
Abstract
Background
Several years ago the International Autoimmune Hepatitis Group simplified the previous revised original scoring system for diagnosis of autoimmune hepatitis (AIH) into a scoring system based on only four instead of 13 parameters.
Objective
We aimed to evaluate the suitability of the simplified AIH score for diagnosis of AIH in a German cohort with chronic liver diseases.
Methods
In this retrospective single-center study, we compared the accuracy of both AIH scores in 70 patients with AIH and 211 patients with chronic liver diseases (PBC (n = 52), PSC (n = 27), NASH (n = 67), DILI (n = 15), CHB/C (n = 50)). Sensitivity, specificity and predictability of each scoring system were calculated.
Results
Using the simplified AIH score, the sensitivity and specificity of detecting a probable AIH (scores ≥ 6) were 96% and 97% with a positive and negative predictive value of 92% and 99%, respectively. For diagnosis of definite AIH (scores ≥ 7), the sensitivity and specificity were 43% and 100% with a positive and negative predictive value of 97% and 84%, respectively. The concordance with the revised original criteria was 63%. The specificity for excluding AIH was excellent in both scoring system.
Conclusion
The simplified diagnostic criteria allow a reliable diagnosis of AIH in a German cohort.
Keywords
Introduction
Autoimmune hepatitis (AIH) is a chronic inflammatory liver disease characterized by lymphoplasmocytic interface hepatitis on histological examination, elevated immunoglobulin G (IgG), the presence of autoantibodies and good responsiveness to immunosuppressive therapy.1–3 AIH should be considered in the differential diagnosis of any patient presenting with elevated liver enzymes and/or unexplained cirrhosis, regardless of age, sex and ethnic background. However, clinical presentation of AIH is heterogeneous and ranges from subclinical non-progressive disease 4 up to severe icteric hepatitis and even fulminant liver failure. 5 Levels of serum aminotransferases in patients with AIH vary widely and autoantibodies are not consistently present. Other chronic liver diseases, including viral, cholestatic, drug-induced and non-alcoholic disorders, may display similar clinical, laboratory and histological features.6–9 Thus, the correct and timely diagnosis of AIH may be a challenge in clinical practice. The prognosis of untreated AIH is restricted because natural progression to cirrhosis is even observed in mild disease activity.10,11 These observations underline the importance of diagnosing AIH at early stages of disease.
In 1993, the International Autoimmune Hepatitis Group (IAIHG) codified descriptive diagnostic criteria to standardize AIH patient populations of different study centers for scientific purposes. 12 The IAIHG defined diagnostic criteria to identify patients with having either probable or definite AIH. Subsequently, retrospective validation studies evaluated the utility of these criteria in clinical practice. The specificity for patients to have a definite AIH diagnosis was shown to be 98%, but only 66% for a probable diagnosis. 13 In 1999, the IAIHG revised the descriptive diagnostic criteria to optimize AIH diagnosis in individuals with atypical manifestations. In addition, it aimed to improve exclusion of cholestatic autoimmune liver diseases, such as primary biliary cholangitis (PBC) and primary sclerosing cholangitis (PSC). 14 Nevertheless, its major limitation still was its complexity consisting of 13 components and 29 possible grades. Thus, in everyday clinical use it was not practical. Therefore in 2008, the IAIHG developed the simplified diagnostic criteria for diagnosis of AIH for routine clinical practice. 15 It was based on only four routinely available parameters, including liver histology, autoantibody titers, IgG levels and exclusion of viral hepatitis. From a total of eight points, probable diagnosis of AIH was defined as having a cutoff score of 6 points and definite AIH as having a score of ≥7 points. The simplified criteria were initially defined and validated in a retrospective cohort study including 11 international centers from America, Europe and Asia. 15 It was based on the data of selected AIH patients with well-established diagnosis. Thus, frequency of definite AIH was 100%. Additionally, response to immunosuppressive therapy in all AIH patients was mandatory to be included.
Data on the use of the simplified score in a German cohort within an everyday clinical setting have not been published yet. Therefore, the aim of our study was to evaluate the suitability of the simplified score for the diagnosis of AIH in a German cohort with chronic elevated liver enzymes presenting in routine clinical practice and to compare it with the previous used revised original score for the diagnosis of AIH.
Patients and methods
Diagnostic criteria and study population
In this retrospective study we included 70 patients with AIH diagnosed by the revised original AIH scoring criteria defined by the IAIHG in 199914 as the gold standard for our study. Patients with a pre-treatment score > 15 were defined as a definite AIH and with a pre-treatment score between 10 and 15 as a probable AIH. Only laboratory findings assessed at the time of diagnosis were used. Liver biopsies were performed in all AIH patients before start of immunosuppressive therapy. Liver specimens were evaluated by the local pathologists who were not blinded to the patient’s history. Liver histologies were graded as established for the two scoring systems. In terms of the simplified score, 53 out of the 70 liver biopsies were considered as “typical,” 13 as “compatible” and four as “atypical.” Subsequent response to immunosuppressive therapy (defined in Montano-Loza et al. 16 ) as an additional confirmation of the diagnosis was required in all AIH patients to be included in our study. We next investigated the simplified AIH score in the above-mentioned 70 AIH patients.
To verify the sensitivity and specificity of both AIH scores, we included 211 patients with different chronic liver diseases who were likewise followed in our tertiary referral center for a seven-year period (2006–2013). Medical records from a dedicated database were systematically reviewed with respect to clinical, laboratory, immunological and histological data mandatory to fulfil both the revised original scoring criteria and the simplified scoring system.14,15 Only patients with complete data were enrolled in this study. In addition, liver biopsy was required in all patients.
Diagnoses of control patients were assigned according to the established diagnostic criteria. In brief, chronic hepatitis B was defined according to the European Association for the Study of the Liver (EASL) international consensus conference on hepatitis B. 17 Diagnosis of chronic hepatitis C was met in accordance with the EASL and American Association for the Study of Liver Diseases (AASLD) clinical practice guidelines.18,19 The diagnosis of non-alcoholic steatohepatitis (NASH) was based on the following criteria: (1) persistent abnormal liver enzymes; (2) liver biopsy compatible with NASH; (3) daily alcohol consumption < 20 g; (4) exclusion of other liver diseases.20,21 Drug-induced liver injury (DILI) was considered when the following criteria were met: (1) history of ingestion of drugs and traditional medicine within 12 months of onset of illness; (2) negative viral serology: hepatitis A virus antibodies (anti-HAV) IgM, hepatitis C virus antibodies (anti-HCV), hepatitis B virus antibodies (anti-HBV) IgM (for patients with positive HBsAg, HBV DNA must be undetectable by polymerase chain reaction (PCR) analysis, or with liver biopsy incompatible with HBV; (3) negative serum markers (such as antinuclear antibodies (ANA), anti-mitochondrial antibodies (AMA), coeruloplasmin); (4) daily alcohol intake < 20 g; and appropriate exclusion of other liver diseases. 22 The diagnoses of PBC and PSC were established in accordance with the EASL and AASLD clinical practice guidelines.23,24
In total, 281 patients (57% female) with complete clinical, laboratory, immunological and histological work-up were enrolled in this retrospective study. Seventy patients fulfilled the revised original scoring criteria (pre-treatment score) as having AIH (71% female). The 211 control patients (52% female) were diagnosed as having PBC (n = 52), PSC (n = 27), NASH (n = 67), hepatitis B/C (n = 50) and DILI (n = 15).
Laboratory assessments
All patients obtained conventional laboratory tests of liver inflammation and liver function. Serum electrophoreses and IgG concentrations were assessed via immunonephelometry in all patients. ANA, AMA and smooth muscle antibodies (SMA) were analyzed via indirect immunofluorescence (IIFT) on Hep-2 cells, monkey liver and rat kidney, liver and stomach tissue slides (EUROIMMUN, Germany). Antibodies against liver kidney microsome type I (LKM-1) and AMA-M2 and soluble liver antigen/liver-pancreas antigen (SLA/LP) were determined by using immunoblot assays (EUROIMMUN, Germany), according to the manufacturer’s protocol. Hepatitis B serum markers (HBsAg, anti-HBs, anti-HBc, HBeAg and anti-HBe) and anti-HCV were assessed in all patients via second-generation enzyme-linked immunosorbent assay (ELISA).
Performance parameters
The revised original scoring system and the simplified criteria were applied to all 281 patients. AIH diagnosis was based on the revised original scoring criteria. Sensitivity, specificity and predictability were assessed for each scoring system.
Sensitivity
Sensitivity was calculated as the number of patients diagnosed with probable or definite AIH by the revised original scoring system who were concordantly diagnosed by the simplified scoring system (true positives) divided by the sum of true positives plus the numbers of patients with AIH by the revised scoring system who were undiagnosed by the simplified scoring system (false negatives).
Specificity
Specificity reflected the number of patients without AIH by the revised original scoring system who were also undiagnosed by the simplified scoring system (true negatives) divided by the sum of true negatives plus the number of patients without AIH by the revised original scoring system who were tested positive for AIH by the simplified scoring system (false positives).
Predictability
Positive predictive value reflected the number of true positives divided by the sum of true positives and false negatives. Negative predictive value was reflected the number of true negatives divided by the sum of true negatives and false negatives.
Statistical analysis
All results were expressed as percentages and for continuous variables as medians and range.
For data analysis, SPSS statistical software version 22 (SPSS Inc, Chicago, IL, USA) was applied.
This retrospective study was conducted according to the principles of the Helsinki/Edinburgh Declaration. It was approved by the Ethical Review Committee of the University of Regensburg.
Results
Demographic and clinical data
Seventy patients fulfilled the revised original scoring criteria (pre-treatment score) as having AIH (71% female). Eight of these patients were identified as having AIH-PBC overlap syndrome, whereas three patients presented with AIH-PSC overlap syndrome. Mean age at diagnosis was 49 ± 17 years. At time of diagnosis, 24/70 AIH patients (34%) had histological features of cirrhosis. None of the AIH patients presented with acute liver failure.
Demographic and laboratory characteristics of the study population.
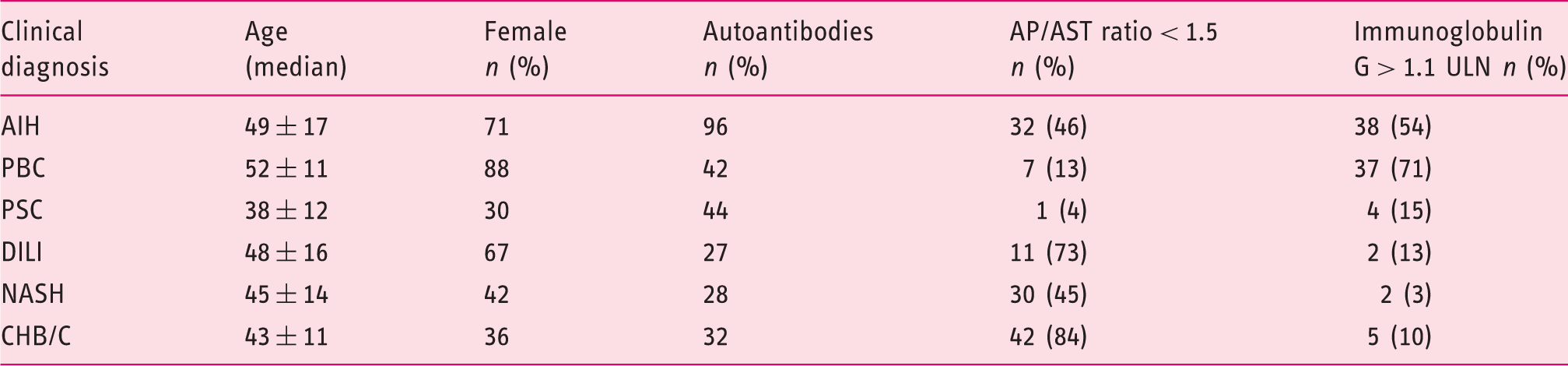
AP/AST: alkaline phosphatase/aspartate aminotransferase; ULN: upper limit of normal; AIH: autoimmune hepatitis; PBC: primary biliary cholangitis; PSC: primary sclerosing cholangitis; DILI: drug-induced liver injury; NASH: non-alcoholic steatohepatitis; CHB/C: chronic hepatitis B/C.
Scoring accordance and scoring discrepancies for AIH
Seventy patients were classified on the basis of the revised original scoring system as having either definite (n = 31) or probable (n = 39) AIH. The simplified criteria identified 67 of these 70 patients as having AIH, whereas three patients were excluded from the diagnosis of AIH. The simplified scoring system graded 30 patients with definite AIH and 37 patients with probable AIH. Both scoring systems identified concordantly 44 patients as having definite AIH (n = 19) or probable AIH (n = 25), resulting in a concordance rate of 63%. Of the 31 patients graded as definite AIH by the revised original scoring system, 12 patients were downgraded to probable AIH using the simplified criteria. Of the 39 patients classified as probable AIH by the revised original criteria, 14 patients were diagnosed as definite (n = 11) or no AIH (n = 3) by the simplified scoring system (Figure 1).
Discrepant autoimmune hepatitis diagnoses based on the revised original (pre-treatment) and the simplified scoring system..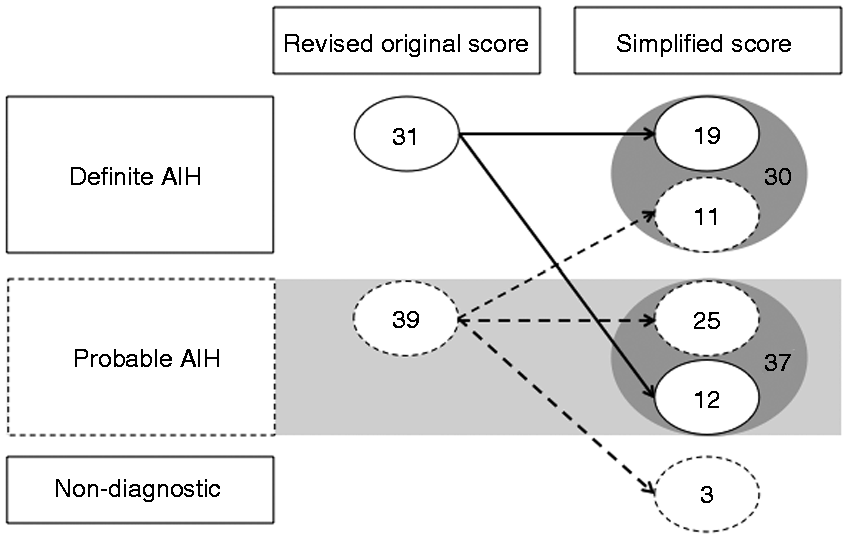
The clinical, laboratory and histological features of the patients with diagnostic discrepancy between the two scoring systems were compared. Patients who were downgraded to probable AIH by the simplified scoring system (n = 12) frequently displayed normal IgG levels (n = 10). In addition, they received points awarded in the revised original but not in the simplified scoring system for female sex (n = 6), concurrent immune disease (n = 3), high-titer autoantibodies (n = 8), alkaline phosphatase/aspartate aminotransferase (AP/AST) ratio < 1.5 (n = 6) and presence of human leukocyte antigen (HLA)-DR 3 or -DR4 (n = 2). Patients excluded from AIH diagnosis by the simplified criteria (n = 3) were all female and presented with normal IgG levels. Furthermore, two out of these three patients showed low ANA titers (1:40) and displayed histologic features compatible with AIH. Points not awarded or subtracted by the revised original scoring system resulted in upgrading of patients to definitive AIH by the simplified criteria (n = 11). These points included male sex (n = 5), lack of concurrent immune disease (n = 6), AMA (n = 6), exposure to potentially hepatotoxic medication (n = 1) and alcohol intake greater than 60 g per day (n = 1). Four of these 11 patients presented with AIH-PBC overlap syndrome.
Performance parameters for diagnosing AIH
Performance parameters of scoring systems for diagnosis of AIH.

PPV: positive predictive value; NPV: negative predictive value.
Using the simplified criteria, we determined an overall sensitivity and specificity for the AIH diagnosis with a score ≥ 6 of 96% and 97%, respectively. The positive and negative predictive values of the simplified scoring system were 0.92 and 0.99 for a probable AIH diagnosis.
When considering a score ≥ 7, the simplified criteria showed an overall sensitivity of 43% and a specificity of 100%, respectively. The positive and negative predictive values were calculated 0.97 and 0.84 for a definite AIH diagnosis.
Comparison of scoring systems for excluding non-AIH diagnosis
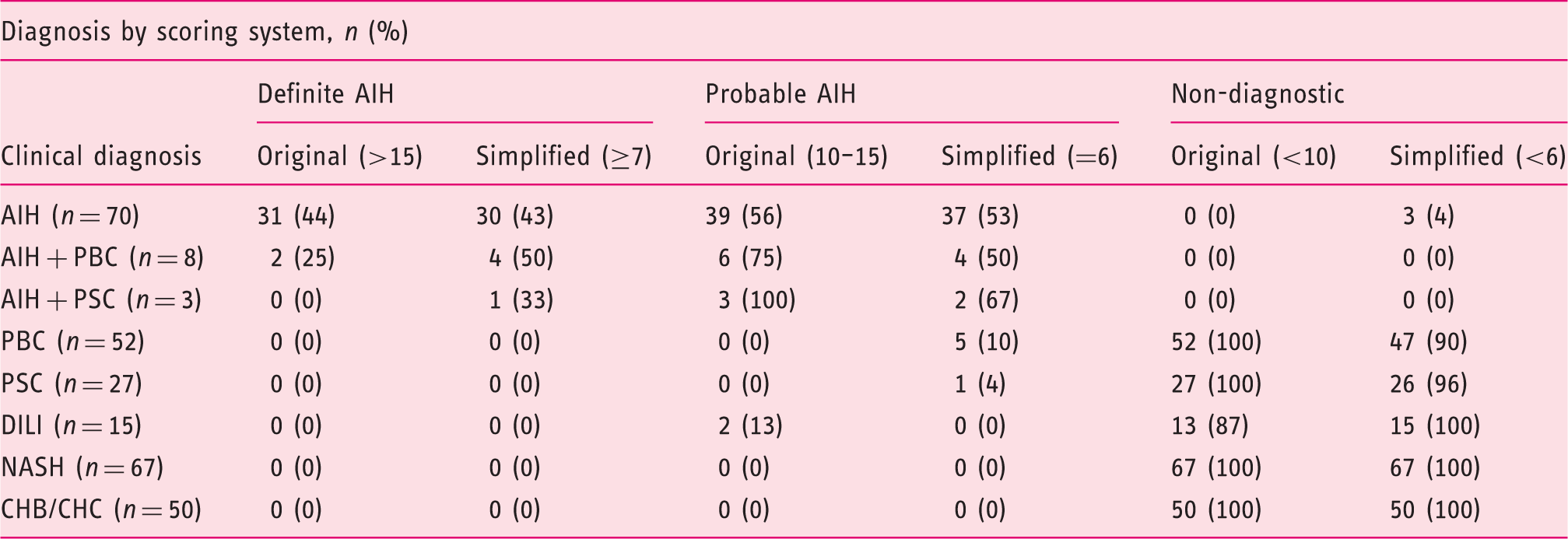
The revised original scoring system graded no patient with chronic hepatitis B/C, PBC, PSC and NASH as having AIH. Two patients with DILI were classified as probable AIH (scores 10 and 11) using the revised original criteria. Both patients were female and presented with a lymphoplasmacytic infiltrate in liver histology and slightly elevated ANA titer. In contrast, the simplified criteria identified one patient with PSC and five patients with PBC as having probable AIH. Noteworthy, neither the revised original nor the simplified criteria graded any patient of the control group as having definite AIH. No patient with chronic hepatitis B and C and with NASH was diagnosed as probable or definite AIH by each scoring systems (Figure 2, Table 3).
Discrimination of AIH patients and controls using points scored by the revised original (pre-treatment) and the simplified diagnostic criteria. Comparison of clinical diagnoses and scoring diagnoses. AIH: autoimmune hepatitis; PBC: primary biliary cholangitis; PSC: primary sclerosing cholangitis; DILI: drug-induced liver injury; NASH: non-alcoholic steatohepatitis; CHB/C: chronic hepatitis B/C.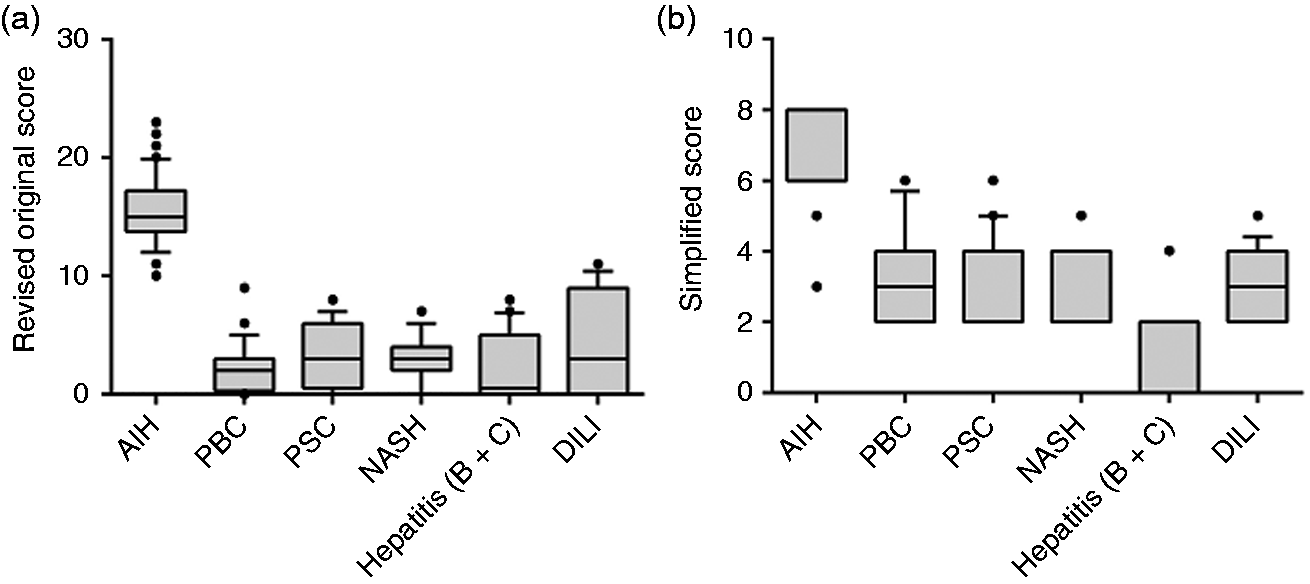
Discussion
In this retrospective study, we evaluated the suitability of the simplified and the revised original scoring system for the diagnosis of AIH in daily clinical practice in a German cohort with chronic liver diseases.
Diagnosis of AIH in our study population was based on the revised original scoring system prior to initiation of treatment. Thus, by definition, overall sensitivity for this scoring system was 100%. Using the simplified criteria, we determined an overall sensitivity and specificity for the AIH diagnosis (score ≥ 6) of 96% and 97%, respectively. For the diagnosis of definite AIH (score ≥ 7), we estimated a sensitivity and specificity of 43% and 100%, respectively. Hennes et al., 15 who created the simplified scoring system in 2008, reported a 88% sensitivity and 97% specificity for the diagnosis of probable AIH (cutoff ≥ 6) and a 81% sensitivity and 99% specificity for the diagnosis of definite AIH (cutoff ≥ 7). This initial validation study comprised patients from Europe (Germany, among others) as well as Asia and South and North America. Therefore, the aim of our study was to investigate the suitability of the simplified AIH scoring in a German cohort. Several other studies have validated the simplified scoring system for diagnosis of AIH in Hispanic, Italian, Chinese, Korean and American patients.25–28 Among these, the sensitivity and specificity for probable AIH ranged from 65% to 95% and from 90% to 98%, respectively. In terms of definite AIH diagnosis, the sensitivity and specificity ranged from 15% and 87% and 99% to 100%, respectively. Thus, the performance parameters of the simplified scoring system determined in our German cohort are comparable to the previous published data.
However, sensitivity for definite AIH was rather low (43%) compared to the overall sensitivity of AIH (96%). Yet, in routine clinical practice overall sensitivity for AIH diagnosis is most relevant. Classification of AIH as definite and probable by the diagnostic scores is principally based on serum levels of laboratory, serological and autoimmune abnormalities. It does not reflect differences in disease severity or prognosis.29,30 And most notably, it does not predict treatment response. 31 Concordance rate between the two scoring systems in designating probable and definite AIH was 63% in our study, which is line with previous studies. 27 Twenty-six out of 70 patients were variously categorized as having definite AIH by the one scoring system and probable AIH by the other system. Noteworthy, discrepant classification as definite and probable AIH did not affect therapeutic management as the indication for treatment was based on the clinical manifestation of disease severity. In addition, the three AIH patients who were classified as non-diagnostic by the simplified score did respond to immunosuppressive therapy, thereby confirming the diagnosis. Two of these three patients relapsed after withdrawal of treatment as a further confirmation of the AIH diagnosis. Thus, treatment response might be considered as an additional criterion to be included in the simplified score and should be further studied.
The simplified diagnostic criteria strongly rely on performing liver biopsy in every patient. Using the simplified score, liver histology is a prerequisite for the diagnosis of definite AIH. But also for reliable AIH diagnosis in patients with atypical features, liver biopsy and careful histological examination are essential. In the present study, the simplified diagnostic criteria downgraded (n = 12) or even excluded (n = 3) patients from AIH diagnosis who presented with atypical features such as normal IgG levels (n = 13/15). In addition, two out of the three patients excluded from AIH diagnosis showed low ANA titers (1:40). An increase in gammaglobulins and particular a selective elevation of IgG in the absence of cirrhosis is a diagnostic hallmark of AIH. But normal IgG levels cover a wide range because of the genetic variability of IgG levels in healthy humans. Some patients physiologically display low baseline IgG levels. During disease activity IgG levels rise significantly from baseline, but may still remain within upper normal ranges. Approximately 5% to 10% of AIH patients are reported to present with normal IgG levels at time of diagnosis. 32 In our study population, 39% (27/70) of the AIH patients displayed normal IgG levels, indicating a high proportion of atypical AIH manifestations. The simplified diagnostic criteria allowed diagnosis of AIH in these patients beside high titer of autoantibodies only in the presence of liver histology classified “typical” for AIH. Detailed communication about the patient’s clinical history and close cooperation between hepatologists and pathologists are therefore critical for optimizing the diagnostic accuracy and the patient management.
In the present study, the simplified diagnostic criteria identified one patient with PSC and five patients with PBC as having probable AIH. None of the PBC and PSC patients were classified as AIH in the revised original scoring system. Patients presenting with clinical, serological and/or histological features of PBC/PSC and AIH have long been recognized and have often been described as overlap syndromes. 33 A recent study in patients with overlapping features of AIH and PBC concluded that these patients suffered from a more aggressive form of PBC with a hepatitic course. 34 These patients benefit from a combined therapy with ursodeoxycholic acid (UDCA) and low-dose immunosuppression. The simplified criteria allow the diagnosis of AIH also in patients with PBC and PSC. The score helps to identify patients with autoimmune liver disease who require immunosuppressive therapy. In contrast, the revised original criteria tend to exclude the diagnosis of AIH in patients with cholestatic features.
One limitation of our study is the retrospective study design and the relatively small number of patients. So far, all published studies validated the simplified criteria only retrospectively. A prospective evaluation of the simplified scoring system is still pending. We believe that our findings are of great clinical importance as they reflect the real-world data derived from everyday clinical practice in a German liver center.
In conclusion, the simplified scoring system is very useful in everyday clinical practice since diagnosis of AIH is based on just four routinely available parameters (IgG, autoantibodies, histology and absence of viral hepatitis). Moreover, it displays a very high overall sensitivity and specificity for the diagnosis of AIH (score ≥ 6). For patients highly suspicious for AIH diagnosis but with atypical features, the revised original scoring system may help to avoid false-negative diagnosis. Both scoring systems therefore complement one another according to the particular clinical situation.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethics approval
This retrospective study was conducted according to the principles of the Helsinki/Edinburgh Declaration. It was approved by the Ethical Review Committee of the University of Regensburg.
Informed consent
Not applicable as this is retrospective study.