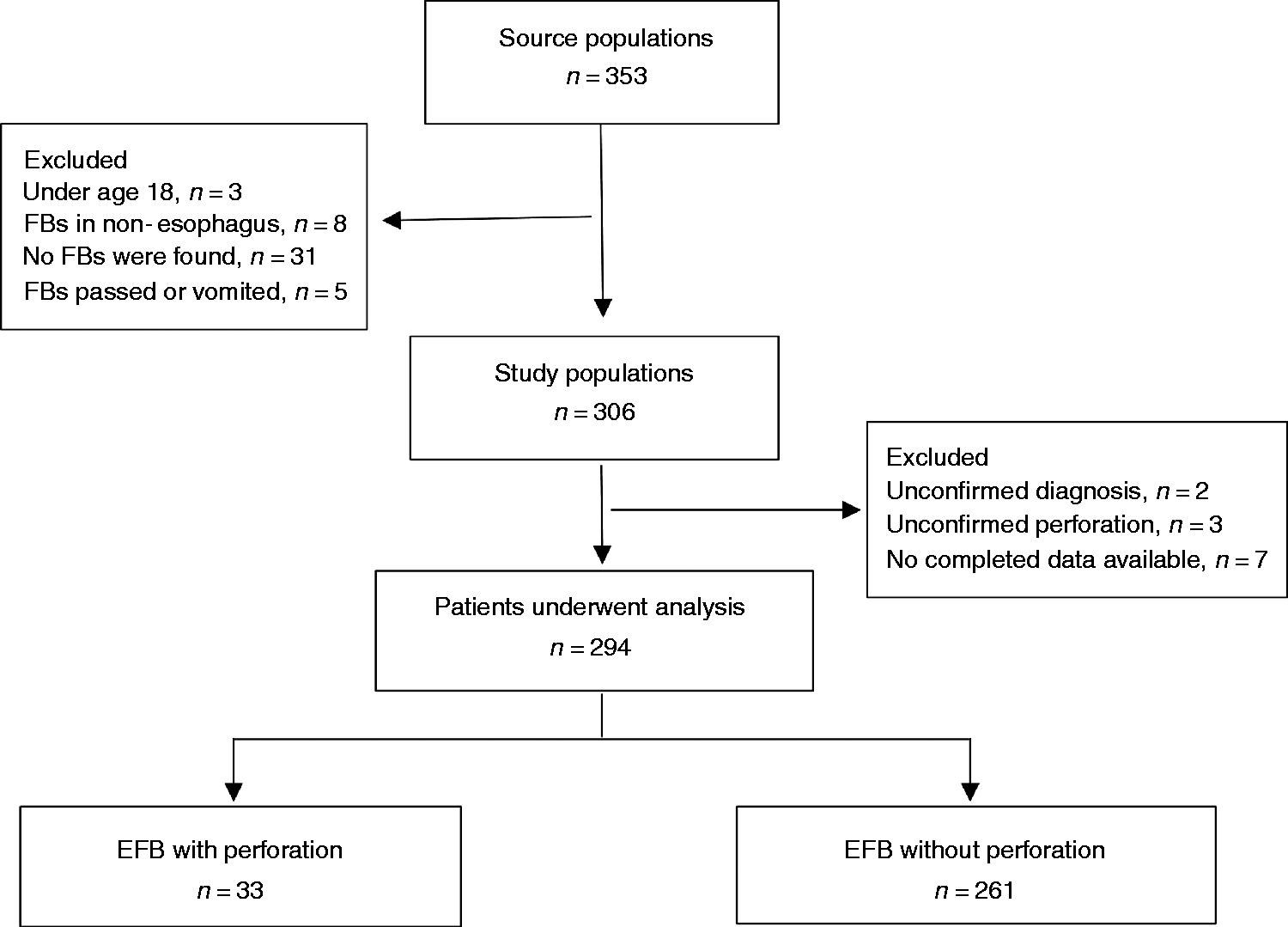
Baseline characteristics.
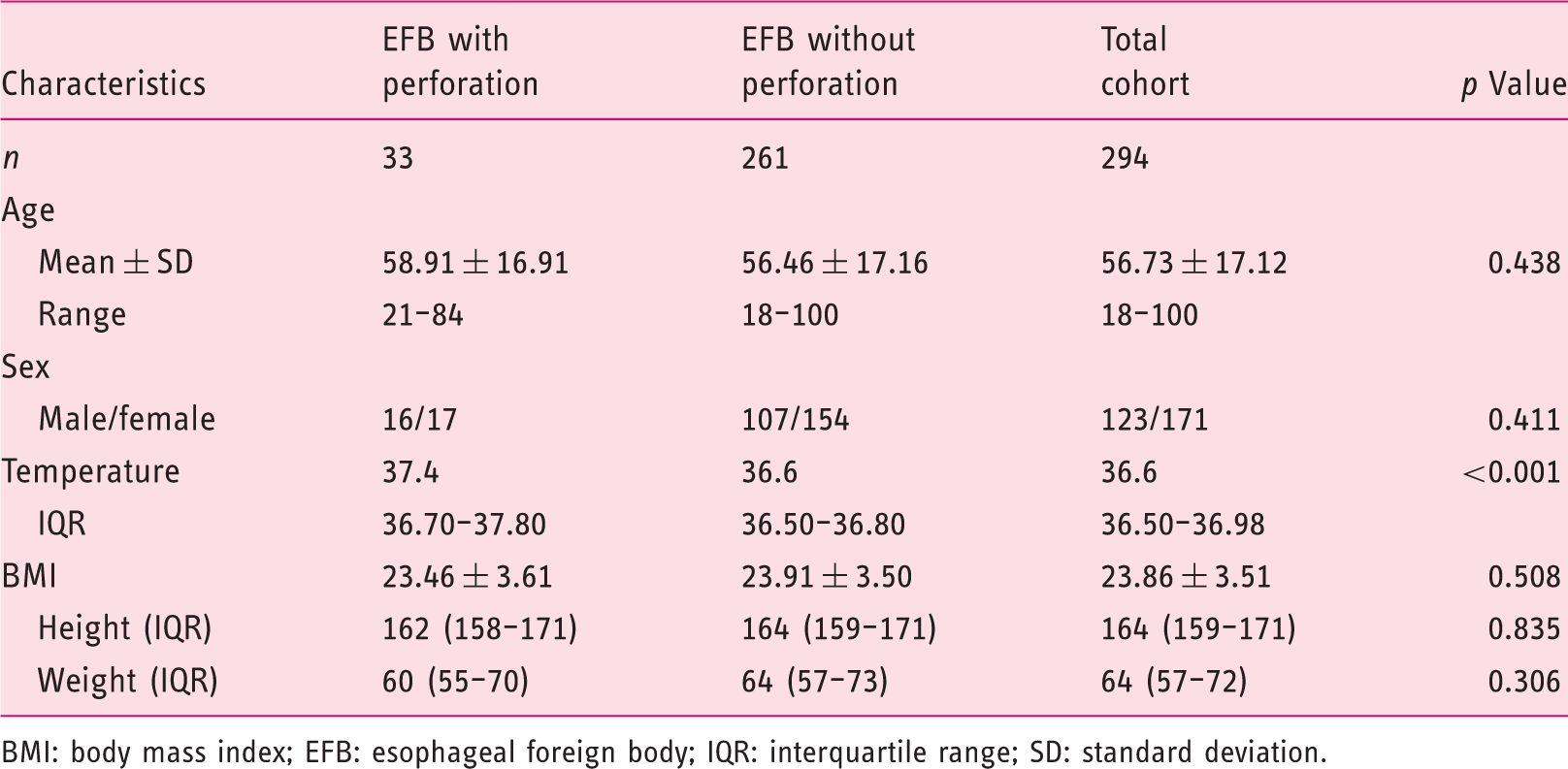
BMI: body mass index; EFB: esophageal foreign body; IQR: interquartile range; SD: standard deviation.
Foreign bodies
The most common type of retained FB was jujube pit (53.06%, 156/294), followed by various bones, dentures and others. FBs were located mainly in the upper esophagus (54.76%; 161/294), followed by the middle esophagus and lower esophagus. Perforation is more likely to occur in the cases with a longer duration of FB impaction and the cases with FBs located in the middle esophagus, but no statistical difference was observed between different kinds of FBs.
Clinical presentations
The most frequent symptomatic complaint after FB ingestion was dysphagia (41.84%, 123/294) and odynophagia (40.82%, 120/294), followed by the sensation of a foreign body, pharyngalgia, chest pain, and others. Fifteen patients did not complain of any symptoms after FB ingestion and were classified as asymptomatic patients. Among them, FBs were most commonly located in the upper esophagus (7/15) and middle esophagus (6/15) when found. FBs located in the lower esophagus are prone to substernal chest pain. The risk for perforation was not associated with dysphagia, odynophagia, and pharyngalgia but associated with the sensation of a foreign body and chest pain.
Diabetes, hypertension and associated upper gastrointestinal (GI) diseases
The positive predictive value of type II diabetes for esophageal perforation is 32%, which indicated one out of every three diabetic patient presentations would be complicated by perforation in the event of EFB. Hypertension did not show a statistically significant difference between the two groups. In addition, five patients (1.7%) had associated GI diseases, two of them suffered from esophageal cancer, one achalasia, one diverticula, and one tongue cancer.
Blood glucose levels within 24 h before operation were included as a variable to analyze when we found that diabetes was a risk factor for EFB perforation, however, no statistical difference was observed between two groups. This may be related to the insufficient samples resulting from the lack of large volumes of relevant data.
Analysis for group jujube pits
To maximally eliminate the effect resulting from different length and sharpness of FBs, we selected the cases with foreign bodies being jujube pits, similar in size and shape, to perform a subgroup analysis (Figure 2). Our analysis showed representativeness of the jujube group from two aspects, one was the greatest sample size, the other was almost the same rate of perforation compared with the total cohort (10.90% jujube vs 11.22% total) and non-jujube group (10.90% jujube vs 11.59% non-jujube, p = 0.85). The results showed the risk factors for EFB-induced perforation are similar between the jujube pit group and the total cohort.
Flowchart of patients with and without jujube pit.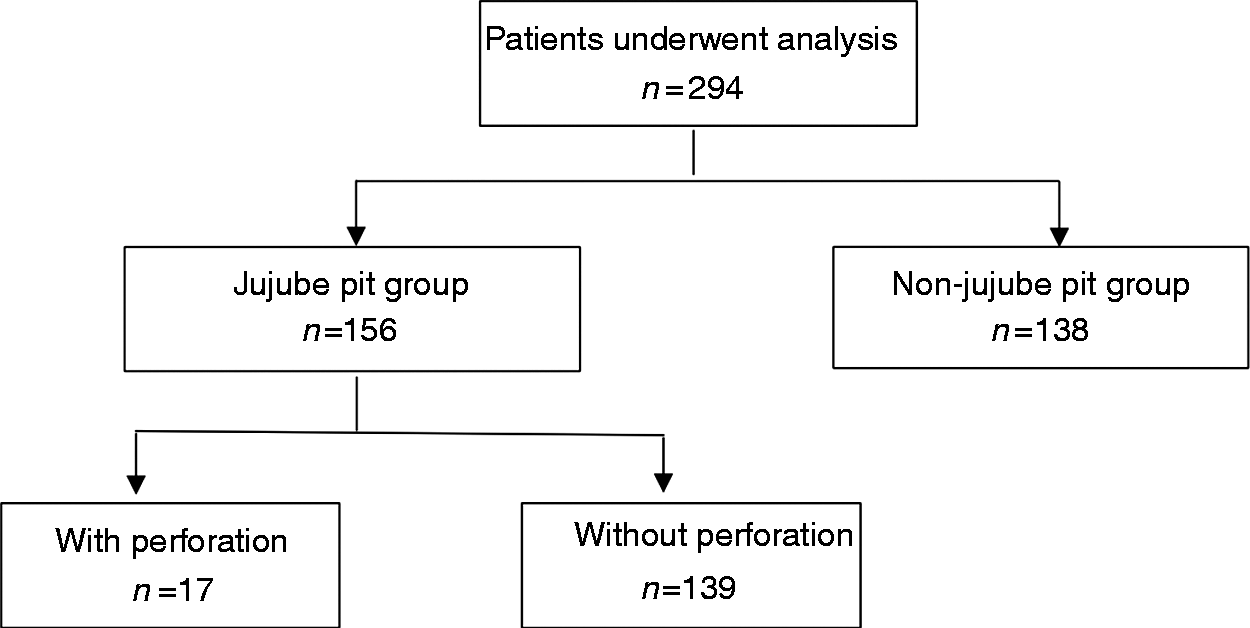
Risk factors for perforation
Results of logistic regression following univariate analysis of risk factors.
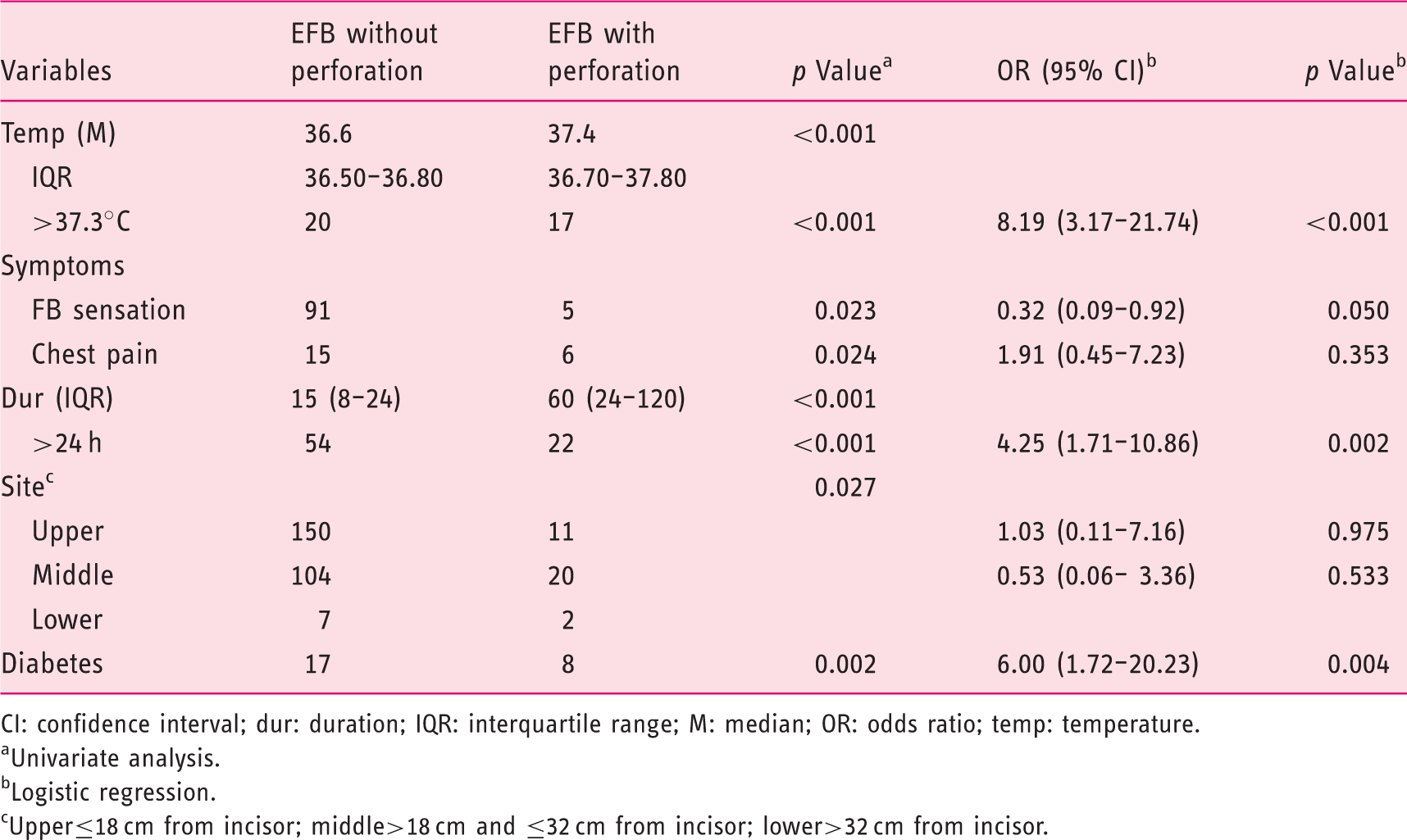
CI: confidence interval; dur: duration; IQR: interquartile range; M: median; OR: odds ratio; temp: temperature.
Univariate analysis.
Logistic regression.
Upper≤18 cm from incisor; middle>18 cm and ≤32 cm from incisor; lower>32 cm from incisor.
Duration between diabetics and non-diabetics
Duration and diabetes.
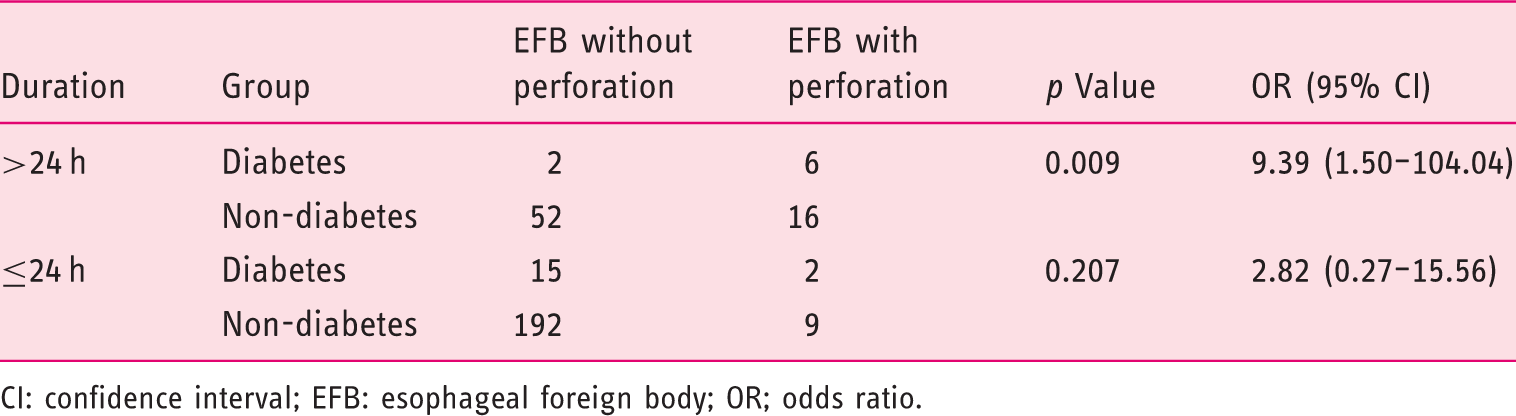
CI: confidence interval; EFB: esophageal foreign body; OR; odds ratio.
Discussion
EFBs can incur a series of complications such as bleeding, ulcer, abscess, among which perforation is the most serious since potentially life-threatening issues like severe mediastinitis and hemorrhage are likely to follow.11,13 Our study confirmed that type 2 diabetes is one of the independent risk factors for perforation of EFB, especially when the duration of impaction exceeds 24 h. We believe that the underlying mechanism of diabetes-induced EFB perforation may lie in impaired wound healing and neuropathy in diabetics.15,20,21 Neuropathy can cause abnormal esophageal motility in most patients with diabetes and sometimes resemble diffuse esophageal spasm,22–24 a logical consequence of neuropathy is that diabetics are more prone to EFB, however, our data are not sufficient to explain this since the prevalence of diabetes in this study is consistent with the current population (8.5% vs 9.7%). 25 Abnormal wound healing in patients with diabetes due to excessive or uncontrolled acute inflammation promoting tissue injury is likely to play a major role. With the prolongation of duration, small injuries incurred by FBs tend to be repaired in non-diabetics and FBs pass spontaneously, 26 whereas in diabetics there is a greater tendency towards worsening injuries and persistent retention, which may cause severe complications like perforation and be aggravated by neuropathy to some extent. Unfortunately, the data of glycated hemoglobin (HbA1c) was unavailable, as it would help to determine if poor blood glucose control in diabetic patients increased the risk of EFB perforation.
The type, size, location and sharpness of FBs, duration of impaction were all considered risk factors for perforation in previous studies. With respect to the type of FBs, the most common is jujube pit, which is different from previous reports and may be closely related to the distribution of jujube and the eating habits of the study subjects.6,17,27 There was no difference in perforation among various FBs in this study, and to eliminate the effect resulting from size and sharpness of FBs, we selected the patients whose FBs were jujube pits to perform subgroup analysis and obtained similar results compared with the total cohort. Prolonged duration of FB impaction are associated with an increased risk of perforation, in line with the majority of previous studies which reported that delaying intervention may produce more complications including perforation.6,28 Consistent with previous reports, the most common location of FB impaction is the upper esophagus,3,29 whereas the most common location of perforation is the middle esophagus in this study.
In addition, we found that FB sensation is the protective factor of perforation, whereas chest pain is a risk factor, indicating that chest pain will cover up the sensation of a foreign body and become the main manifestation when perforation occurs. Some patients with EFBs are asymptomatic, this is more common in patients with FBs in the upper or middle esophagus, with no relation to perforation. Fever is a predictive factor of perforation, and a reasonable explanation is the normal inflammatory response of the body to injuries and mediastinitis after perforation.
An important risk factor for EFBs is upper gastrointestinal disease, which accounted for a high proportion (8–52%) in previous studies but not in our study, and this may related to repeated endoscopy after the removal of FBs.8,17,30 Sperry SL et al. reported that the incidence of EoE, an allergic inflammatory condition of the esophagus that involves eosinophils and regarded as a major factor of EFB impactions in adults, may be substantially underestimated. 30 However, biopsies were not a routine examination in our study and, therefore, we cannot confirm this hypothesis. On the other hand, the prevalence of EoE in Western populations is higher than that of the Japanese population. 31
The rate of perforation is 11.22% and much higher than the majority of studies in which the rate ranged from 0.3–8.5%.3,6,17,32 The reasons for this are likely threefold, the first is that our investigation focused on adult inpatients, the second is that we excluded the cases where no FB was found (n = 31) by endoscopy or surgery, the third is that more patients in a serious condition are prone to hospitalization in our center, a tertiary care center. However, if these factors are taken into account, the odds ratio for diabetes in patients with perforation to those without perforation may be greater and more robust in practice (we can assume that patients with EFBs in other hospitals are characterized by a mild condition and less possibility of coexisting chronic conditions such as diabetes).
Our study has several limitations. First, selection bias is inevitable on account of patients in a poor condition being prone to referral and hospitalization in our institution, although we collected and reviewed all the cases diagnosed with EFBs during the five-year study period. Second, the association between diabetes and perforation cannot be interpreted as causal, although all the data was prior to the perforation being determined. Third, to ensure reliability of the investigation, although we conducted telephone follow-up to replenish missing values for 18 patients who met the inclusion criteria but were without information on coexisting type II diabetes and hypertension, recall bias may followed. Fourth, because this was a single center study focused on adult inpatients, our results may not be generalizable to other populations. However, it is adequate to draw the attention of medical staff and assist them in avoiding missed diagnosis and misdiagnosis. Finally, given the retrospective design of our study and relatively small number of cases with perforation, these results need to be further validated.
In conclusion, our results indicate that type II diabetes is an independent risk factor for patients with EFBs complicated by perforation, meanwhile, a set of accessible variables that would be conducive to estimating whether an EFB was complicated by penetrating injury were identified, which would facilitate doctors in timely and accurate medical decision-making. In particular, when encountering the EFB patients with diabetes and duration of FB impaction exceeding 24 h, increased vigilance for delayed complications such as perforation is necessary. Future research needs to validate these findings in other centers or populations by prospective cohort studies. We advocate for the potential mechanism of diabetes incurring perforation in patients with EFBs to be clarified through fundamental research.
Supplemental Material
Supplemental material for Diabetes is an independent risk factor for delayed perforation after foreign bodies impacted in esophagus in adults
Supplemental material for Diabetes is an independent risk factor for delayed perforation after foreign bodies impacted in esophagus in adults by Shaowei Zhang, Jiaxin Wen, Mingmei Du, Yunxi Liu, Lianbin Zhang, Xiangyang Chu and Zhiqiang Xue in United European Gastroenterology Journal
Supplemental Material
Supplemental tables - Supplemental material for Diabetes is an independent risk factor for delayed perforation after foreign bodies impacted in esophagus in adults
Supplemental material, Supplemental tables for Diabetes is an independent risk factor for delayed perforation after foreign bodies impacted in esophagus in adults by Shaowei Zhang, Jiaxin Wen, Mingmei Du, Yunxi Liu, Lianbin Zhang, Xiangyang Chu and Zhiqiang Xue in United European Gastroenterology Journal
Footnotes
Acknowledgements
The authors would like to express their gratitude towards all patients that participated in this study. They would like to thank the programmer Xu Hongbin for providing technical assistance in collecting data. And, they would like to thank the staff of LinkDoc Data for providing assistance in follow-up to patients without complete information on history of diabetes and hypertension. Author contributions were as follows. Shaowei Zhang: study concept and design, analysis and interpretation of data, drafting of the manuscript, critical revision of the manuscript; Jiaxin Wen: analysis and interpretation of data, drafting of the manuscript, critical revision of the manuscript; Mingmei Du: collection and interpretation of data, critical revision of the manuscript; Yunxi Liu: study design, collection of data, critical revision of the manuscript; Lianbin Zhang: study design, interpretation of data, critical revision of the manuscript; Xiangyang Chu: study concept, analysis and interpretation of data, critical revision of the manuscript. Zhiqiang Xue: study concept, analysis and interpretation of data, critical revision of the manuscript. All authors approved the final version.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Ethics approval
The protocol for this study was approved by Ethical Review Boards of the Chinese PLA General Hospital, and conformed to the ethical guidelines of the 1975 Declaration of Helsinki.
Funding
None.
Informed consent
After careful and rigorous review, our application for exemption from written, informed consent was approved by Ethical Review Boards of the Chinese PLA General Hospital.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.