
Abstract
Background
Pain has been associated with fatigue in many chronic diseases, but data are not available for inflammatory bowel disease (IBD). The aim of this study was to investigate whether fatigue is associated with pain in IBD after adjusting for the relevant covariates.
Methods
Participants were recruited from nine hospitals in the south-eastern and western part of Norway. Socio-demographic variables were self-reported by patients. Disease activity was assessed by disease activity indices and faecal calprotectin. Patient-reported outcomes (PROs) were collected using the Fatigue Questionnaire (FQ), Brief Pain Inventory (BPI), Hospital Anxiety and Depression Scale (HADS) and Basic Nordic Sleep Questionnaire.
Results
From a total of 452 invited patients, 414 (91.6%) provided written informed consent. After excluding any missing data, 408 total patients were included in the analyses (ulcerative colitis = 180 and Crohn’s disease = 228). In the crude analysis, substantial and chronic fatigue were associated with increased pain intensity regardless of the diagnosis. However, when controlling for relevant covariates in the ANCOVA, the differences in pain intensity among patients with and without substantial or chronic fatigue were insignificant. The Cohen’s d effect size was small to moderate (>0.20) in patients with chronic fatigue.
Conclusions
Despite a tendency of elevated pain intensity scores among patients with fatigue, these differences were insignificant after controlling for the relevant covariates. However, based on Cohen’s effect size, these differences may be of clinical importance in a subset of patients.
Introduction
Inflammatory bowel disease (IBD) consists of ulcerative colitis (UC) and Crohn’s disease (CD) and is characterised by chronic, recurrent inflammation of the gastrointestinal (GI) tract. 1 In UC, the inflammation is located in the colonic and rectal mucosa, whereas in CD, any part of the GI tract may be affected. Common IBD symptoms include abdominal pain, tenesmus and diarrhoea, either with or without blood, pus and mucus. 2
Fatigue is a frequently reported symptom in patients with IBD. 3 Several definitions of fatigue exist, which indicates a lack of consensus. However, the recent literature defines fatigue as, ‘an overwhelming, debilitating, and sustained sense of exhaustion that decreases one’s ability to carry out daily activities, including the ability to work effectively and to function at one’s usual level in family and social roles’. 4 In most cases, fatigue is influenced by disease activity, but studies have also revealed that these symptoms are prevalent even when patients are deemed to be in remission.5–8 Prior studies also revealed that factors such as anxiety, depression and decreased levels of haemoglobin are associated with increased fatigue. 3 Fatigue is viewed by IBD patients as one of their most burdensome symptoms, and it is associated with increased worry and impaired health-related quality of life (HRQoL).9–12 In addition, there are reports of a gap between health care personnel’s knowledge and understanding of the complexity of fatigue and the impact that these symptoms have on IBD. 13
In addition to fatigue, pain is one major symptom that occurs in IBD. 14 The latter is related not only to abdominal discomfort, which is caused by inflammation or strictures with subsequent bowel distension, but also non-inflammatory joint pain and pain caused by arthritis. 15 In other chronic illnesses, such as rheumatoid arthritis (RA) and multiple sclerosis (MS), increased pain has been associated with more fatigue.16,17 Although an association between pain and fatigue has been demonstrated in other patient populations, no such data are available for IBD. Based on input from members of the Norwegian Crohn’s and Colitis Association, we hypothesised that pain might also be a potential unexplored factor of importance for fatigue symptoms in IBD. Investigating the potential association between fatigue and pain in IBD may be helpful in planning how to manage or alleviate fatigue among these patients.
Consequently, the primary aim of this study was to investigate whether fatigue symptoms are associated with increased pain in IBD. The secondary aim was to investigate whether controlling for disease activity, depression and sleep problems could influence these scores.
Materials and methods
Participants were recruited from IBD outpatient clinics at nine hospitals in the south-eastern and western part of Norway from March 2013 to April 2014. The inclusion criteria were: >17 years of age, a verified diagnosis of IBD (based on endoscopic, laboratory and histological findings, i.e. the Lennard-Jones criteria), 18 the ability to read Norwegian, and written informed consent.
Data collection
After patients had consented to participate in the study, a standardised inclusion procedure was followed at each centre. This allowed clinical, socio-demographic, questionnaire and laboratory data to be collected at the hospital during inclusion.
While the socio-demographic variables included age, gender, smoking status, and marital and educational status, the disease activity was assessed by the Simple Clinical Colitis Activity Index (SCCAI) and the Simplified Crohn’s Disease Activity Index (SCDAI).19,20 To measure faecal calprotectin, stool samples were delivered in person at the outpatient clinic and sent by mail to Gas-Cal-Lab©, Oslo University Hospital, where they were stored at −20℃ until ready for extraction (Roche Diagnostics GmbH®). The phenotypic classification was conducted according to the Montreal classification.
Questionnaires
The Fatigue Questionnaire (FQ)
The FQ was developed by Chalder et al. 21 and has been previously validated in several settings including IBD.7,22 The scale scores of the FQ were scored on a dichotomised scale (0 = better than usual and no more than usual, 1 = worse than usual and much worse than usual). Based on prior studies and the general consensus, substantial fatigue was defined as a dichotomised FQ score >4, whereas chronic fatigue (CF) was defined as a dichotomised FQ score >4, and in addition, a duration ≥6 months.21,23
The Brief Pain Inventory (BPI)
Developed by Cleeland and Ryan, 24 the BPI was designed to measure (a) the subjective intensity of pain and (b) the impairment caused by pain. The pain intensity section of the BPI consists of four items that are scored from 0 (no pain) to 10 (worst possible pain). A pain severity score is calculated from the mean of the four pain intensity items. 24 Recently, the BPI was evaluated in IBD. 25
Hospital Anxiety and Depression Scale (HADS)
Depression was measured using the depression subscale of the Hospital Anxiety and Depression Scale (HADS). 26 HADS is a self-assessment instrument that is divided into two scales: (A) measuring anxiety and (D) depression. Each scale has seven items that are scored on a four-point Likert scale (0–3); the higher the score, the greater the level of anxiety and depression. The Likert scale has been widely used to describe the prevalence of anxiety and depression in IBD.
Basic Nordic Sleep Questionnaire
Sleep problems were measured using the Basic Nordic Sleep Questionnaire item on sleep quality in the last three months. The item is scored on a five-point Likert scale, where a higher score indicates increased sleep problems. 27
Statistical analyses
To assess patient characteristics, we used descriptive analysis, frequencies and the χ2 test. The means and standard deviations were used to express normally distributed variables, whereas the medians and interquartile range (IQR) were used to express non-normally distributed variables. To investigate potential associations between fatigue and pain, an analysis of variance (ANOVA) was used. To correct the model for relevant covariates hypothesised to influence fatigue and pain, the following factors were entered as covariates in the analysis of covariance (ANCOVA): gender, disease activity index score, C-reactive protein (CRP), haemoglobin, ferritin and calprotectin levels, depression, anxiety and sleep problems. The data on fatigue and pain are presented as: (a) crude scores and (b) scores adjusted for the previously presented factors (estimated marginal means). Cohen’s d was used to calculate clinical significance. 28 Operational definitions of 0.2, 0.5 and 0.8 were categorised as small, medium and large effect sizes, respectively. 28 All of the tests were two sided with a 5% significance level and performed using Predictive Analytics Software (PASW) version 22.0 (SPSS Inc, 233 S. Wacker Drive, Chicago, IL, USA).
Ethics
Participation in the study was based on written informed consent and performed in accordance with the principles of the revised Helsinki Declaration. Approval was obtained from the Regional Ethics Committee (reference number: 2012/845/REK Sør-Øst A).
Results
Socio-demographic and clinical data according to diagnosis.
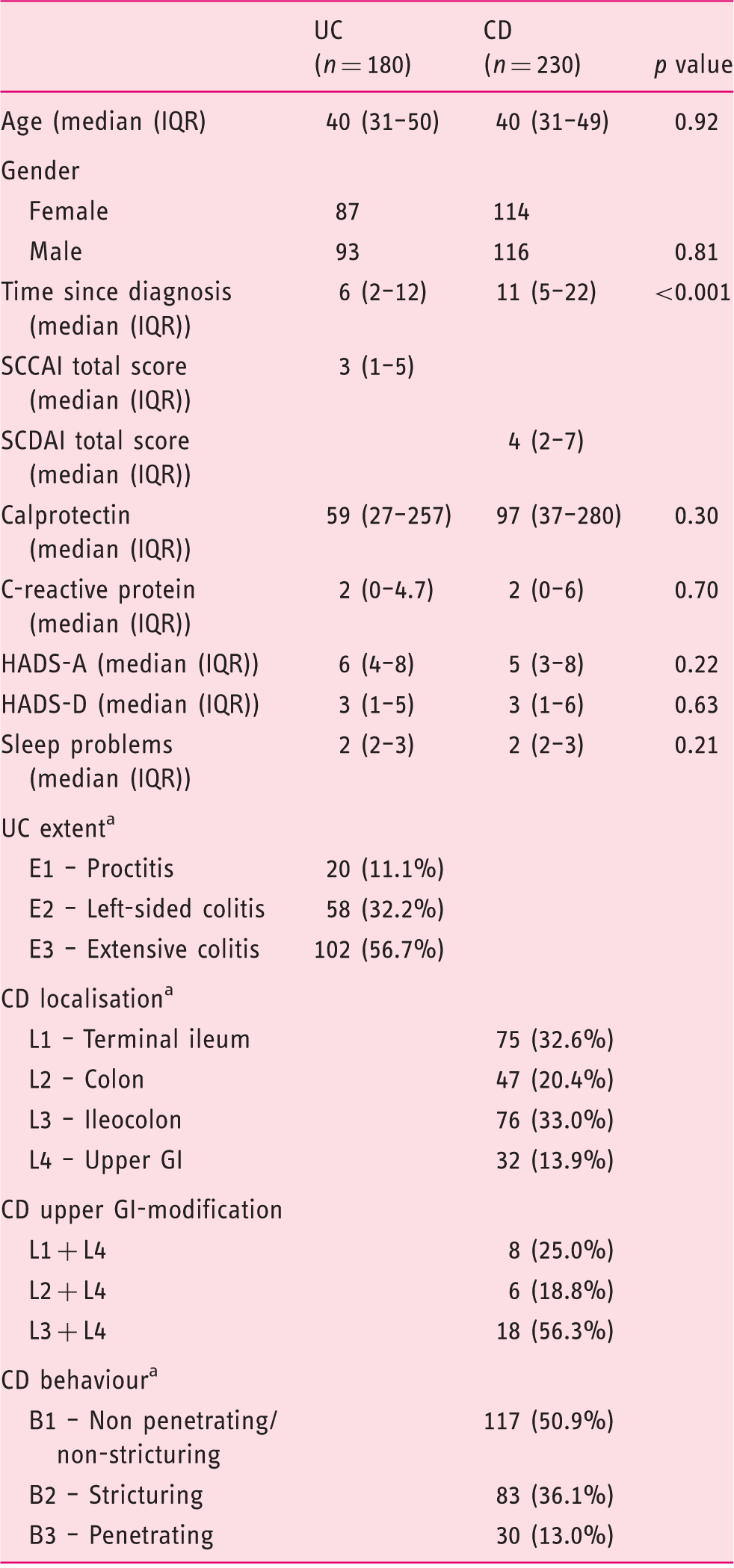
UC: ulcerative colitis; CD: Crohn’s disease; GI: gastrointestinal; SD: standard deviation: IQR: interquartile range; SCCAI: Simple Clinical Colitis Activity Index; HADS: Hospital Anxiety and Depression Scale; SCDAI: Simplified Crohn’s Disease Activity Index, aMontreal Classification. Figures are the mean and standard deviation in brackets if not otherwise noted.
Out of the 408 patients who had evaluable data on both the BPI and FQ, substantial fatigue (SF) was reported in 90/180 (50%) of UC patients and in 104/228 (45.6%) of CD patients. CF was reported in 52/180 (28.9%) of UC patients and in 65/228 (28.5%) of CD patients. There were no statistically significant differences in the occurrence of substantial- or CF between the diagnostic groups.
The anxiety, depression and disease activity index scores were significantly associated with substantial fatigue in UC and substantial as well as CF in CD (Mann Whitney U, p < 0.001). In UC patients, CF was associated with depression and an increased disease activity score (Mann-Whitney U, p < 0.001). A higher level of sleep problems was associated with both substantial and CF, regardless of diagnosis (Mann-Whitney U, p < 0.001). Neither age, nor the levels of haemoglobin, ferritin, CRP or calprotectin were significantly associated with substantial or CF in UC or CD.
A total of 323 out of 408 patients delivered a stool sample for the measurement of faecal calprotectin (79.2%, UC 147/180, CD 176/228). There were no statistically significant differences in calprotectin levels between the diagnostic groups (Table 1). In UC, the correlation between the SCCAI total score and CRP was insignificant, whereas a significant correlation was observed between the SCCAI and calprotectin (0.38, p < 0.001). In CD, the SCDAI total score was not correlated with either CRP or calprotectin.
Fatigue and pain intensity
Crude pain intensity scores among patients reporting substantial (SF) or chronic fatigue (CF).
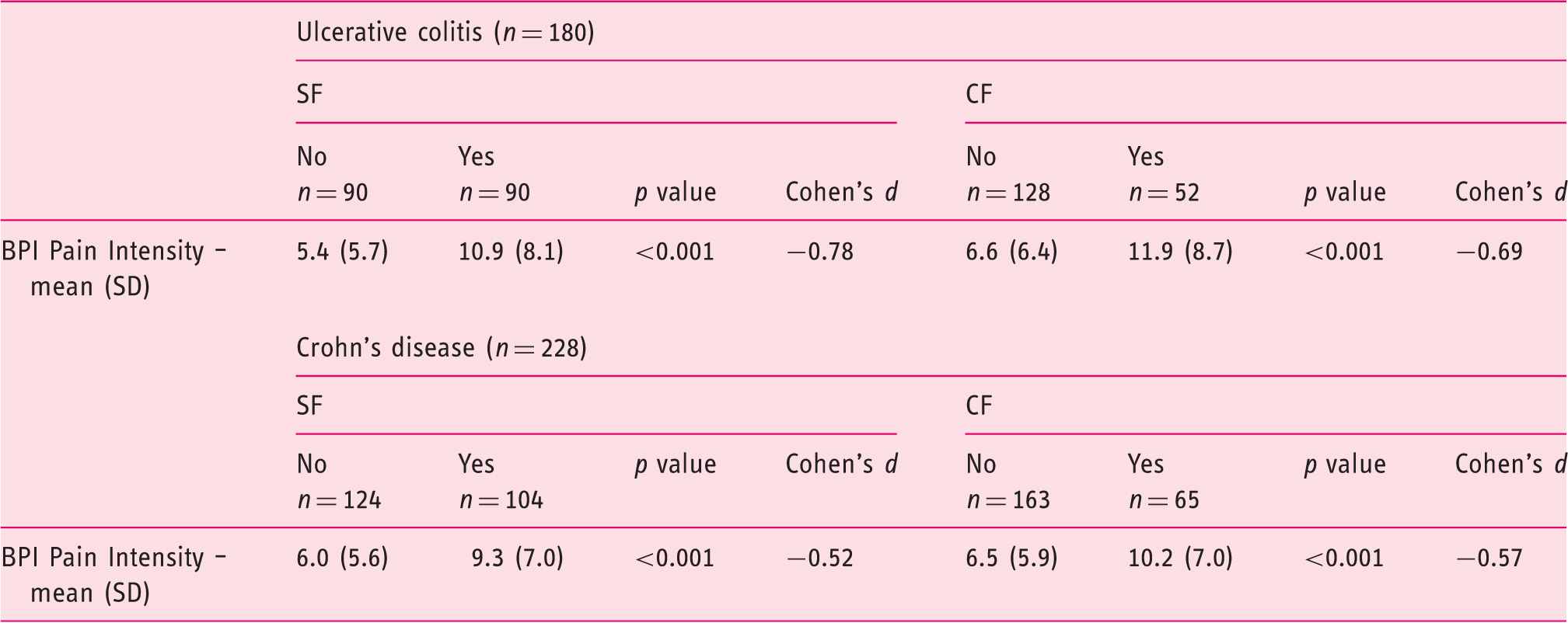
BPI: Brief Pain Inventory; SD: standard deviation, Cohen’s d: operational definitions of 0.2, 0.5 and 0.8 regarded as small, medium and large effect size, respectively.
Pain intensity scores calculated as the estimated marginal means in the analysis of covariance a (ANCOVA). Scores are presented according to the presence of substantial or chronic fatigue.
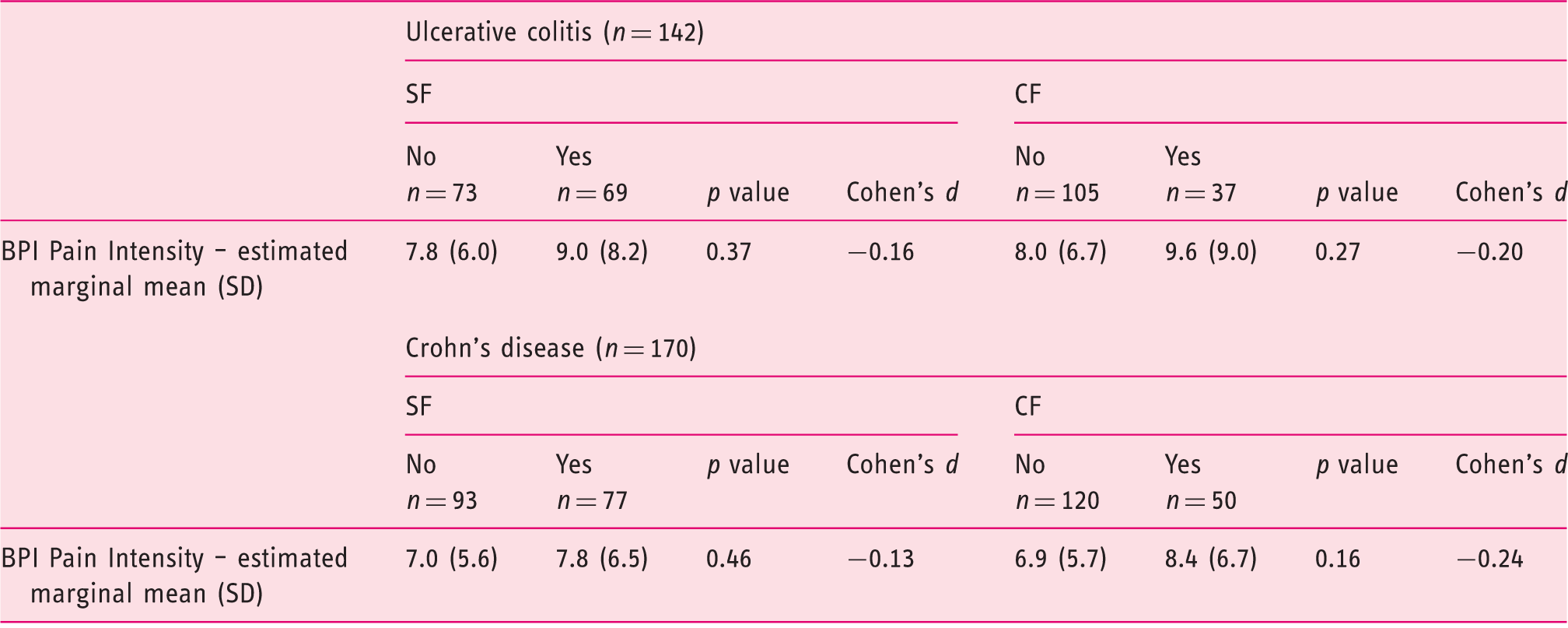
The following covariates appear in the model: age, disease activity index total score, calprotectin, C-reactive protein, ferritin, haemoglobin, sleep problems, HADS anxiety and depression. Only patients with complete data for all parameters included as covariates appear in the model. BPI: Brief Pain Inventory; SD: standard deviation, HADS: Hospital Anxiety and Depression Scale; Cohen’s d: operational definitions of 0.2, 0.5 and 0.8 regarded as small, medium and large effect size, respectively
Calculating Cohen’s d effect size revealed that differences in pain intensity scores were moderate to large in the ANOVA (Table 2). Following ANCOVA, a small effect size remained among patients with CF, regardless of the diagnosis (Table 3).
Discussion
Compared to IBD patients without fatigue, patients with substantial and/or CF had significantly increased pain intensity scores. However, after adjustment for relevant covariates, differences in pain intensity among these patients was insignificant. However, in patients with CF, the effect sizes remained small to moderate.
Until recently, fatigue in IBD was investigated only to a limited extent. However, following a review by van Langenberg and Gibson in 2010, 29 a substantial body of literature has been published to study prevalence, predictors and the impact of fatigue in IBD.3,9,30 In IBD, higher levels of fatigue have most frequently been associated with increased disease activity,3,7,8,31 but numerous other physical and psychological factors that may influence fatigue have been identified.6,7,31,32 Prior studies are also conflicting in regard to some of these factors.30,32 Although the interest in research has increased, IBD fatigue still remains inadequately investigated.
Pain has been reported to be a frequent complaint and concern among IBD patients and is also related to disease activity (e.g. measured by SCDAI).14,33 In this regard, we hypothesised that pain symptoms could be associated with fatigue. Our findings reveal that crude pain intensity scores were twice as high in UC patients with SF compared to those without, whereas in CD, the score was one-third higher in patients with SF. Moreover, when comparing patients with and without CF, the differences in pain intensity further increased regardless of the diagnosis. Consequently, these results seem to align with prior studies in e.g. RA16,34 and MS. 17 Indeed, in RA, studies have indicated that pain may be a stronger predictor of fatigue than disease activity. 35 Several causal explanations for this association have been proposed. On one hand, fatigue could be caused by prolonged pain exposure and dealing with pain is energy consuming. On the other hand, fatigue can cause more pain due to less ability to deal with pain. 35 However, in RA, longitudinal studies have not indicated that one precedes the other, but that pain and fatigue seem to be synchronous. 34
However, given prior identification of the factors associated with IBD fatigue, 3 a potential association between pain and fatigue cannot be based merely on crude scores. Consequently, taking into account potential covariates, such as age, disease activity, depression, anxiety, sleep problems, haemoglobin and ferritin levels, seems inevitable.4,7,8,32 Furthermore, calprotectin has been shown to be a more specific marker of intestinal inflammation than CRP. 36 Hence, CRP and calprotectin may be measuring something quite different. Therefore, both were entered as covariates in the ANCOVA. Our findings indicated that after controlling for these potential covariates, patients with fatigue tended to have higher pain intensity levels. However, the levels of pain intensity scores were not statistically significantly different from those patients not reporting fatigue. Moreover, these findings confirm the importance of taking into account factors such as disease activity, depressive symptoms and sleep problems when investigating fatigue.
Even though one strength of the current study is the large sample of IBD patients recruited from multiple centres, a limitation may be related to the fact that the results in this study are based merely on hospital outpatients. The latter may cause speculations as to whether the patients recruited were those with more active disease and more frequent hospital visits. However, it is important to emphasise, even though such a bias cannot be ruled out, that the vast majority of Norwegian IBD patients are found in specialised hospital clinics. Another limitation is that the Basic Nordic Sleep Questionnaire has not previously been validated in IBD. Moreover, the pain intensity scale of the BPI is a generic pain scale and does not differentiate between different pain locations. Consequently, it is impossible to assess whether pain intensity in this population is mainly driven by abdominal or extra-intestinal pain. Although plasma ferritin is in equilibrium with body stores, we did not measure serum iron and total iron-binding capacity (TIBC), which could have provided us a clearer picture of the iron status in this population.
In conclusion, after adjusting for relevant covariates, the statistically significant association between pain intensity and fatigue in IBD disappeared. However, judged by Cohen’s effect size, these differences may not be trivial in a subset of patients. Thus, despite the lack of statistical significance, we believe that an assessment of pain may be important in patients troubled by fatigue. Future studies need to examine whether pain interventions may have a beneficial effect on fatigue.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.