
Abstract
Background
The role of menopausal hormone therapy (MHT) in the development of pancreatic cancer is inconclusive owing to small studies and lack of proper study design.
Methods
This population-based matched cohort study included all Swedish women who used systemic MHT between 1 July 2005 and 31 December 2012. For each user of MHT, three never-users of MHT were randomly selected, matched for childbirth, history of thromboembolic events, and previous hysterectomy, as well as for year of birth, diabetes, obesity, and smoking- or alcohol-related disorders. Multivariable conditional logistic regression was used to calculate odds ratios (ORs) and 95% confidence intervals (CIs) for the association between MHT use and pancreatic cancer. The effect of MHT duration on pancreatic cancer development was calculated using multivariable Poisson regression.
Results
There were 290,186 ever-users of MHT and 870,165 matched never-users. During the follow-up, 311 (0.0011%) ever-users of MHT and 1220 (0.0014) never-users developed pancreatic cancer. In a multivariable adjusted model, ever-users had a 23% reduced risk (OR 0.77; 95% CI: 0.68–0.87) of pancreatic cancer. This risk decreased by 35% (incidence rate ratio (IRR) 0.65; 95% CI: 0.33–1.27) in women who used MHT 1–2 years and by 60% (IRR 0.40; 95% CI: 0.18–0.88) in women who used MHT ≥ 3 years compared to women with <1 year of MHT use. The type of MHT did not change the results.
Conclusion
Systemic MHT use might reduce the risk of pancreatic cancer.
Background
Pancreatic cancer is the fourth leading cause of cancer death in the world. 1 The tumor is often diagnosed at an advanced stage without possibility of surgery with curative intent owing to unspecific symptoms and late clinical presentation. 2 Even after surgery the prognosis remains poor with 5-year survival rates below 20% for the majority of patients. 3
Cigarette smoking, high body mass index, particularly during early adulthood, and diabetes mellitus are known risk factors for pancreatic cancer.4–7 The effect of sex hormones, particularly estrogens, has been a matter of debate. It is known that women are less likely to develop pancreatic cancer and this is not fully explained by the differences in exposure to the known risk factors. Both normal and neoplastic pancreatic tissues express estrogen and progesterone receptors. 8 Estrogen has been reported to inhibit pancreatic cancer cell growth in experimental studies.9–11 Thus, it is plausible that sex hormones might affect the risk of pancreatic cancer in women.
Several epidemiological studies have assessed the role of hormonal factors, including menopausal hormone therapy (MHT) in postmenopausal women, in the development of pancreatic cancer.12–22 None of the case-control studies found any association between MHT use and pancreatic cancer.13,14,17,18,22 However, most case-control studies were hampered by a non-random control selection, i.e. controls were patients treated for non-neoplastic conditions in the same hospital where pancreatic cancer patients received treatment,13,14,17,22 or control selection by random digit dialing. 18 The results of the cohort studies have been inconclusive.12,15,16,19–21 However, only one recent study, with detailed information of MHT use, showed a statistically significantly 30% reduced risk of pancreatic cancer MHT users compared to non-user. 12
Our aim was to conduct a large population-based matched cohort design to study the association between systemic MHT use and pancreatic cancer in Swedish women using national population-based registers.
Methods
Study design
This study was a nationwide population-based matched cohort study that included female residents in Sweden older than 40 years without any history of cancer (not including non-melanoma skin cancer) since 1 July 2005. Subjects were followed up until occurrence of exocrine pancreatic cancer, death or the end of follow-up in 31 December 2012. The Swedish Prescribed Drug Registry was used to assess exposure to MHT before 1 January 2013. The Swedish Cancer Registry was used to identify incident exocrine pancreatic cancer. History of diseases and surgical procedures was retrieved from the Swedish Patient Registry. Record linkage was made possible using the Swedish National Identification Number which uniquely identifies each Swedish resident. 23 The study was approved by the central ethical review board in Stockholm, Sweden.
Sources of data
The Swedish Prescribed Drug Registry was established in July 2005 and includes information on all prescribed and dispended drugs in Sweden. The registry is complete for the entire Swedish population (including only <0.3% patient identity data for all items). 24 Information on, relevant drugs according to the Anatomical Therapeutic Chemical (ATC) classification system, date of drug dispensation, and mode of administration was collected.
The Swedish Cancer Registry has registered information on all incident cases of cancer in Sweden since 1958. All cancers are recorded according to the International Classification of Diseases (ICD) codes using the 7th and the current version of ICD. 25
The Swedish Patient Registry was established in 1964 and since 1987 has national coverage on all inpatient care and since 2001 national coverage on outpatient specialist visits in Sweden. 26 Each record includes, among other data, information on discharge diagnosis and surgical procedures.
The Cause of Death Registry has information on all deceased Swedish residents since 1952 and data on cause-specific death are 99.2% complete. 27
Exposure identification
Women older than 40 years who received at least one prescription of MHT (ATC codes: C03C for estrogens, G03D for progestins, G03F for estrogen and progestins) during the study period were identified (n = 1,227,314). Exclusions were made for non-systemic use of MHT (n = 529,868), MHT prescription after 31 December 2012 (n = 86,816), prescription of progestins without concomitant prescription of estrogen (n = 283,333), age < 40 years at time of first MHT prescription (considered as premature menopause or other indications for MHT) (n = 18,739), and previous malignant cancer excluding non-melanoma skin cancer (n = 18,372). In total, there were 290,186 women exposed to systemic MHT, i.e. oral or transdermal administration route.
Women older than 40 years not receiving any MHT medication during the study period were identified (n = 2,281,118). Exclusions were made for previous history of malignant cancer excluding non-melanoma skin cancer (n = 171,020).
Matching procedure
All women exposed to systemic MHT were randomly matched to three unexposed women. Since the matching was a computationally intensive procedure, we decided to stratify the dataset first, in effect making this an exact matched sample for the stratifying variables and a nearest neighbor matched sample for the other variables. Three stratifying variables, i.e. childbirth, history of thromboembolic events, and previous hysterectomy, were initially used to create eight strata of data. Within each of these strata we matched on the nearest neighboring control for year of birth, diabetes, obesity, smoking-related- or alcohol-related disorders. Information on history of diseases and previous hysterectomy was retrieved using the Swedish Patient Register (a complete list of ICD and surgical procedure codes is available in the Appendix, supplied as a Supplementary online file).
The matching procedure was based on group-level matching and not individual matching. Thus, no index date could be calculated for the unexposed matched women because of matching on a group level.
Outcome
Using the Swedish Cancer Registry, patients with a histologically verified diagnosis of exocrine pancreatic cancer (ICD-10 code C250, C251, C252, C257, C258, and C259) were identified. Endocrine pancreatic cancer was excluded. Using the C24 World Health Organization classification of histology, the histology code “096” was used to identify adenocarcinoma of exocrine pancreatic cancer.
Statistical analyses
Conditional logistic regression was used to calculate the risk of developing pancreatic cancer comparing women exposed to MHT to matched unexposed women (ever versus never use), expressed as odds ratios (ORs) and 95% confidence intervals (CIs). The statistical analyses included, apart from the exact matching variables (previous delivery, history of thromboembolic events, and previous hysterectomy), the nearest neighbor matching variables (year of birth, diabetes, obesity, and smoking- or alcohol-related disorders), osteoporosis, chronic pancreatitis, and chronic liver disease. The statistical analyses were also stratified for the type of systemic MHT, i.e. estrogen only or combined therapy with estrogen and progestins.
Poisson regression was used to calculate adjusted incidence rate ratios (IRRs) and the corresponding 95% CIs for the effect of MHT use duration and pancreatic cancer using <1 year of MHT use as the reference. Duration of use was categorized in three categories (<1 year, 1–2 years, and ≥3 years). For this analysis, only MHT users since 1 January 2006 were included, so we can assume that the date of the first prescription during the study period is the actual first prescription. Pancreatic cancer cases developed within the first year after initiation of MHT use were excluded to avoid detection bias. The statistical analyses were performed using Stata v.9.4 statistical software (Stata Corp).
Results
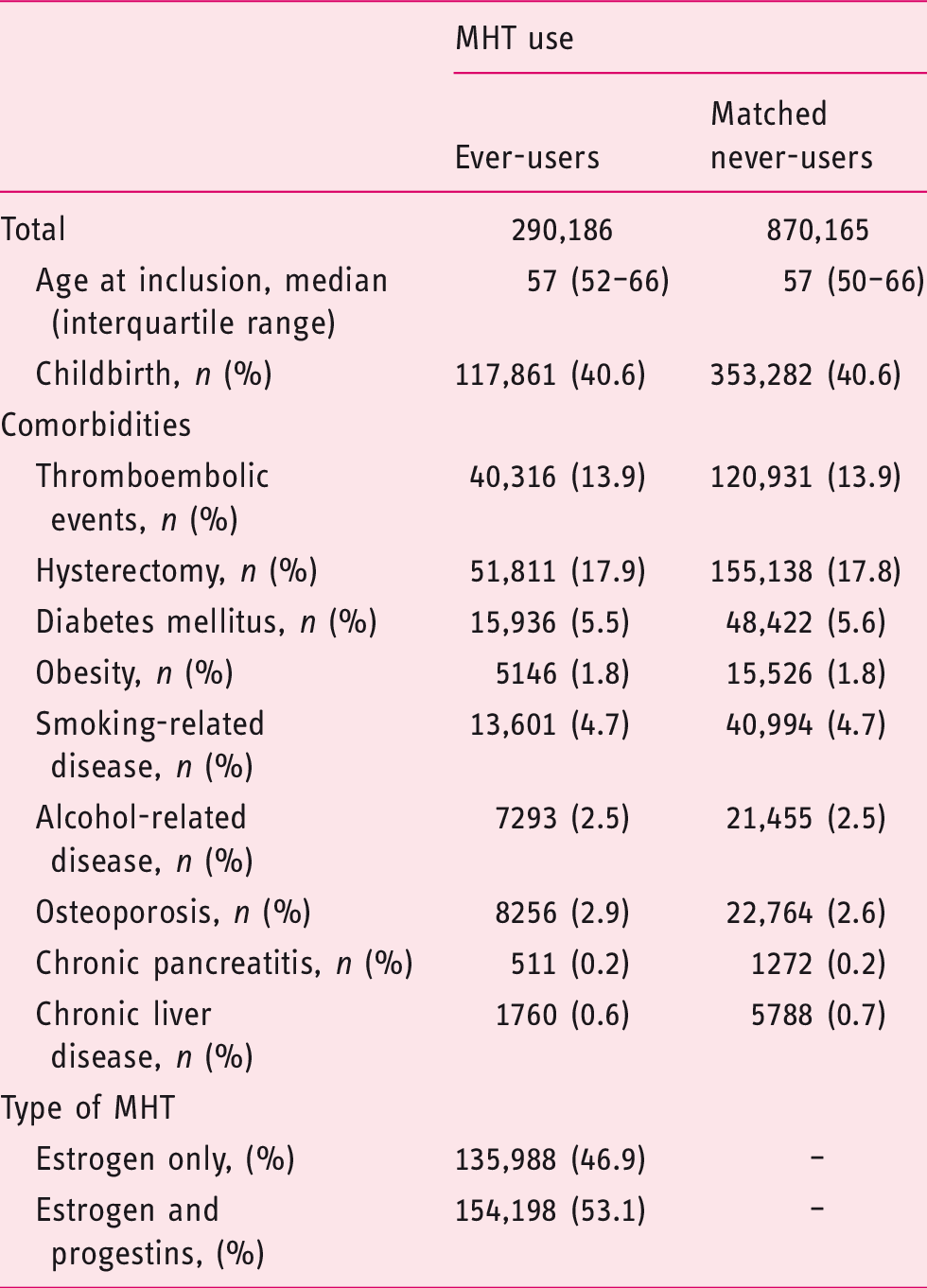
Baseline characteristics of Swedish women older than 40 years of age in relation to their exposure to menopausal hormone therapy (MHT) between 1 July 2005 and 31 December 2012.
Odds ratios (ORs) and 95% confidence intervals (CIs) for the association between menopausal hormone therapy (MHT) use and the risk of pancreatic cancer in Swedish women.
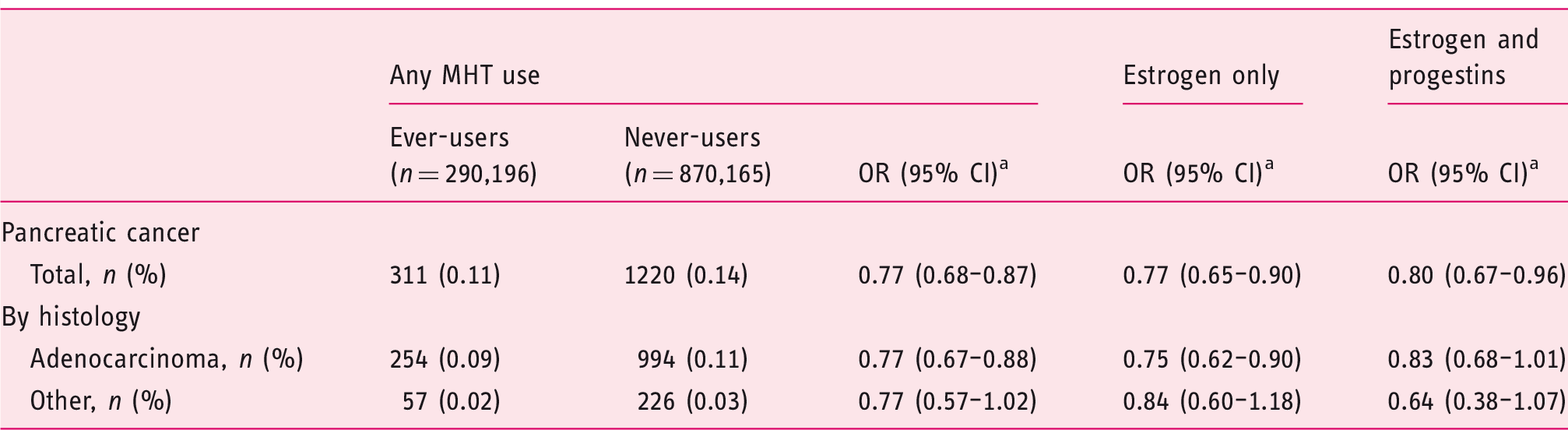
The model was adjusted for childbirth (matching variable), hysterectomy (matching variable), thromboembolic events (matching variable), date of birth, smoking-related diseases, alcohol-related diseases, obesity, diabetes, osteoporosis, chronic liver disease, and chronic pancreatic disease.
Incidence rate ratios (IRRs) and 95% confidence intervals (CIs) for the association between duration of menopausal hormone therapy (MHT) use and pancreatic cancer in Swedish women since 1 January 2006.
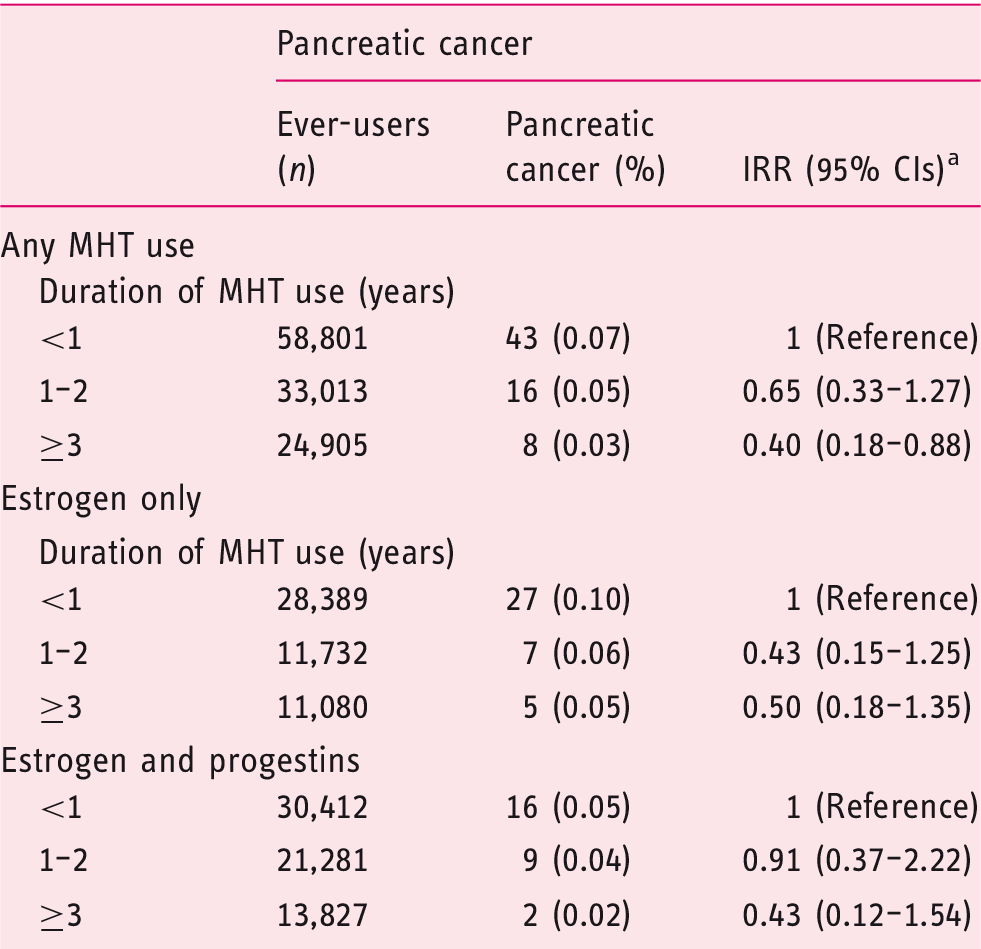
The model was adjusted for childbirth (matching variable), hysterectomy (matching variable), thromboembolic events (matching variable), date of birth, smoking-related diseases, alcohol-related diseases, obesity, diabetes, osteoporosis, chronic liver disease, and chronic pancreatic disease.
Discussion
In this large population-based study, we observed a statistically significant reduced risk of pancreatic cancer in women who used MHT. This association became stronger by longer duration of MHT use. The observed associations did not differ with respect to the type of systemic MHT.
The strengths of this study are the large population-based design, the complete nationwide coverage of Swedish national registries on the MHT exposure and the outcome, and most importantly the accessibility of the Swedish healthcare system to all Swedish citizens. These advantages reduce selection bias and facilitate generalizability of the results. The prospectively collected data on both exposure and the outcome reduced information bias. However, this study has some limitations. There was no information on MHT use prior to 1 July 2005. Thus, we were neither able to investigate the effect of past use of MHT nor the effect of longer duration of MHT use on the development of pancreatic cancer. We also lack information on socioeconomic status. Although the role of socioeconomic status on the development of pancreatic cancer is uncertain, 28 this factor can act as a proxy variable for unhealthy living habits that might affect the development of pancreatic cancer. However, because of universal access to the healthcare system to all Swedish residents, it is unlikely that women were deprived from MHT use because of their socioeconomic status. Furthermore, many of the matching variables, e.g. smoking- or alcohol-related diseases, will act as proxy variables for lifestyle habits. Although the matching procedure ensured similar distribution in potential confounders, residual confounding is possible since there was no individual data on these important confounders. However, we observed a gradually declining risk of pancreatic cancer by the duration of MHT use among women exposed to this medication. It is unlikely that confounding by life-style factors would fully explain these results. Thus, the distribution of residual confounding should be unrelated to the exposure status, i.e. result in non-differential misclassification.
The association between MHT and pancreatic cancer has been studied in several cohort studies.12,15,16,19–21 Whereas no association was found in many of the previous studies, one recent publication showed a decreased risk of pancreatic cancer in users of MHT. 12 This study was based on the California Teachers Study, a cohort study that enrolled over 118,000 women in 1995–1996. Baseline characteristics were collected by self-administered questionnaire. In agreement with our findings, MHT use was shown to reduce the risk of pancreatic cancer by 30% (hazard ratio 0.70; 95% CI: 0.54–0.91) in that study. Furthermore, as also shown by our results, there were no clear differences in the risk of pancreatic cancer in relation to the type of systemic MHT. This highlights the potential protective effect of estrogen in the pathogenesis of pancreatic cancer. Because of lack of multiple measurements, the impact of MHT use duration on the development of pancreatic cancer could not be assessed in that study. In our study, a duration ≥3 years of MHT was strongly associated with a decreased risk of this cancer.
Estrogen and its metabolites have been reported to inhibit pancreatic cancer cell growth in in vitro studies.9–11 2-Methoxyestradiol, a natural estrogen metabolite, has itself cytotoxic properties and potentiates the cytotoxic properties of other chemotherapeutic compounds. 29 However, this combination is associated with high toxicity resulting in death of experimental animals. 29 2-Methoxyestradiol could also inhibit tumor cell growth in cell lines resistant to cytostatic drugs. 30 Thus, estrogen provided as MHT substitution might induce chemoprevention in exposed women and act protective against the development of pancreatic cancer. This might explain the observed reduced risk of pancreatic cancer after relatively few years of MHT use in the current study.
In conclusion, systemic MHT use, irrespective of the MHT type, was associated with decreased risk of pancreatic cancer. Further investigations are warranted to assess if this potential risk reduction remains at long-term after cessation of MHT use.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This work was supported in part by grants from the Centre of Clinical Research, Sörmland County, the Swedish Society of Medicine and Strategic Research Areas by Karolinska Institutet.
Ethics approval
The study was approved by the regional ethical board in Stockholm (number: 2014/1291–31/4).
Informed consent
The study was register-based and informed consent was therefore not applicable.