
Abstract
Introduction
Out of hours admissions have higher mortality for many conditions but upper gastrointestinal haemorrhage studies have produced variable outcomes.
Methods
Prospective study of 12 months consecutive admissions of upper gastrointestinal haemorrhage from four international high volume centres. Admission period (weekdays, weeknights or weekends), demographics, haemodynamic parameters, laboratory results, endoscopy findings, further procedures and 30-day mortality were recorded. Five upper gastrointestinal haemorrhage risk scores were calculated.
Results
2118 patients, 60% male, median age 66 years were studied. Compared with patients presenting on weekdays, patients presenting at weekends had no significant differences in comorbidity, pulse, systolic BP, risk scores, frequency of peptic ulcers or varices. Those presenting on weekdays had lower haemoglobin (p = 0.007) and were more likely to have a normal endoscopy (p < 0.01). Time to endoscopy was less for weeknight presentation (p = 0.001). Sixty-seven per cent of those presenting on weekdays, 75% on weeknights and 60% at weekends had endoscopy within 24 h. Transfusion requirements, need for endoscopic therapy or surgery/embolization, rebleeding rates (6.1%) and mortality (7.2%) did not differ with presentation time.
Conclusion
This multi-centre international study in large centres found no difference in demographics, comorbidity or haemodynamic stability and no increase in mortality for patients presenting with upper gastrointestinal haemorrhage out of hours.
Keywords
Key summary
In this multi-centre international study, patients presenting out of hours (weekends and weeknights) with upper gastrointestinal haemorrhage do not differ in outcome (transfusion, endoscopic therapy, surgery/ embolization, rebleeding, mortality) from those presenting during weekdays. Patients presenting out of hours (weekends and weeknights) with upper gastrointestinal haemorrhage do not differ in respect of comorbidity, haemodynamic stability, risk scores and endoscopic findings. Patients presenting on weeknights with upper gastrointestinal haemorrhage had an upper gastrointestinal endoscopy earlier than those presenting during weekdays or weekends.
Introduction
Upper gastrointestinal haemorrhage (UGIH) is a common cause for emergency admission, resulting in 103–172 admissions per 100,000 per annum.1–3 Despite improvements in endoscopic therapy which have been shown to reduce risk of rebleeding and death, and despite an increase in the number of hospitals providing a dedicated on call service to manage UGIH, mortality from this condition has remained at 8–14%.1–3 This observation may relate to changes in case-mix, with more elderly patients with greater comorbidity presenting with UGIH than previously was the case, and an increase in variceal haemorrhage, which has a worse outcome. 2
Previous studies from Europe and North America have shown increased mortality rates for weekend admissions for many medical and surgical emergencies.4–8 The strength of the weekend effect is variable, and appears dependent upon the conditions studied. The strongest effect was noted for conditions with high acute mortality such as abdominal aortic aneurysm, pulmonary embolism, stroke and subarachnoid haemorrhage 4 and for conditions where acute, more complex intervention may affect outcome, such as myocardial infarction,5,6 renal failure and acute cerebrovascular disease. 6 The underlying reasons for the increase in mortality are disputed. It could be due to patients admitted at weekends being more unwell. An alternative explanation is that it is due to reduced availability of services during weekends. 6 Some studies have suggested that the increased mortality reported for weekend admissions may also apply to patients admitted out-with working hours during the week. 8
Studies of UGIH and the ‘weekend effect’ have reported mixed results. Some studies have shown higher mortality rates for weekend admissions,4,5,9–12 whilst others have not.12–16 All these studies were retrospective, used differing definitions of ‘weekends’, and did not study ‘out of normal working hours’ admissions on weekdays.
The aim of our prospective international study was to compare mortality for patients presenting during weekday daytime hours with those presenting out of hours both during the week and at weekends. As a secondary measure we also compared comorbidity and severity of UGIH as measured by several previously evaluated scoring systems. These include Glasgow Blatchford score (GBS), albumin, international normalized ratio, mental status, systolic blood pressure, age >65 years (AIMS65) score, admission (ARS) and full (FRS) endoscopy Rockall scores and Progetto Nazionale Emorragia Digestive score (PNED). This enabled us to investigate whether there were differences between patients presenting with UGIH at various times during the week. It also permitted recognition of high risk patients to determine whether these patients had poorer outcomes when presenting out of hours. We also assessed the available services and resources for patients presenting with UGIH at weekends in each centre.
Materials and methods
The study was undertaken in Glasgow Royal Infirmary (Scotland, UK), Royal Cornwall Hospital Truro (England, UK), Odense University Hospital (Denmark) and Singapore General Hospital (Singapore). Ethical approval was obtained from West of Scotland Ethics committee (reference 14/WS/0012; project number: 145837) and each centre obtained approval from their local research committee or review board. The study was registered with ISRCTN (reference no. 16235737) and is a subgroup post hoc analysis of data obtained from a study investigating the utility of scoring systems used for UGIH.
Patient ascertainment and management
Consecutive patients with UGIH presenting to the participating hospitals during the 12 month period from March 2014 were included in the study. UGIH was defined by haematemesis, coffee-ground vomiting, or melaena. Patients who developed UGIH while already an inpatient for other reasons were excluded, as were patients aged under 18 years. If a patient presented within a 30 day period from their initial presentation this was considered a ‘re-admission’ and was analysed as part of that presentation. Any patient presenting with a second episode of UGIH outside this timeframe was analysed as a separate admission. Rebleeding was defined as further haematemesis, coffee-ground vomiting, or melaena associated with cardiovascular instability and/or a drop in haemoglobin of >20 g/l developing within seven days of the initial bleeding episode. 17
All patients presenting to each hospital with UGIH were initially assessed in the Emergency Department or acute assessment unit. Time of presentation to the Emergency Department was recorded. Low risk UGIH patients, defined as GBS≤1 (Glasgow and Odense) or GBS≤2 and age <70 years (Truro) were not admitted to hospital unless required for other reasons. These lower risk patients not admitted were managed in the community with early outpatient endoscopy planned, and all are included in our analysis. In Singapore, the practice was to admit the vast majority of patients with UGIH unless decided against based on clinical judgement.
Proton pump inhibitors (PPIs) were not given routinely prior to endoscopy but high dose PPIs, initially as an intravenous bolus followed by infusion, were given to patients with high-risk ulcer stigmata requiring endoscopic therapy (Forrest classification I and IIa,b 18 ) and to other selected patients, depending on clinical judgement. For patients with suspected variceal bleeding, patients were given intravenous vasopressors and antibiotics prior to endoscopy. In all centres, patients with high-risk stigmata of non-variceal bleeding had injection therapy, thermal contact and/or clips, but not adrenaline alone. Band ligation or injection of tissue glue +/− transjugular intrahepatic portosystemic stent-shunt was performed in cases of oesophageal or gastric variceal bleeding respectively. In line with recent evidence and guidelines, blood transfusion was administered at a threshold of 7–8 g/dl or as guided by the clinician in severe haemorrhage. 19
Data collection
Data were collected at each site by a dedicated research nurse, doctor or medical student. The data collected included time of presentation, patient demographics, comorbidities, haemodynamic and laboratory parameters at presentation, as required to calculate ARS, GBS, AIMS65, FRS and PNED scores. Timing of admission, endoscopy and endoscopic findings were recorded, as were interventions including blood transfusion, endoscopic therapy, interventional radiology and surgery; rebleeding, in-hospital and 30-day mortality, and length of hospital stay. A patient was considered a ‘weekday’ admission if they presented 09:00–17:00 Monday–Friday, a ‘weeknight’ admission 17:00-09:00 Monday–Thursday and a weekend admission if they presented 17:00 Friday–09:00 Monday.
Statistical analysis
We compared characteristics, treatment and outcome between patients presenting to hospital during weekday daytime, out-of-hours weekdays, and at weekends. Pearson’s chi-square test and Fischer’s exact test were used to compare proportions. The Kruskal–Wallis equality-of-populations rank test was used to compare medians. Bonferroni correction was applied to counteract the problem of multi comparisons.
Logistic regression analysis was used to estimate the possible association between out-of-hours or weekend presentation and mortality. The regression model was constructed using backward elimination. Candidate variables with a p-value ≥0.15 were evaluated and excluded from the model one by one if a comparison of the full and reduced models using likelihood ratio tests was statistically insignificant. Based on clinical knowledge, the following covariates were included as candidate variables: age (continuous variable; measured in years), sex (male/female), American Society of Anesthesiologists (ASA) score ≥ 3 (yes/no), AIMS65 (continuous variable), systolic blood pressure at presentation (continuous variable), presentation with melaena (yes/no), presentation with syncope (yes/no), haemoglobin measured at time of hospital presentation (continuous variable; measured in g/l), urea measured at time of hospital presentation (continuous variable; measured in mmol/l), creatinine measured at time of hospital presentation (continuous variable; measured in µmol/l), variceal bleeding (yes/no), performance of endoscopic therapy (yes/no), development of rebleeding (yes/no), number of transfusions received during hospital admission (continuous variable), and time from presentation to hospital to performance of endoscopy. Presentation to hospital out-of-hours or at weekends was included as a mandatory variable. Results are presented as odds ratios (ORs) with 95% confidence intervals (CIs). Missing data were handled using listwise deletion.
Based on clinical knowledge, evaluation of potential first order multiplicative interactions was performed using interaction terms. Potential interaction between admission out-of-hours and age, admission out-of-hours and ASA score ≥ 3, admission out-of-hours and performance of endoscopic therapy, admission out-of-hours and AIMS65, admission out-of-hours and rebleeding, age and ASA score ≥ 3, age and rebleeding, age and AIMS65, age and performance of endoscopic therapy, AIMS65 and performance of endoscopic therapy, and AIMS65 and rebleeding were analysed.
To determine whether only patients at higher risk from their UGIH had poorer outcomes from out-of-hours admissions we studied patients with raised GBS or raised AIMS and also those requiring endoscopic intervention separately. AIMS65 ≥ 2,20–24 GBS >1 (indication for inpatient management of UGIH in most units) and GBS >1220,23–26 were used to define higher risk. We also assessed whether the UK centres alone showed a difference in outcomes.
The appropriateness of the underlying assumptions (collinearity, linearity of independent variables and log odds) was examined graphically and statistically. Goodness of fit was evaluated using the Hosmer–Lemeshow test.
Assuming an expected mortality rate of 5% on weekdays,21,22 hypothesized mortality rate of 8% at weekends 9 , with an alpha of 5% and power of 80% the required sample size was 1820 patients. A two-tailed significance level of 5% was used. Data analysis was undertaken using STATA 11.0 (StataCorp, College Station, Texas, USA).
Data and publication
Only the local principal investigator and data recorder had access to patient identifiable data from their centre; anonymized data were sent to SBL for central analysis and are available from SBL on request.
Results
Time of presentation and demographics
Characteristics of patients presenting primarily with upper gastrointestinal haemorrhage.
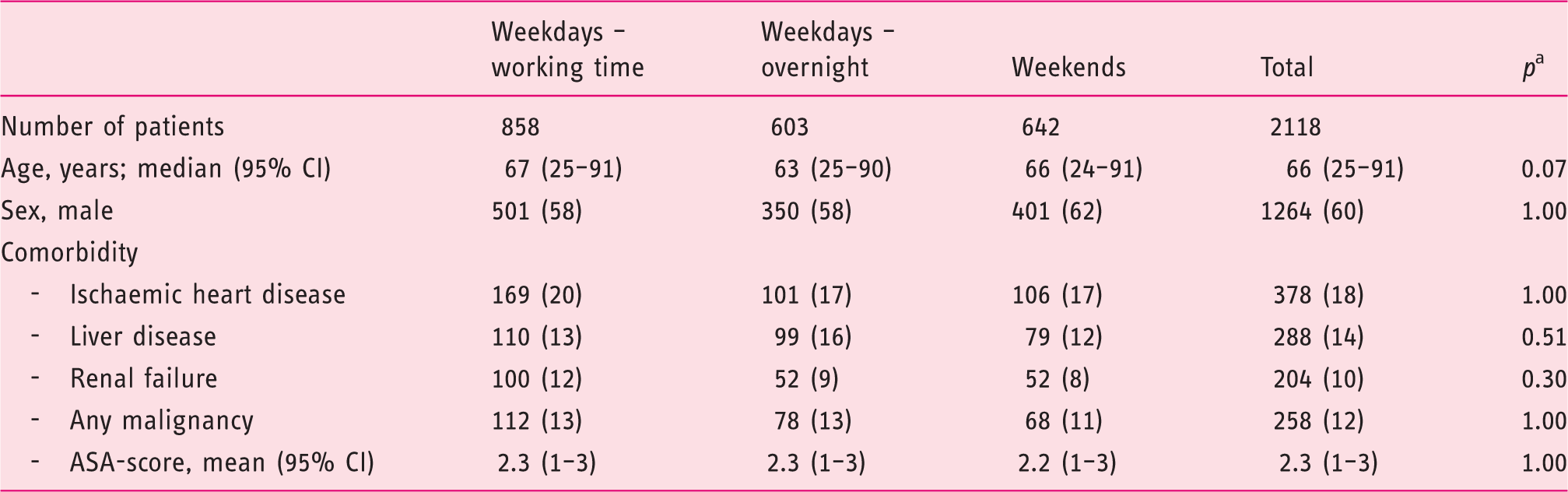
Data are number of patients (%), unless otherwise stated. A total of 2118 patients were included: Glasgow (n = 600), Truro (n = 544), Odense (n = 541) and Singapore (n = 433). There were missing values for time of admission (n = 15), comorbidities (n = 1), ASA score (n = 29).
p-values are Bonferroni corrected.
CI: confidence interval
Severity of upper gastrointestinal bleed
Measures of severity of upper gastrointestinal haemorrhage.
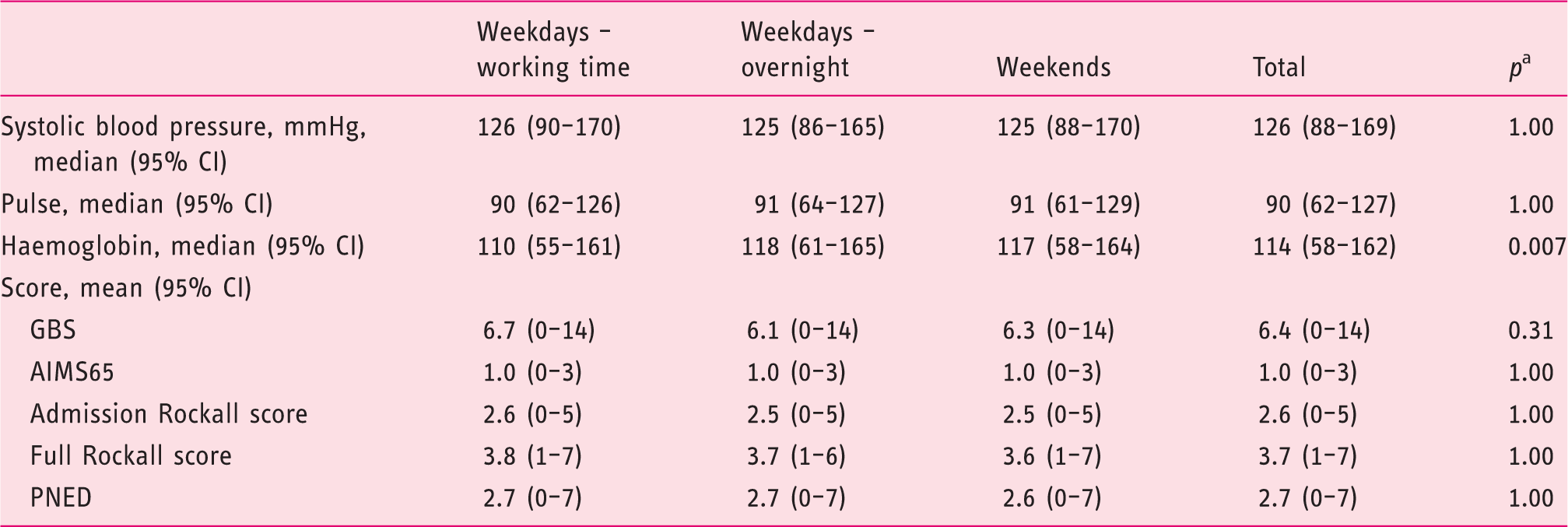
Data are median (95% CI), unless otherwise stated. A total of 2118 patients were included: Glasgow (n = 600), Truro (n = 544), Odense (n = 541) and Singapore (n = 433). There were missing values for time of admission (n = 15), comorbidities (n = 1), blood pressure (n = 39), pulse (n = 38), haemoglobin (n = 18), GBS (n = 66), AIMS65 (n = 267), admission Rockall score (n = 43) and full Rockall score (n = 628).
p-values are Bonferroni corrected.
CI: confidence interval; GBS: Glasgow Blatchford score; AIMS65: albumin, international normalized ratio, mental status, systolic blood pressure, age >65 years; PNED: Progetto Nazionale Emorragia Digestive score
Endoscopy findings and outcomes
Outcome of patients admitted with upper gastrointestinal haemorrhage based on time of presentation.
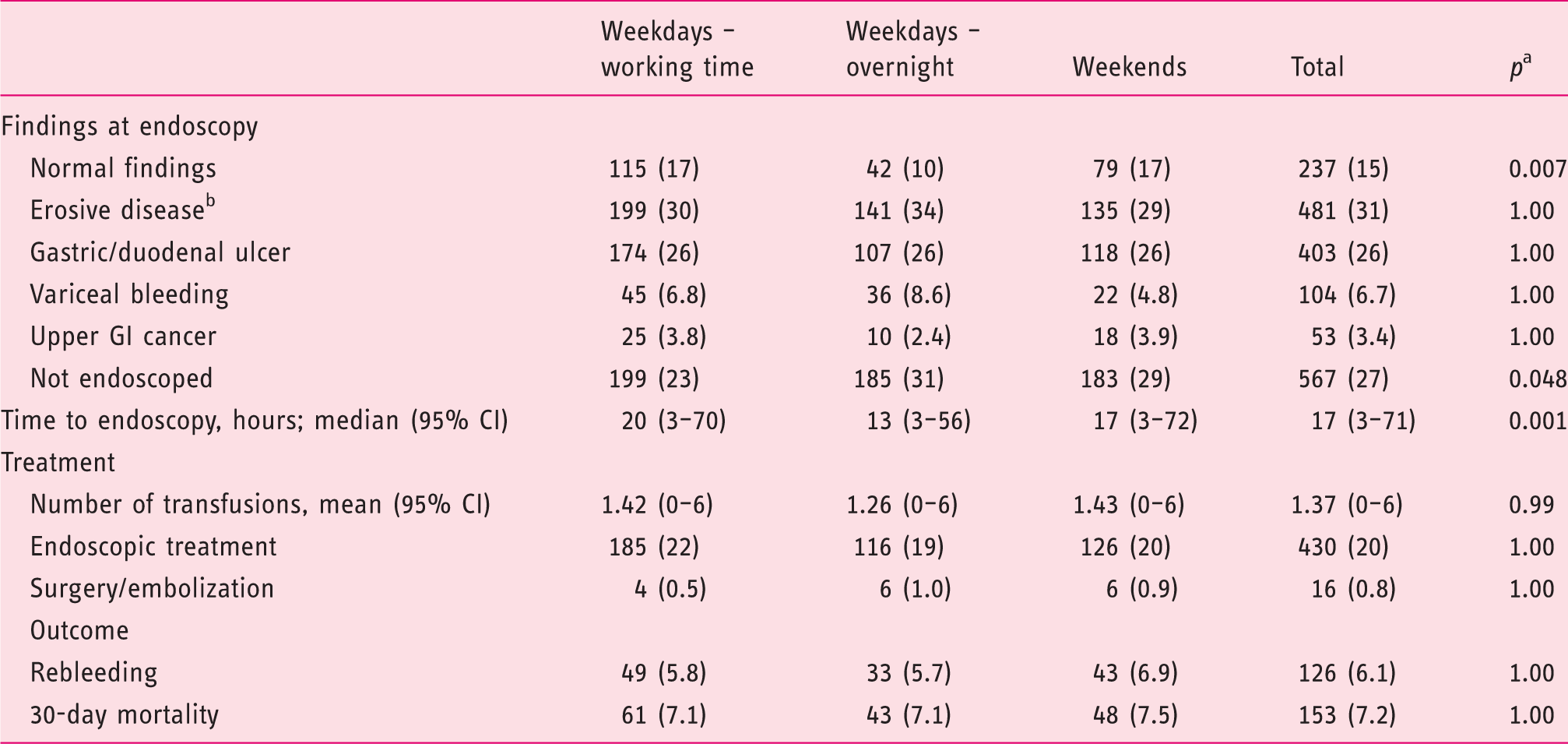
Data are number of patients (%), unless otherwise stated. A total of 2118 patients were included: Glasgow (n = 600), Truro (n = 544), Odense (n = 541) and Singapore (n = 433). There were missing values for time of admission (n = 15), time to endoscopy (n = 69), number of transfusions received (n = 23), performance of haemostatic intervention (n = 4), development of rebleeding (n = 51), mortality (n = 1).
p-values are Bonferroni corrected.
Oesophagitis, gastritis or duodenitis.
CI: confidence interval; GI: gastrointestinal
There were no significant differences in frequency of treatment with transfusion (36%), endoscopic therapy (20%), surgery or embolization (0.8%), rebleeding rate (6.1%) or 30-day mortality (7.2%) based on time of presentation (Table 3). Twenty-four per cent of patients with UGIH and haemoglobin ≥ 70 g/l, systolic blood pressure >100 mmHg and no history of ischaemic heart disease had a transfusion, that is, the clinical decision to transfuse was outside of the generally accepted transfusion algorithm. There was no statistical difference between transfusion rates for these patients between presentation times; 25% of weekday, 20% of weeknight and 25% of weekend patients received a transfusion.
Following adjustment for covariates of prognostic importance using logistic regression analysis, we found no association between admission out-of-hours or weekend and mortality (OR (95% CI): 1.00 (0.62–1.60)). The Hosmer–Lemeshow goodness-of-fit tests showed no indication of poor fit. There was no sign of interaction.
Outcome of higher risk patients with upper gastrointestinal haemorrhage dependent upon time of presentation.
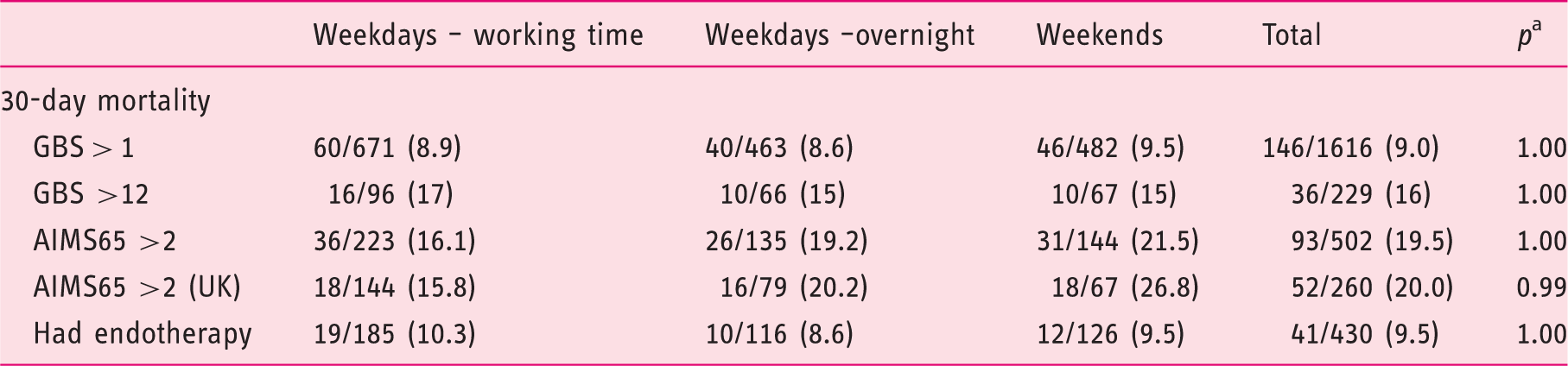
Data are number of patients who died/total within that group (%). A total of 2118 patients were included: Glasgow (n = 600), Truro (n = 544), Odense (n = 541) and Singapore (n = 433). There were missing values for time of admission (n = 15), mortality (n = 1), GBS (n = 66), AIMS65 (n = 267).
p-values are Bonferroni corrected.
GBS: Glasgow Blatchford score; AIMS65: albumin, international normalized ratio, mental status, systolic blood pressure, age >65 years
Outcome of patients with upper gastrointestinal haemorrhage dependent upon time of presentation and site.
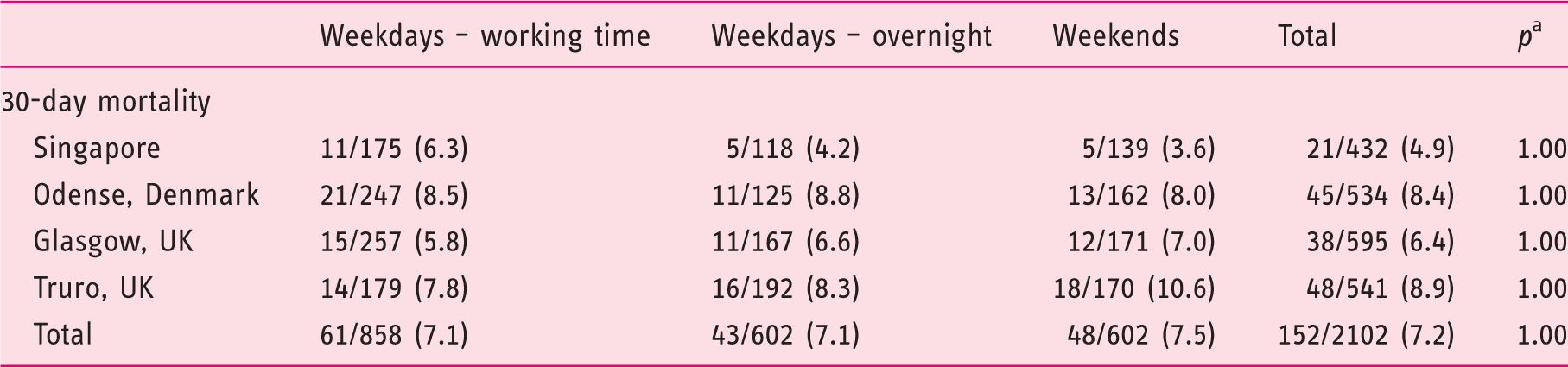
Data are number of patients who died/total within that group (%). A total of 2118 patients were included: Glasgow (n = 600), Truro (n = 544), Odense (n = 541) and Singapore (n = 433). There were missing values for time of admission (n = 15), mortality (n = 1).
p-values are Bonferroni corrected.
Discussion
Increased mortality for patients presenting on weekends has been reported in many countries and for many conditions including some, though not all, studies of UGIH. Conditions with high early mortality or requiring specialist intervention seem most susceptible to a ‘weekend effect’. This is the first study which has prospectively collected data on comorbidity and clinical and laboratory data to enable assessment of patients and their likelihood of adverse outcomes based upon their time of presentation to hospital. We studied not just whether there was a weekend effect but also whether presentation out-of-hours on weekdays also had increased mortality, as has been shown previously for all admissions in a UK district general hospital. 8
We found no significant difference in mortality for patients presenting at weekends compared with those presenting on weekdays or weeknights. This was confirmed following adjustment for confounding factors in a multivariate regression analysis and was consistent for both UK and other centres. We analysed the UK centres separately due to the political importance of out-of-hours outcomes in the UK. It is possible that our study lacked sufficient power to detect a small difference in mortality although it did have power to detect an expected 2% difference. 9 Each centre has senior gastroenterologist input seven days per week with ability to undertake weekend endoscopy as clinically indicated, although during the study period only one (Truro) offered a ‘routine’ endoscopy list for inpatients at weekends, and then only on Sundays. In all centres there is a 24 h on call service including an endoscopist experienced in all therapeutic modalities plus one or two endoscopy trained nurses available. Our study might not be generalizable to smaller units without availability of senior staff out-of-hours.
We have previously shown that GBS is the optimal scoring system for predicting a composite of need for intervention and death and for need for intervention alone. 20 The PNED and AIMS65 were equally effective at predicting mortality and outperformed other scoring systems. 20 In the current study, using AIMS65 and GBS we have shown no relationship between time of presentation and outcome even for higher risk patients.
As data were collected prospectively we have been able to correctly identify patients admitted late on Fridays who would theoretically be most at risk of any weekend effect. The outcome from UGIH is determined not only by availability of endoscopy but also by effectiveness of resuscitation, which could be affected by availability of senior staff. Defining which times of presentation should be considered as ‘out-of-hours’ is complex and we acknowledge that by including those patients presenting near the start of the working day in the ‘out of hours’ group we could potentially have diluted any effect related to presentation time. After discussion, arbitrary definitions of weekday (09:00-17:00 Monday–Friday), weeknight (17:00–09:00 Monday–Thursday) and weekend (17:00 Friday–09:00 Monday) were adopted. We were unable to look at the effect of presentation on holidays, although this has previously been shown not to affect outcomes. 15 Early endoscopy improves mortality rates for patients with high-risk but not low-risk non-variceal haemorrhage. 26 We therefore studied whether there was any effect from presenting out-of-hours with higher risk bleeding and perhaps having delayed endoscopy as a result. Using GBS >1 (patients recommended to have inpatient management of their UGIH), GBS >12 (shown to be high risk in previous studies), AIMS65 ≥2 (those with highest mortality) and finally those receiving endoscopic therapy as surrogate markers for severity of bleeding failed to demonstrate any weekend effect on outcome. Although we found no such effect, it is possible that our study had insufficient power to demonstrate a difference as the number of participants was reduced when studying higher risk groups.
It was unexpected that patients presenting during weekdays actually had the longest time from presentation to endoscopy. It is possible that this relates to protected inpatient spaces being made available on morning (but not afternoon) endoscopy lists specifically for patients with UGIH. Therefore patients presenting late morning or in the afternoon may wait until the following day for their endoscopy. Although not directly studied here it is possible that offering inpatient spaces during afternoon endoscopy lists may reduce time to endoscopy and could improve length of stay and inpatient costs. Others have previously reported shorter time to endoscopy for weekend admissions 15 although most have shown delays.11–13,16
Contrary to some previous studies we did not find any increase in comorbidity 9 nor in haemodynamic instability 14 for patients presenting at weekends. In fact, as reported by others previously, patients presenting on weekdays had lower haemoglobin than those presenting out-of-hours. 15 There was no statistical difference in age or pre- or post-endoscopy scores dependent upon presentation time.
In conclusion, this multi-centre international study indicates that there is no clinically relevant increase in mortality for patients presenting with UGIH at weekends, or out-of-hours weekdays, in high-volume centres with access to around the clock endoscopy. Therefore, increasing out-of-hours availability in such centres is unlikely to have a major impact on mortality for patients with UGIH.
Footnotes
Acknowledgements
Registered with ISRCTN (reference no. 16235737). The paper was written by IAM with input from all co-authors, who approved the final manuscript. Our report follows STROBE guidelines.