
Abstract
Background
The hypothesis is that decision-making for transfusion varies considerably among gastroenterologists. The aim is to identify preferences and predictors of transfusion decision-making in chronic anemia.
Study design and methods
Between February and April of 2015, a computerized adaptive choice-based conjoint survey was administered to gastroenterologists in the Netherlands. The survey included seven patient attributes: hemoglobin levels, hemoglobin stability, age, iron indices, the presence of anemia-related symptoms, cardiovascular comorbidities, and the number of transfusions in the past half year. Predictors of transfusion preferences were assessed by multivariable regression.
Results
113 gastroenterologists completed the survey (response rate = 29%; mean age = 47 years; 24% women). Absolute hemoglobin level was the most important incentive of transfusion, accounting for 42% of decision-making, followed by age (15%), hemoglobin stability (12%), anemia-related symptoms (10%), and cardiovascular comorbidities (10%). A hemoglobin level >9.6 g/dL is an inflection point, where gastroenterologists would not prescribe transfusions. Age of the patient is more important in the decision-making process to younger gastroenterologists (OR −2.9, 95% CI −5.3 to −0.5).
Conclusion
Absolute hemoglobin level is the most important factor to transfusion decision-making. This is contradictory to transfusion guidelines for chronic anemia which address the importance of symptoms.
Keywords
Introduction
Iron deficiency anemia is a common problem in gastroenterology practices and is associated with lethargy, weakness, dyspnea, and a decreased quality of life.1,2 Therefore, treatment of iron deficiency anemia is important to improve the related symptoms. Apart from treating the underlying cause, iron supplementation and/or red blood cell (RBC) transfusions can be given to restore hemoglobin (Hb) level. However, both undertreatment and overtreatment of anemia are associated with impaired clinical outcomes. 3 Therefore, a targeted transfusion regimen with clear defined rules in each patient is the best route to an increased quality of life and clinical outcome. 4
RBC transfusion strategies have become more restricted over the past decade. 5 American, European, and Australian transfusion guidelines for patients with chronic anemia advise transfusion in case of clinical symptoms and below defined Hb level thresholds.6–8 There is no literature published on transfusion practices in gastroenterology, but it is known that there is a wide variation in transfusion practices in perioperative care and critical care patients. 9
It is unknown which clinical factors determine the decision-making process, when and who to transfuse or whether there are differences between gastroenterologists. This decision-making process is complex and although there are guidelines, the interpretation of these guidelines in clinical practice might differ between healthcare professionals. As a corollary we hypothesize that transfusion preferences vary, but that certain gastroenterologists’ characteristics predict behaviors such as gender, years of experience, type of hospital, or subspecialization. More insight in the understanding of and reasons for variation in transfusion practices could lead to targeted strategies to increase awareness among gastroenterologists to adequately prescribe RBC transfusions.
The aim of this study is to identify factors that trigger the use of transfusions in chronic anemia due to gastrointestinal bleeding and characterize the heterogeneity among gastroenterologists regarding transfusion decision-making through a nationwide survey using the adaptive choice-based conjoint (ACBC) analysis technique.
Materials and methods
Study setting
We administered a survey to every gastroenterologist affiliated with the Dutch Association of Gastroenterologists. Over 98% of active gastroenterologists in the Netherlands are member of the Dutch Association of Gastroenterologists. In total, 395 gastroenterologists were invited to participate in this anonymous survey. The survey was sent to invitees by e-mail between February and April 2015, with a reminder up to two times to initial non-responders.
Overview of ACBC analysis
Conjoint analysis is a quantitative method originally developed in applied sciences which can be used to evaluate clinical decision-making in healthcare.10–17 Full control of potentially confounding factors can be achieved by having each participant evaluate the same clinical factors with according levels. As such, conjoint analysis is considered as a good method to effectively analyze decision-making in clinical medicine. 18 Compared with other methods to investigate decision making, such as self-report or absolute ranking of factors, ACBC is more effective in approximating the real world.19,20 Because the decision to transfuse depends on complex combinations of clinical factors that may be interdependent and are weighed by the individual gastroenterologists, ACBC is a good method to investigate this decision-making process.
The administered survey consists of two parts: the ACBC analysis and a set of stand-alone questions regarding provider demographics and practice characteristics. The seven evaluated clinical factors in the ACBC analysis are: Hb level, Hb stability, age, iron indices, the presence of anemia-related symptoms, cardiovascular comorbidities, and the number of transfusions in the past half year. Triggers of transfusion were studied in a scenario of chronic anemia due to gastrointestinal bleeding from angiodysplasias. This scenario was not changed as we do not want to study the underlying disease as a clinical factor, because this is not a trigger according to the guidelines.6–8,21,22
Clinical factors and levels tested in conjoint analysis clinical vignettes.
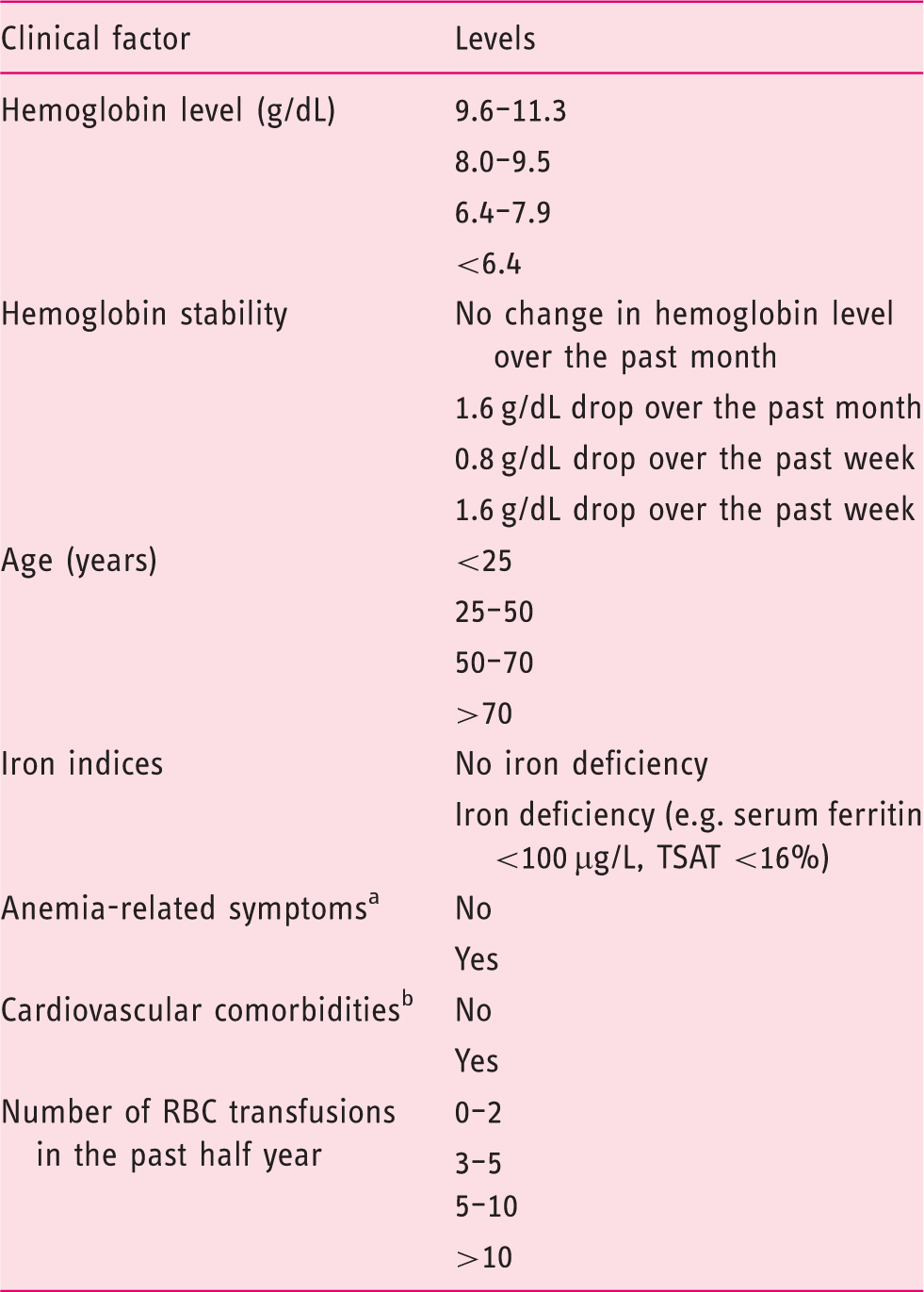
TSAT, transferrin saturation.
Anemia-related symptoms: fatigue and dyspnea.
Coronary artery disease, peripheral artery disease, cerebrovascular accident, or myocardial infarction.
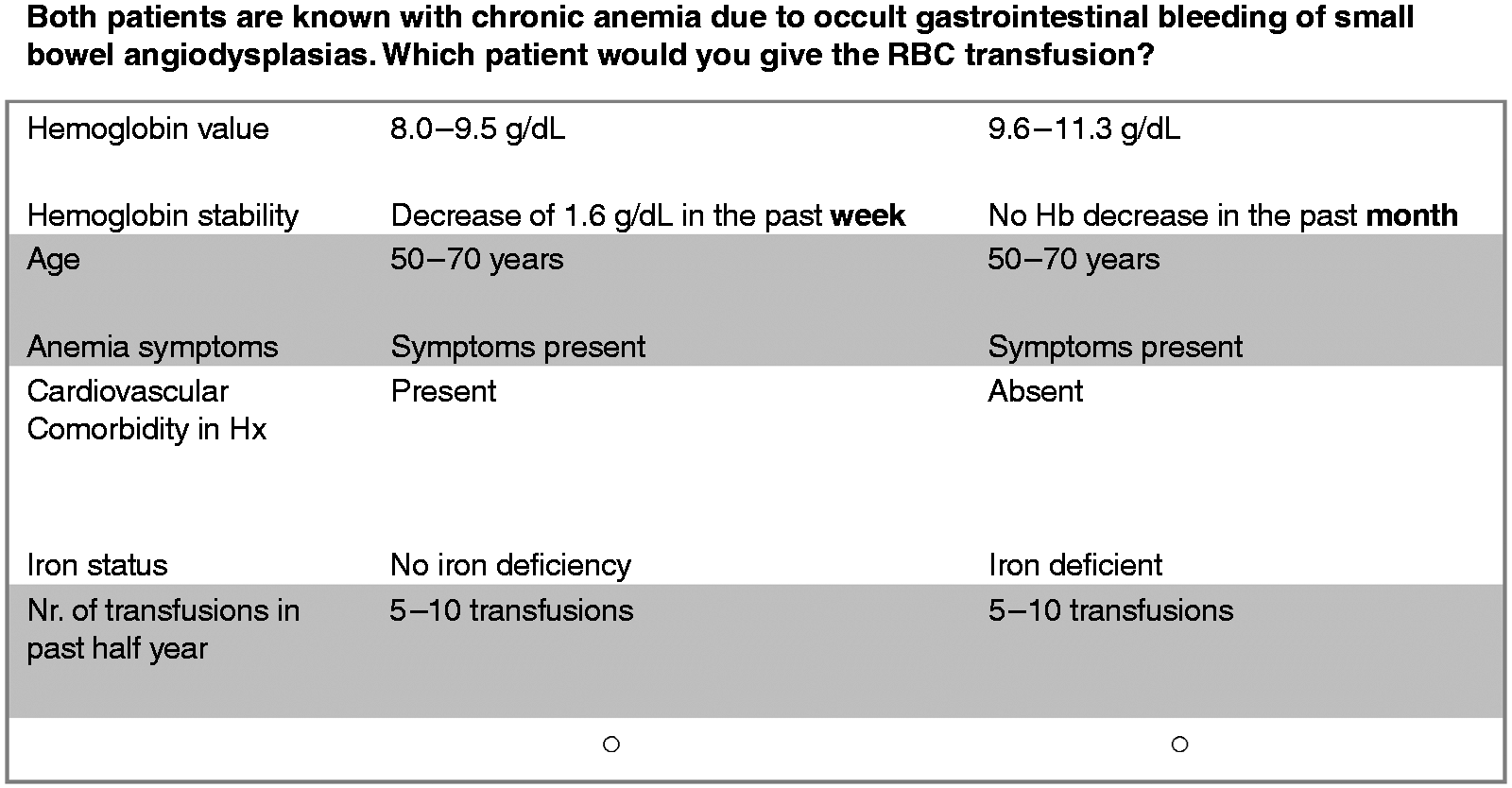
Example of a case vignette.
Survey design
To ensure that the survey adequately queried clinical factors related to RBC transfusion decision-making, we used the British, Dutch and American transfusion guidelines that were current at the time of the survey.6,7,21 Moreover, we piloted the validity of clinical characteristics in a small (n = 8) group of gastroenterologists. The pilot group also advised to include number of transfusions in the past half year as a variable. This process further refined the case vignettes and the levels of clinical factors.
Sample size and statistical analysis
The specific sample size for conjoint analysis (n) should satisfy the equation (nta)/c ≥ 500, where t is the number of tasks, a is the number of alternatives per task, and c is the maximum number of levels for a given attribute. 10 In this survey, providers completed t = 6 tasks with an average a = 3 alternatives and c ≤ 4 levels, based on these parameters a sample size of 110 can be considered sufficient.
The main outcomes are utilities. The utilities indicate how much the difference between the levels of one attribute affects the decision to transfuse. Across the levels of one attribute the utilities add up to 0, which leads to a middle weight around 0. Negative utilities for a certain level do not trigger gastroenterologists to prescribe a transfusion compared to positive utilities, where gastroenterologists do want to prescribe a transfusion. Hierarchical Bayes analysis is used to calculate individual importance for each of the seven clinical factors. The relative importance shows the contribution in percentage of each individual factor relative to the other factors and together they make up 100% of the decision-making. This results in a rank order of the seven clinical factors from most to least important together. We performed descriptive analyses to calculate means and proportions for the gastroenterologist characteristics.
We aimed to predict decision-making behavior (the dependent variable) using clinical factors and their levels as independent variables. We conducted multivariable linear regression analysis to determine if gastroenterologist or practice type characteristics (sex, age, years as a specialist, subspecialization, and type of hospital) predicted individual importance for each of the seven tested clinical factors. Factors were included if the p-value was <0.2 in univariate analysis. Continues independent variables were transformed in binary variables by using the mean /median. For each of these gastroenterologists’ characteristics the association with the individual importance scores of the seven clinical patient factors was calculated by the odds ratio (OR) with 95% confidence intervals (95% CIs). The part-worth utility analyses and individual attribute importance values are automatically calculated by the Sawtooth Software (North Orem, UT, USA). The regression analysis was performed with SPSS Statistics software version 22.0 (IBM, Armonk, NY, USA).
Results
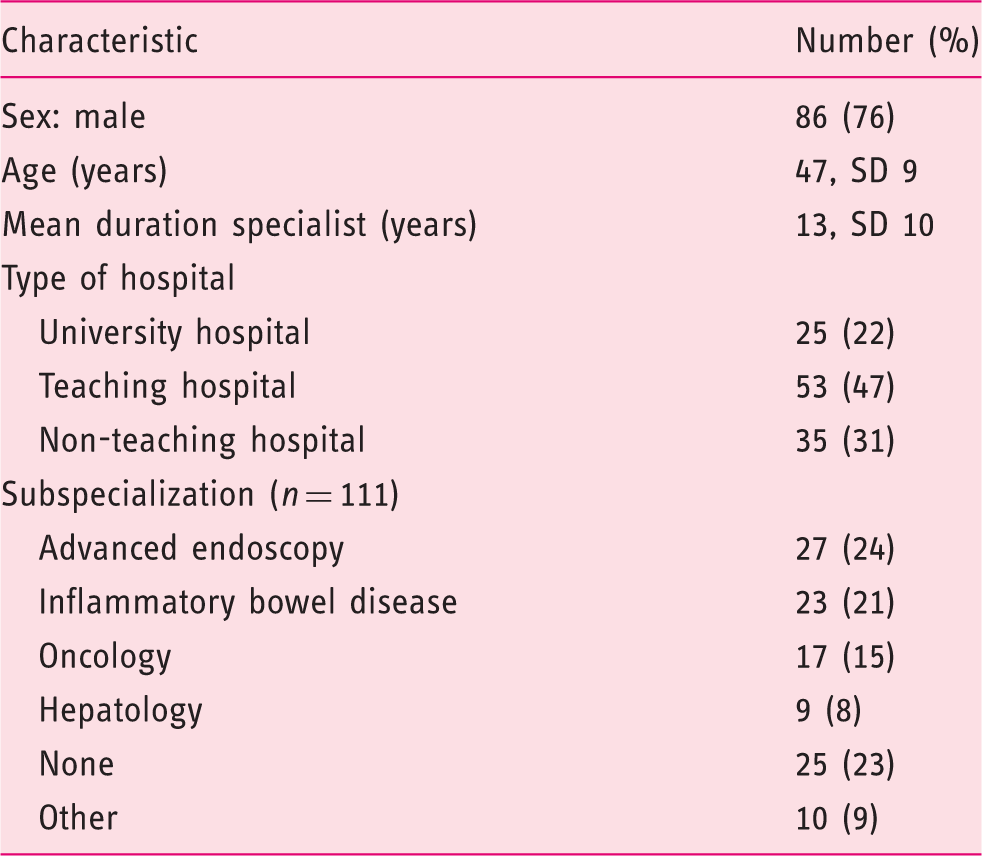
Characteristics of responders
Gastroenterologists characteristics (n = 113).
Rank order of clinical factors
Of the seven attributes assessed, absolute Hb level is the most important incentive for transfusion, accounting for 42% of decision-making, followed by age (15%), Hb stability (12%), anemia-related symptoms (10%), cardiovascular comorbidities (10%), the number of transfusions in the past half year (6%), and iron indices (5%) (see Supplementary figure 1 online).
Inflection points of clinical factors
The inflection point is the point where the utility of a specific level increases or decreases significantly compared to the other levels of the clinical factor. For Hb level the inflection point is 9.6 g/dL, above which physicians do not prescribe transfusions (Supplementary figure 2). Inflection points of the other clinical factors were also calculated (Supplementary figure 3). Hb stability is only an important clinical factor in the decision-making process when the extremes are true, which were no Hb change or a 1.6 g/dL drop over the past week. The average part-worth utilities for the different levels (stable, 1.6 g/dL drop over the past month, 0.8 g/dL drop over the past week, 1.6 g/dL drop over the past week) are respectively −37 (SD 18), 1 (SD 20), 0 (SD 15), and 36 (SD 35). The inflection point for age of the patient is 25 years, e.g. below this age gastroenterologists are not triggered to prescribe transfusions.
Preferences for transfusion dependent on gastroenterologist characteristics
In multivariable linear regression, age of the gastroenterologists was a predictor for the importance in decision-making process of the patient’s characteristic age (OR −2.9, 95% CI −5.3 to −0.5). Younger gastroenterologists (<47 years) value the patient’s age 2.9 times more than older gastroenterologists in their decision-making process to transfuse. Sex, type of hospital, and subspecialization were not predictors in multivariable regression analysis for the importance of any of the seven clinical factors in the decision-making process.
Discussion
This study provides insight in the decision-making process concerning RBC transfusion in everyday gastrointestinal practice. Of all clinical factors, absolute Hb level is the most important incentive of RBC transfusion in patients with chronic anemia. The inflection point in decision making is an Hb level of 9.6 g/dL, above which gastroenterologists are averse in prescribing RBC transfusions. Symptoms, age of the patient and iron indices are less important in the decision making process. Transfusion preferences are dependent on the gastroenterologists’ age.
Guidelines recommending transfusion strategies in (chronic) anemia. a
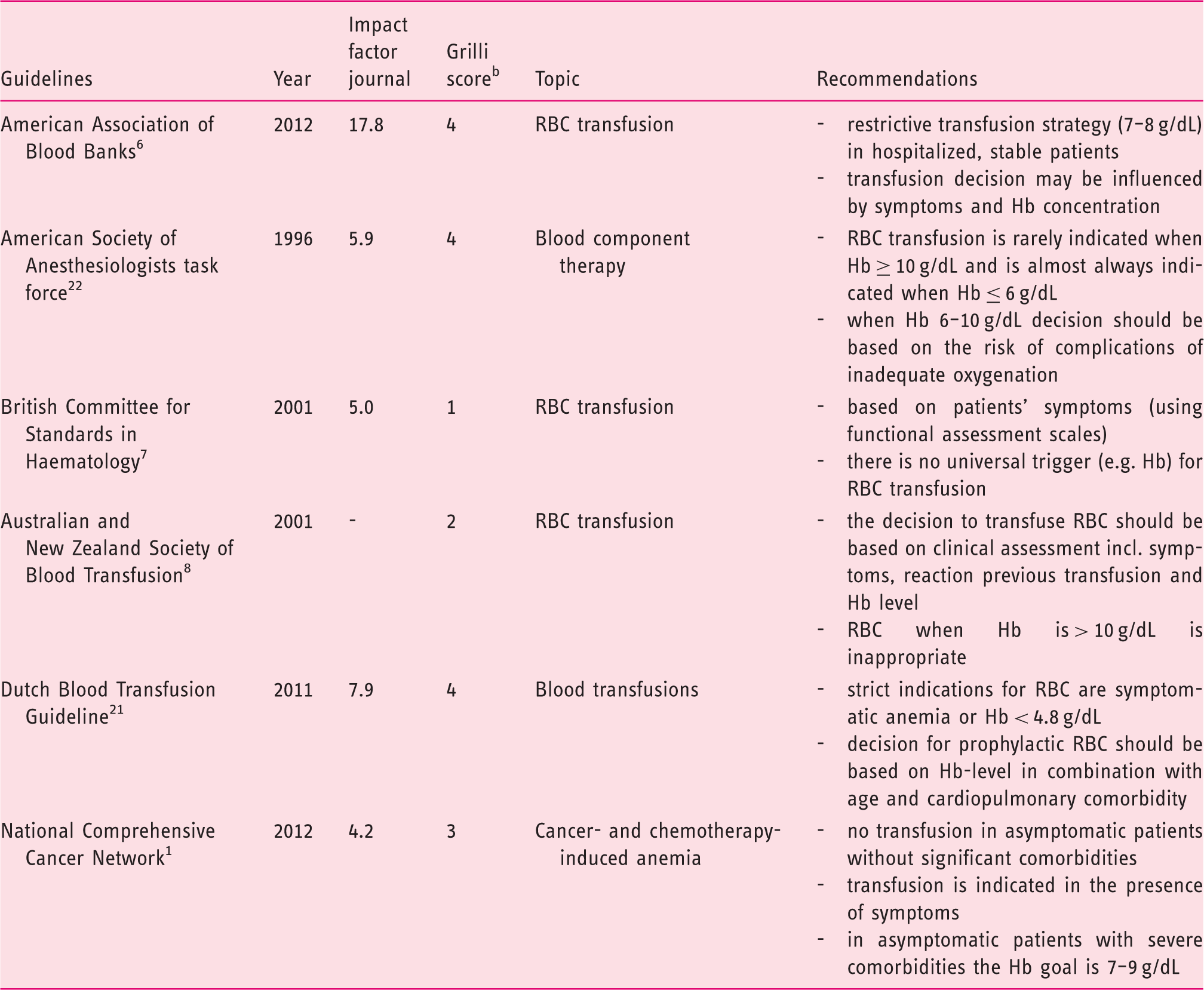
RBC, red blood cell; Hb, hemoglobin; incl., including.
Guidelines addressing perioperative care, critically ill patients or children are excluded.
Grilli score: quality assessment tool for guidelines addressing three topics: description of the involved professionals, description of the sources of information, and explicit grading of evidence. Score range: 0–4.
The present study comes with limitations. First, we determined the clinical factors and the corresponding levels used in this ACBC analysis technique by using the guidelines and pilot testing for comprehensibility. However, there may be unidentified factors that influence the decision-making process. For example, our survey did not offer parenteral iron supplementation as an option to treat anemia. In daily clinical practice RBC transfusion can be preceded by parenteral iron. This may increase the likelihood of measurement error, which could have led to a higher inflection point of Hb for RBC transfusion than in real life. Second, there is a risk of response bias due to the relatively low response rate (29%). We do not know the specific reasons for non-response, but to assess if there are systematic differences we compared respectively characteristics of responders and members of the Dutch Association of Gastroenterologists. Sex (76% vs. 71% men), experience (13 vs. 13 years as a consultant), and type of hospital (academic 21 vs. 22%, teaching hospital 49 vs.39%) are comparable between the two groups, which lowers the chance of a large non-response bias in this study. Moreover, the response rate in our study is comparable to other surveys. 23
As this study is designed to get insight in the decision-making process, we can only speculate about the underlying causes for the discrepancy with guidelines. Further research should be performed to investigate the causes of non-adherence. This is study however is the first step in understanding the decision-making. This is important to instigate the debate about the correct use of RBC transfusion, which eventually should lead to strategies to improve guideline awareness and adherence. Ultimately, this might decrease the undertreatment and overtreatment of chronic anemia with an improvement of clinical outcomes and quality of life.
To conclude, absolute Hb level trumps all other factors as the most important trigger to RBC transfusion decision-making. Current transfusion guidelines address the importance of other factors like the presence of symptoms.1,6,7,8,21 This discrepancy might reflect a lack of awareness of these guidelines by gastroenterologists.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.