
Abstract
Background and aim
Scanty data about inter-observer agreement (IOA) among pathologists in the evaluation of pancreatic samples acquired with EUS histology needle are available. The aim of this study was to determine IOA on adequacy of pancreatic histology specimens obtained with a 22G needle by a panel of experienced pathologist, in comparison with the 19G needle.
Methods
This multicentre prospective study involved 73 pancreatic specimens prepared using histology needles of different calibres. Five pathologists independently reviewed all the samples, assessing the presence of a core, specimen adequacy and the possibility to perform additional analyses. IOA determined by Fleiss’ Kappa statistic was used as the primary outcome measure. Secondary outcome was to compare 22G versus 19G needle results.
Results
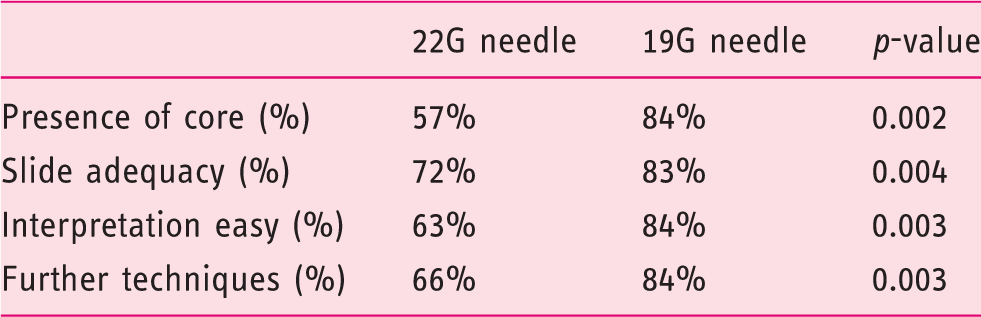
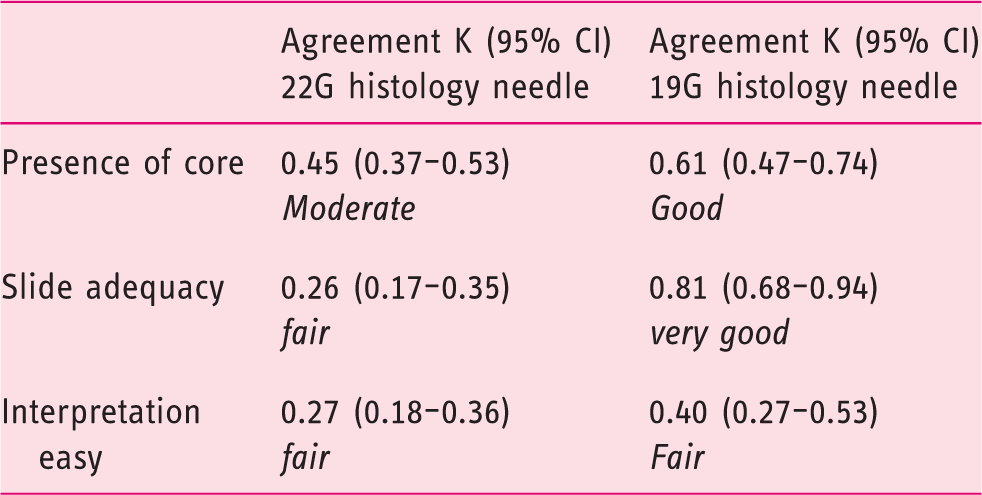
A core was present in 57% of pancreatic specimens obtained by 22G needle. The specimens were considered adequate in 72% of cases, with poor agreement among pathologists (p = 0.02, Fleiss’ κ = 0.26). The possibility to perform further analyses was rated as ‘positive’ in 66% of cases without significant difference among observers (p = 0.80). When comparing the results, the presence of a core and the adequacy of tissue slides were significantly better for the 19G needle (57% vs. 84% p = 0.002; 72% vs. 83% p = 0.004, respectively). Reproducibility in the assessment of pancreatic sample adequacy was significantly better with the 19G needle (κ = 0.26 for 22G samples vs. κ = 0.81 for 19G samples).
Conclusions
Our results suggest that histology sampling of pancreatic masses should be performed with a 19G histology needle, since is able to provide a core in the majority of cases, with 83% of adequate specimens and excellent results in term of reproducibility among pathologists.
Keywords
Introduction
Pancreatic ductal adenocarcinoma is the fifth leading cause of cancer-related death in Europe 1 and has a dismal survival rate even after radical surgery and adjuvant chemotherapy. 2 Endoscopic ultrasound fine-needle aspiration (EUS-FNA) is the procedure of choice to sample pancreatic masses, with an overall sensitivity of almost 85% and specificity of 94%. 3 Cytological study of samples obtained by EUS-FNA allows for recognition of clear signs of malignant transformation such as anisonucleosis, nuclear membrane irregularity and nuclear enlargement. However, in the presence of a high stromal content, tissue architecture is lost and certain types of tumour are difficult to diagnose.4,5
In an attempt to overcome the limitations of EUS-FNA, preserve tissue architecture and improve sample adequacy and diagnostic accuracy, different types of needles have been proposed. Among these, core biopsy needles of different calibres have been presented, showing very promising results in terms of histology core adequacy. A multicentre prospective study assessed the feasibility and diagnostic accuracy of a new 19G core biopsy needle (ProCore needle, Cook Endoscopy Inc, Limerick, Ireland), reporting an easy and reliable way of obtaining histological samples of both pancreatic and non-pancreatic lesions with an overall accuracy of 86% with only one needle pass. 6 A further investigation on these samples was performed to evaluate the inter-observer agreement among gastrointestinal pathologists in grading the quality of specimens. 7 Considering pancreatic masses, the agreement among pathologists on the presence of the core and sample adequacy was almost perfect (Fleiss’ κ = 0.81; 95% CI 0.68–0.94). Pancreatic specimens obtained from stomach and bulb were qualitatively better than those achieved from the second part of the duodenum. Indeed, the use of 19G needles is sometimes hampered when lesions in the pancreatic head region are punctured from the second portion of the duodenum. Therefore, a smaller-sized, more flexible 22G core biopsy needle (ProCore needle, Cook Endoscopy Inc, Limerick, Ireland) has been developed. A multicentre prospective study demonstrated that, for solid pancreatic masses, the overall accuracy of a 22G EUS-FNB needle was adequate in 88.5% of cases. 8 However, data on the inter-observer agreement among pathologists evaluating samples acquired with the 22G core needle have not been reported yet. The aim of this study was to determine the inter-observer agreement on the quality of pancreatic specimens obtained with a 22G ProCore needle by a panel of experienced gastrointestinal pathologists, in comparison with the 19G ProCore needle.
Materials and methods
Study design
This multicentre study involved five experienced pathologist (CD, KB, GM, IA and GR) from European academic referral centres (Marseille, France; Milan and Rome, Italy; Rotterdam, the Netherlands and Santiago de Compostela, Spain) to examine pancreatic specimens obtained with both 22G and 19G core biopsy needles. The pathologist team was the same involved in the previous agreement study. The study was approved by each local institutional review board.
Each pathologist contributed sample materials from 10 consecutive patients obtained with 19G and 10 with 22G needles. In the evaluation sequence, all 19G slides were evaluated first, and subsequently those obtained by 22G. Each pathologist contributed with the best diagnostic slide selected from each patient. Pathologists were blinded to the final diagnosis and were asked to evaluate the presence of a tissue core and independently assess the following features: adequacy and interpretability of specimen, and possibility to perform further analyses such as immunohistochemistry and fluorescence in-situ hybridization.
The adequacy of the specimen for diagnosis was defined as the clear presence of target organ cells to guarantee an accurate diagnosis. The interpretation of each specimen was judged as ‘easy’ or ‘not easy’, taking into consideration the percentage of pathological tissue on each slide. For quantitative assessment, three different classes were recognized: ≤50% of pathological tissue (class 0), >50% and ≤70% (class 1), and >70% (class 2). The possibility to perform further analyses as described above was scored as ‘positive’ or ‘negative’ based on the quantitative assessment of malignant cells, at the pathologist’s discretion.
All pathologists simultaneously observed each specimen at the microscope and independently rated it. A structured, predefined worksheet was provided to record all relevant data. Final data analysis was performed by MCP (endosonographer) and MB (epidemiologist), who were not involved in the evaluation and interpretation of the pathology slides.
EUS technique and specimen processing
Between March and July 2010, 19G ProCore needles were used in consecutive patients referred for EUS-guided tissue acquisition to evaluate intra-intestinal or extra-intestinal mass lesions and/or peri-intestinal lymph nodes, 6 while between September and December 2010 22G ProCore needles were used to evaluate solid pancreatic masses. 8 Therefore, all specimens obtained with 22G needle and included in this study were pancreatic. EUS-guided fine-needle biopsy (FNB) was performed using a linear convex array echoendoscope (Pentax EG-3870UTK or Olympus UCT-140/180). All procedures were performed by experienced endosonographers, and only one pass was done during the procedure according to a standardized study protocol. Tissue samples were acquired according to the same standard protocol by all centres involved in the study: after endosonographic visualization of the target lesion and scanning for blood vessels by colour and pulsed Doppler, the fine-needle biopsy with a 19G or 22G ProCore needle was performed from either the duodenum, stomach or oesophagus, depending on location of the lesion. Once inside the lesion, the stylet was removed and suction was applied with a 10 ml syringe. The needle was kept still for approximately 10 s, after which it was moved to and fro within the lesion three times. Suction was released before needle removal. Tissue samples were recovered according to each centre’s protocol in CytoLyt and/or formalin by flushing the needle with 5 ml of saline solution. All samples were processed at the pathology departments for histological analysis and assessed by a dedicated pathologist with a special interest in evaluating tissue materials obtained via EUS. Samples were embedded in paraffin and tissue sections of 3–4 µm were stained with haematoxylin and eosin for morphological evaluation. If pathologists were not able to obtain a core for histological evaluation, they processed the same material as cell-block for cytological evaluation.
Statistics
The results obtained from different centres were compared using Pearson’s chi-square test to evaluate possible systematic differences. Inter-observer agreement was determined by kappa statistics (Fleiss’ κ-statistic and 95% confidence intervals (CIs)). κ-Statistics are widely used and accepted coefficients that provide a measure of observer agreement, accounting for agreement other than that which occurs by chance alone. κ-Statistics were interpreted according to the convention of Landis and Koch:
9
<0, no agreement; 0–0.20, slight agreement; 0.21–0.40, fair agreement; 0.41–0.60, moderate agreement; 0.61–0.80, substantial agreement; and 0.81–1.0, almost perfect agreement. Statistical significance was established as p < 0.05 (two-tailed). All analyses were carried out using
Results
A total of 100 cases were reviewed by five experienced pathologists. All specimens obtained with 22G FNB (50) were from pancreatic lesions, while among 50 specimens obtained with 19G needles 23 were from pancreas, while the remaining 27 were from other organs and for this reason not included in the analysis.
The simultaneous analysis of pancreatic specimens obtained with a 22G needle revealed that the presence of a tissue core was observed in 57% of cases, with moderate agreement among pathologists (κ = 0.45; 95% CI 0.47–0.74). The percentage of slides with a core did not differ across observers (p = 0.26).
The specimens were considered adequate in 72% of cases, with poor agreement among pathologists (p = 0.02, κ = 0.26; 95% CI 0.68–0.94). The interpretation of specimens was reported as ‘easy’ in approximately 63% of cases, with poor agreement among pathologists (κ = 0.27; 95% CI 0.17–0.35). The possibility to perform further analyses was rated as ‘positive’ in approximately 66% of cases without significant difference among observers (p = 0.80). Considering the amount of pathological tissue that was present in the slides, 48% of samples presented ≤50% of pathological tissue and were included in class 0, 38% had >50% and ≤70% of pathological tissue and were included in class 1, and 4% had more than 70% of pathological tissue and were included in class 2.
Rates for tissue cores, sample adequacy, interpretation and additional techniques of pancreatic specimens obtained with 19G and 22G needles.
Reproducibility among pathologists in the assessment of pancreatic sample quality (κ-statistics).
Discussion
In this multicentre prospective study we compared pancreatic histological specimens obtained with two EUS histology needles of different calibres (19G and 22G), evaluating the inter-observer agreement among expert pathologists. It is noteworthy that the histological specimens were obtained by a single pass. Our results showed that using a core needle it is possible to obtain from 72% to 83% specimen adequacy by a single pass. Furthermore, the presence of the core, sample adequacy, sample interpretation and the possibility to perform further analyses on the same material were significantly better for samples obtained using the 19G needle than for those obtained using the 22G needle. In a previous study, we demonstrated that the adequacy of tissue specimens significantly improved when the percentage of pathological tissue increased. 8 In this study core tissue was observed in 57% of specimens obtained with a 22G needle and in 84% of samples obtained with a 19G needle. Therefore, the larger calibre needle seems to offer a better opportunity to achieve adequate samples, and subsequently a correct diagnosis is probably more likely. These results are consistent with a recent prospective randomized study comparing the diagnostic accuracy of two EUS-FNA needles, 19G and 22G, without ROSE in patients with solid pancreatic masses. Per-protocol analysis showed that the diagnostic accuracy of a 19G FNA needle was significantly higher than that of a 22G FNA needle. 10 Although 19G needles offer a better diagnostic yield, ESGE guidelines recommend against using 19G needles for transduodenal biopsy because of the higher rate of technical failures in the case of lesions that need to be punctured from the duodenum. 11 However, this aspect has not been evaluated in our study, since it was based exclusively on pancreatic specimens that we received from each pathology department.
Our results highlight that performing EUS-FNB with a 19G needle improves both tissue acquisition and sample adequacy. Indeed, the cellular architecture of specimens is better preserved in the 19G FNB specimens, with excellent results in terms of inter-observer agreement (κ = 0.81). Pathologists agreed in evaluating sample adequacy obtained using the 19G needle, while agreement was only fair (κ = 0.26) when 22G pancreatic samples were evaluated.
The possibility to perform additional analyses was rated as positive in approximately 84% of samples obtained with the 19G needle, significantly more than with the use of the 22G needle (66%). Indeed, in the dawning era of individualized medicine, a tissue core biopsy is able to provide information that may facilitate personalized treatment of cancer: our results indicate that pancreatic samples obtained with the 19G needle are more suitable for this purpose.
This study has some limitations. First, the pathologists were not blinded regarding the size of the needle evaluated. Second, each component of the team was academic pathologist, highly experienced in the assessment of EUS specimens from the gastrointestinal tract, and it has been demonstrated that the level of agreement between expert pathologists is usually higher than that of pathologists working in, for example, community hospitals. Third, the EUS-FNB protocol used to produce biopsies was standardized among participating centres, whereas in clinical practice this may differ. It remains to be confirmed that major or minor technical variations in the acquisition and tissue-processing procedure do not affect the quality and outcome of the assessment of EUS-FNB samples. Therefore, further studies are needed to verify the feasibility of EUS-FNB to analyse pancreatic lesions in everyday practice. Last, the study aimed to evaluate the agreement among pathologists on the quality of samples, and was not designed to assess the clinical diagnostic value of EUS-FNB. This is emphasized by a recent study that seems to suggest that the improved ability of EUS-FNB needles to obtain an adequate tissue core does not translate into an accurate pre-operative grading when compared with the final resected specimen. 12
In summary, our results suggest that sample acquisition of pancreatic masses should be performed with a larger diameter 19G EUS-FNB needle, since it is able to provide a sample for histological examination in the majority of cases (84%), with 83% of adequate specimens and excellent results in term of reproducibility among pathologists.
Further advances in needle technology are required to improve needle flexibility and facilitate the use of a large calibre needles in difficult anatomical situations such as the duodenum.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.