
Abstract
Background
We investigated, for the first time, levels of compliance with faecal calprotectin test in inflammatory bowel disease patients.
Methods
All consecutive adult inflammatory bowel disease patients having been prescribed an faecal calprotectin test between December 2014–July 2015 were included. At their next visit to the hospital, patients had to return a stool sample for the faecal calprotectin test and answer a simple questionnaire: ‘Have you brought a stool sample? If not, why not? If so, did you encounter any difficulties when collecting the sample? Were you aware of faecal calprotectin before being asked to take the test?'.
Results
One hundred and one patients were included (50 men; 77 patients with Crohn’s disease). The range age was 40 years (19–68). Eighty-nine patients were being treated with infliximab, 10 were on vedolizumab, and two were not being treated with a biologic. Thirty-seven patients (35%) had performed the faecal calprotectin test. Eighty-one patients (80%) had not been aware of faecal calprotectin before being asked to take the test. Of the 64 patients who did not take the test, the prime reasons for non-compliance were forgetfulness (n = 49, 76.6%), a lack of perceived benefit for the test (n = 7, 11%), constipation (n = 5, 7.8%), refusal to handle faeces (n = 2, 3.1%), and difficulty collecting the stool sample (n = 1, 1.5%).
Conclusion
Only one-third of the patients performed the faecal calprotectin test. The main reason for non-compliance was forgetfulness. Our present results emphasise the need for better patient education on the importance of complying with faecal calprotectin testing and the future of faecal calprotectin testing at home.
Introduction
Inflammatory bowel disease (IBD) encompasses a number of disabling, chronic, inflammatory conditions. 1 Mucosal healing is a major therapeutic goal in IBD, 2 and has been associated with lower rates of relapse, hospitalisation and surgery.3–6 At present, the management of IBD is based on ‘treat-to-target’ strategies, with regular assessments of disease activity (using validated outcome measures) and a subsequent adjustment of treatment if persistent inflammatory activity is detected. 7 Direct endoscopic assessment of mucosal inflammation is the current gold standard. 8 However, this procedure is relatively invasive, time-consuming and costly; furthermore, endoscopy is associated with patient discomfort and is not risk-free.9–11 A number of faecal markers can potentially be used to (a) differentiate between quiescent and active disease states, (b) assess mucosal healing or (c) predict the response to therapy.12–15 The two most commonly used markers are faecal calprotectin (FC) and lactoferrin. 16 FC is a calcium-binding protein that accounts for approximately 60% of the cytosolic protein in neutrophils. 17 Given that FC is stable in faeces, it can be used as a marker for neutrophil infiltration of gastrointestinal tissues and thus gut inflammation. 18 FC is considered to be the most accurate non-invasive marker for monitoring mucosal healing in IBD.19–27 Compliance with this test is essential if the patient is to benefit from the results. However, some patients may forget or be reluctant to perform this test.28,29 Furthermore, regular monitoring is a major issue in chronic diseases like IBD.30,31 Hence, the present study sought to (a) investigate for the first time compliance with the FC test in a population of IBD patients and (b) identify factors associated with non-compliance.
Methods
Study design
A prospective observational study was performed at Nancy University Hospital (Nancy, France) between December 2014–July 2015. A FC test was prescribed to all consecutive adult patients in the Nancy IBD cohort as part of our department’s standard care for IBD. It is the reason why we included only patients coming to our infusion clinic. The Nancy IBD cohort has been registered with the French National Data Protection Commission (Commission Nationale de l’Informatique et des Libertés; reference: N81404720). All patients had Crohn's disease (CD) or ulcerative colitis (UC). The patients’ demographic and clinical characteristics were recorded. All patients received written information on the FC test’s purpose and procedure (as in our routine practice). Patients were asked to return a stool sample at the time of their next infliximab or vedolizumab infusion and to complete a short questionnaire: ‘Have you brought a stool sample to this consultation? If not, why not? If so, did you encounter any difficulties when collecting the sample? Were you aware of FC before being asked to take the test?'.
Lastly, we recorded each patient’s serum C-reactive protein (CRP) level.
Statistical analyses
Categorical variables were quoted as the number (percentage), and continuous variables were quoted as the mean ± standard deviation (range). Factors associated with compliance with the FC test were identified in bivariate logistic regression analyses. A multivariable logistic regression model was then computed using candidate variables with a p-value<0.2 in the bivariate analysis. A stepwise procedure was applied, with a significance-level-to-enter <0.2 and significance-level-to-stay <0.05. The strength of association was estimated by calculating the crude and adjusted odds ratios (ORs) (95% confidence interval (CI)). The alpha risk was set to p < 0.05. All analyses were performed using SAS software (version 9.4, SAS Institute Inc., Cary, North Carolina, USA).
Results
Study population
Baseline characteristics of the study population (n = 101).
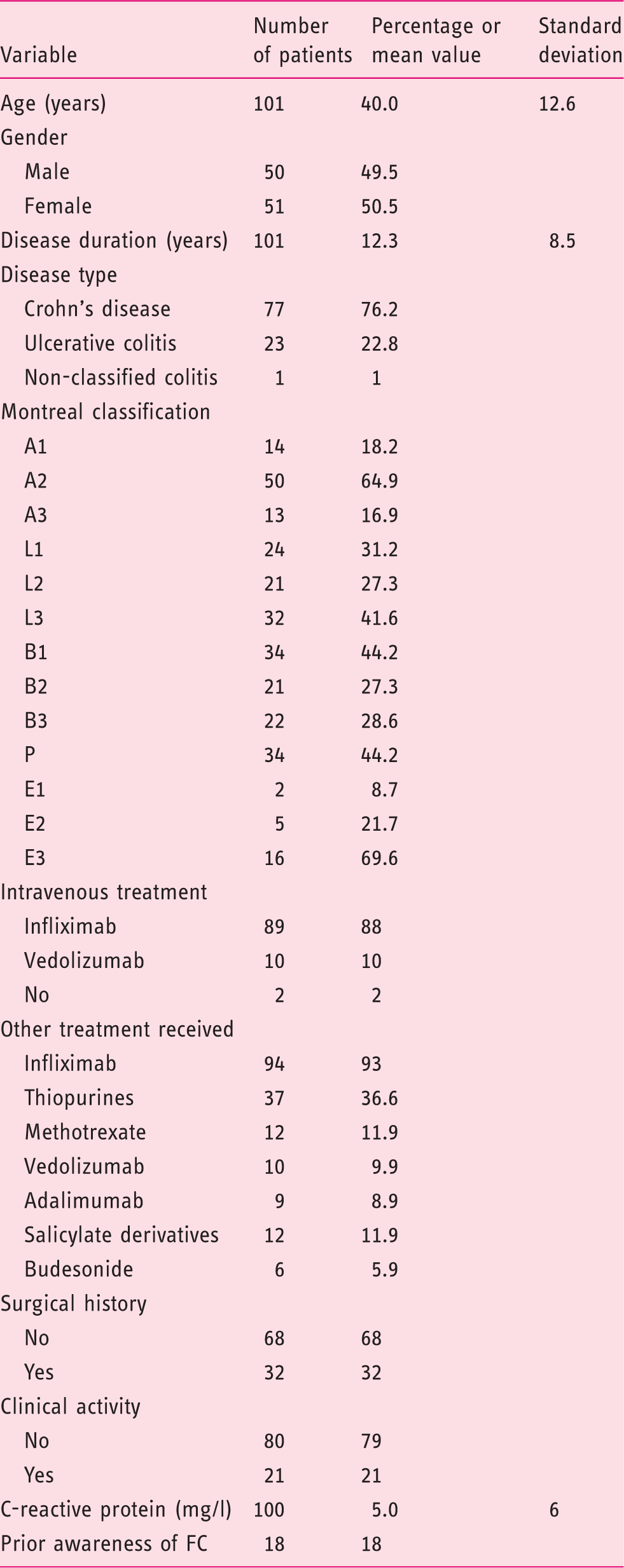
FC: faecal calprotectin.
Compliance with the FC test, and clinical factors associated with compliance/non-compliance
Thirty-seven of the 101 patients (36%) brought a stool sample to the next consultation. None of these patients reported difficulty in collecting a stool sample for the FC test.
Factors associated with compliance with the faecal calprotectin (FC) test (bivariate analyses).

CI: confidence interval; OR: odds ratio.
After applying stepwise selection in a multivariate analysis, stricturing behaviour was the only factor significantly associated with compliance with the FC test (OR (95% CI) = 4.3 (1.3–14); p = 0.03).
Gender, disease type, clinical activity, a history of surgery and other previous treatments were not associated with compliance.
Reasons for non-compliance with FC test
The prime reasons for not bringing back the stool sample (n = 64) were as follows (Figure 1). Forgetfulness was reported by 49 patients (76.6%), six patients (11%) did not consider that the FC test was of value, five patients (7.8%) reported constipation, two (3.1%) refused to handle stools, and one patient (1.5%) reported difficulty in collecting a stool sample.
Reasons for non-compliance with faecal calprotectin (FC) test.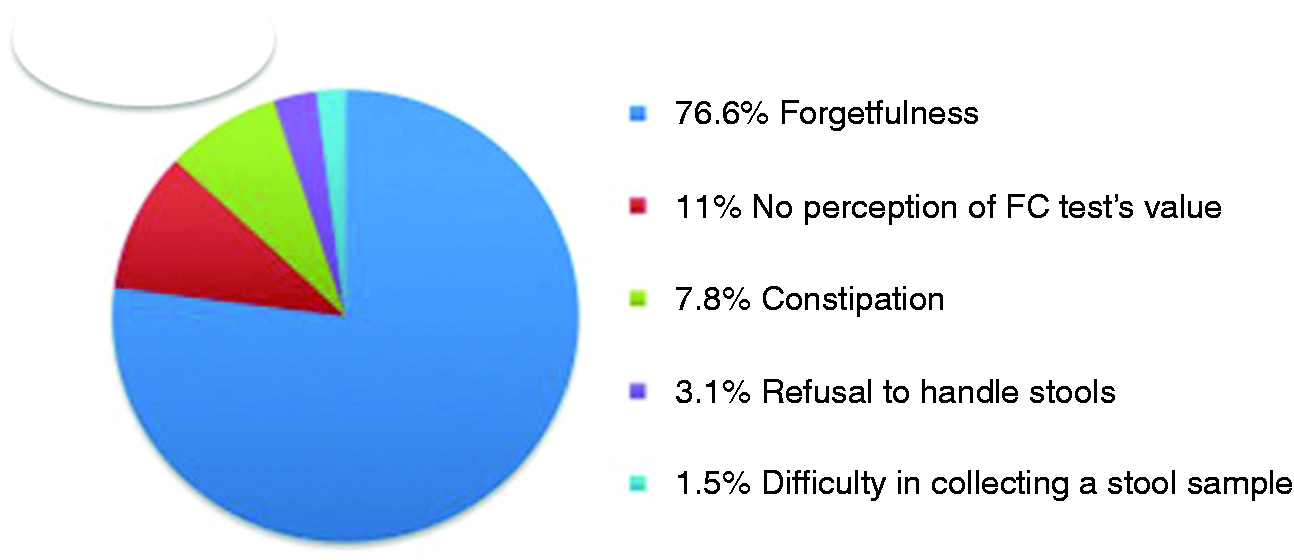
Discussion
This is the first study to have investigated compliance with the FC test in patients with IBD. We found that only one-third of the patients complied with this test.
Treatment adherence is acknowledged to be a major therapeutic goal in chronic disorders such as hypertension 32 and diabetes. 33 However, rates of compliance with long-term treatments are far from optimal, with an average value of 50%. 34 Sub-optimal treatment compliance has been also reported in immune-mediated inflammatory diseases (IMIDs). In IBD, treatment compliance rates range from 7–72%. 35 A systematic review of 73 studies 31 has assessed the factors associated with non-compliance with treatment for IMIDs. As in the present study, few studies 31 found an association between compliance on the one hand and demographic factors, disease activity and disease duration on the other. In terms of treatment-related factors, greater compliance was observed in patients receiving tumor necrosis factor (TNF) antagonists. 31 In the present study, compliance was worse in patients on infliximab compared to patients on vedolizumab. However, this result was barely significant, given that only 10 patients were being treated with vedolizumab. Moreover, this factor was not statistically significant in a multivariate analysis. We also found that previous or ongoing treatment with vedolizumab was associated with better compliance. We hypothesised that vedolizumab-treated patients were more compliant because their disease was more likely to be resistant to conventional treatments. 36 Moreover, vedolizumab-treated patients have often undergone many endoscopic assessments and have a better understanding of the value of FC as a non-invasive marker. A systematic review reported that practical factors (such as travelling, busy lifestyles and forgetfulness) had an impact on treatment compliance. 31 In the present study, the main reason for non-compliance was forgetfulness. Our patients were seen every month or every two months in our IBD infusion clinic; we hypothesise that compliance would be even worse in patients seen every three or six months. Home testing might improve compliance, and the latest rapid FC tests have much the same diagnostic performance as conventional enzyme-linked immunosorbent assays (ELISA) values. 37 Self-monitoring could improve compliance with IBD medications, just as home blood pressure monitoring is associated with better compliance with anti-hypertensive medications in hypertensive patients.32,38
It is important to find ways of improving the observed, poor compliance with the FC test. A systematic review 39 has sought to identify the most suitable interventions for improving treatment compliance in patients with IMIDs. Although patient education alone had no effect on compliance rates, multicomponent interventions did have a significant association with compliance. 39 In the present study, prior awareness of FC was not associated with better compliance. If patient education alone is not sufficient, it could be combined with further information related to the patient’s beliefs, practical problems with the test, and greater encouragement to perform the test. Text-message-based reminders might also be of value.
The compliance rate for colorectal cancer screening is around 30%,40,41 which is similar to the value observed in this study for the FC test. These results indicated that compliance with a faecal test is a major issue. Poor patient awareness and a lack of advice from physician are both factors associated with poor compliance. 40 Compliance with the FC test might be better if more information was provided by the physician prescribing the test.
The main strength of the present study was its prospective design. However, the study also had some limitations. Firstly, it was a single-centre study. Secondly, all but two of the patients were being treated with a biologic in a day hospital. Thirdly, the number of included patients was relatively small, and the statistical power of the multivariate model may have been too low to highlight other significant associations with FC compliance.
In conclusion, the current treatment strategy in IBD (based upon the regular assessment of disease activity and then treatment adjustment) requires repeated testing for non-invasive markers (such as FC). However, we found that only one-third of patients complied with this test. Multicomponent patient education might increase compliance rates. Home testing is probably of value in IBD monitoring.
Footnotes
Declaration of conflicting interests
LPB: consulting fees from Merck, Abbvie, Janssen, Genentech, Mitsubishi, Ferring, Norgine, Tillots, Vifor, Therakos, Pharmacosmos, Pilège, BMS, UCB-pharma, Hospira, Celltrion, Takeda, Biogaran, Boerhinger-Ingelheim, Lilly, Pfizer, HAC-Pharma, Index Pharmaceuticals, Amgen, Sandoz and Forward Pharma GmbH. Lecture fees from Merck, Abbvie, Takeda, Janssen, Ferring, Norgine, Tillots, Vifor, Therakos, Mitsubishi and HAC-Pharma. The others authors declare no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.