
Abstract
Background and study aims
Percutaneous endoscopic gastrostomy (PEG) in head and neck cancer (HNC) patients is associated with higher complication and mortality rates when compared to a general patient population. The pull technique is still the preferred technique worldwide but it has some limitations. The aim of this study is to compare the pull and introducer PEG techniques in patients with HNC.
Patients and methods
This study is based on a retrospective analysis of a prospectively collected database of 309 patients with HNC who underwent PEG in the Cancer Institute of São Paulo.
Results
The procedure was performed with the standard endoscope in 205 patients and the introducer technique was used in 137 patients. There was one procedure-related mortality. Age, sex and albumin level were similar in both groups. However in the introducer technique group, patients had a higher tumor stage, a lower Karnofsky status, and presented more frequently with tracheostomy and trismus. Overall, major, minor, immediate and late complications and 30-day mortality rates were similar but the introducer technique group presented more minor bleeding and tube dysfunctions.
Conclusion
The push and introducer PEG techniques seem to be both safe and effective but present different complication profiles. The choice of PEG technique in patients with HNC should be made individually.
Introduction
Patients with head and neck cancer (HNC) are at high risk of malnutrition. More than 50% of patients with advanced disease have significant weight loss and possible cachexia. 1 During treatment, treatment-related toxicities and anatomical changes may impair swallowing and caloric intake. Up to two-thirds of HNC patients present with dysphagia at diagnosis and 75% post-treatment. 2 A recent study showed that 58% of patients with HNC in the USA received a feeding tube before or during treatment. 3
Percutaneous endoscopic gastrostomy (PEG) is the method of choice to provide long-term (>30 days) tube feeding in patients who are unable to swallow. The pull technique was first described by Gauderer et al. 4 and is the preferred technique worldwide due to its simplicity and low complication rate. However, this technique has some limitations in patients with HNC. Severe malignant stenosis and trismus may preclude the passage of the endoscope in up to 20% of patients with HNC. 5 Moreover there is an increased infection rate and a low but definite risk of implanting metastases at the PEG site.6,7 The introducer technique avoids passage of the feeding tube through the oropharynx and may overcome some of these limitations. It was first described by Russell et al. 8 and had several modifications over the years.5,9,10 The main modification was the introduction of gastropexy, which rendered the introducer technique safer. 11 However, previous published studies comparing both techniques show conflicting results.12–17
The aim of this study is to compare the results of the pull and introducer PEG techniques in patients with HNC in a tertiary oncologic hospital.
Material and methods
This study was based on a retrospective analysis of a prospectively collected database of all patients with HNC who underwent PEG at the Cancer Institute of São Paulo from December 2008 to October 2013. The indication for PEG placement was made by the treating oncologist or head and neck surgeon.
Clinical data included age, gender, Karnofsky performance status, albumin, anticoagulant/platelets antiagregant use, tumor location, tumor staging, trismus, larynx’s tumor involvement, tracheostomy, and whether PEG was performed before, during, or after treatment. Procedure data included antibiotic use, need for dilation, type of endoscope used, PEG technique, success of PEG placement, and related complications.
The ethics committee of the Cancer Institute of São Paulo approved the study protocol. Written informed consent was obtained from all patients.
PEG
PEGs were performed under propofol sedation by an anesthesiologist. Patients were intubated at the discretion of the anesthesiologist. All patients received antibiotic prophylaxis with first generation cephalosporin, except those patients who were receiving antibiotics for other diseases. The type of endoscope (slim or standard endoscopes) (GIF-N180 and GIF-Q180, Olympus Co., São Paulo, Brazil) and PEG technique was selected at the discretion of the endoscopist. Briefly, in patients with trismus or limited mouth opening, a slim scope was introduced transnasally and the introducer technique was selected. The finding of significant oropharynx stenosis was another common indication for the introducer technique using the slim endoscope. Dilation of the tumor with Savary bougies was made in those cases where severe tumoral stenosis precluded the passage of the endoscope.
The pull technique was based on the standard procedure described by Gauderer et al. 4 A small incision, approximately 1 cm, was made at the transillumination site. A puncture needle was inserted through the incision into the stomach and a stiff thread was passed through the needle under endoscopic view. The thread was grasped by a snare and brought through the patients’ mouth. The PEG tube was tied to the thread and pulled through the esophagus into the stomach to exit the abdomen (PEG 24-Pull, Cook Medical, Bloomington, USA).
The introducer technique was performed with a double-needle gastropexy device and a trocar with a peel-away sheath (Freka Pexact, Fresenius Kabi, Bad Homburg, Germany). Gastropexy was performed with two polypropylene sutures, 2 cm distant from each other, using the double-needle gastropexy device. A 1 cm incision was made between both sutures and the trocar was inserted into the stomach. The trocar was removed leaving the sheath in place. A 15Fr gastrostomy tube was inserted inside the sheath into the stomach, the balloon was inflated with 5 ml of distilled water and the peel-away sheath was removed.
Follow-up and complications
Each patient was evaluated one day after the procedure, and then on days 7, 15, 30 postprocedure, and then monthly for 180 days. Before discharge all patients were taught about tube care. Nurses reinforced the importance of tube rotation and mobilization, as well as tube flushing after each meal. In those patients with balloon gastrostomy tube, the balloon content was checked in every consultation. Gastropexy sutures were removed 15 days after the procedure. The 15Fr PEG tube was changed 30 days after the procedure, according to the manufacturer’s recommendation, and the 24Fr was changed 180 days after the procedure. Nutritional status follow-up was provided by the treating oncologist and nutritionist.
Complications were divided into immediate (until 24 h after the procedure) or late (after 24 h of the procedure), and major (required endoscopic therapy, surgical intervention, or prolonged hospitalization) or minor (required only local and conservative treatment). Major complications included acute respiratory failure, aspiration, major bleeding at the PEG site (hematemesis, melena, or hemoglobin drop of 2.0 g/dl or more), upper GI bleeding (major bleeding not from the PEG site), buried bumper syndrome, inadvertent early tube removal (<7 days), peritonitis, gastrocolic fistula, and PEG-site metastasis. Minor complications included local pain, dermatitis, granulation tissue, wound infection, peristomal leakage, minor bleeding at the PEG site (self-limited abdominal or gastric wall oozing), and tube dysfunction (dysfunction of the PEG tube before the 30th postoperative day).
Statistical analysis
Continuous variables with normal distribution were described as mean and standard deviation. Categorical variables were described through absolute and relative frequencies. Student's t-test was used to compare normally distributed continuous variables. Differences of categorical variable between groups were compared using the chi-squared test, or Fisher’s exact test where appropriate. All data were arranged, processed and analyzed with SPSS v.20.0 data (Statistical Package for Social Sciences, SPSS Inc., Chicago, Illinois, USA). Reported p-values of <0.05 were considered statistically significant.
Results
Study population
From December 2008–October 2013, 415 patients were sent to the endoscopy unit for PEG and 314 (75.7%) patients had HNC. PEG was successful in 309 (98.4%) patients who were included in the study. PEG failure occurred in five patients, two patients had a severe stenosis that precluded the passage of the slim endoscope even after dilatation, transillumination was not possible in two patients, and one patient had a large laryngeal tumor and refused tracheostomy so the procedure was contraindicated due to the high risk of respiratory failure.
Demographic and descriptive data
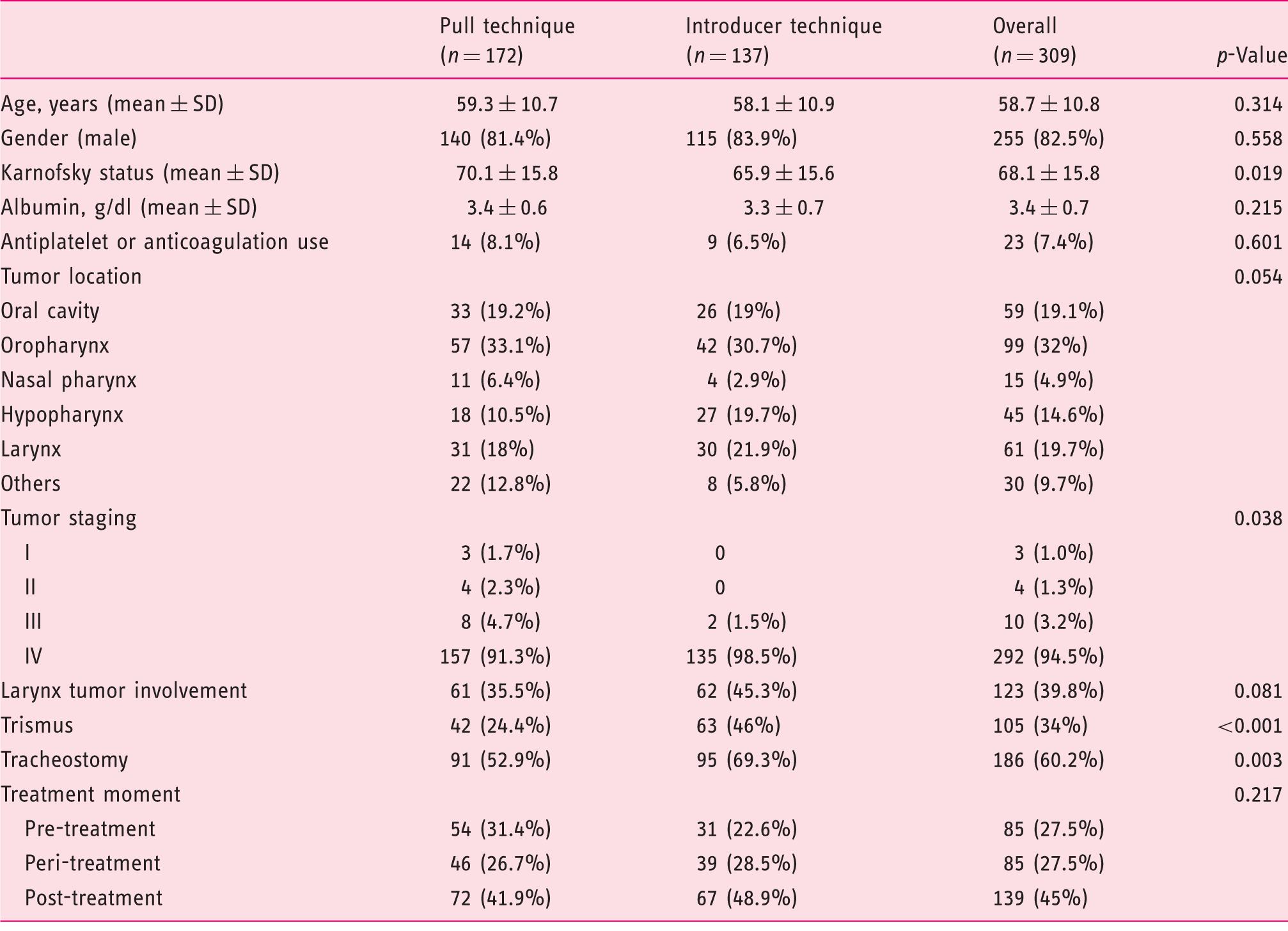
SD: standard deviation.
Procedure and follow-up
The procedure was performed with the standard endoscope in 205 (66.3%) patients and the introducer technique was employed in 137 (44.3%) patients. There was one procedure-related mortality (0.3%). The patient had an advanced oral cavity tumor and underwent PEG with the pull technique. Two hours after the procedure he presented major tumoral bleeding followed by massive aspiration. Thirty-day mortality was 20.7%.
Mean follow-up period was 103.8 days. Altogether 106 patients were followed for 180 days and 15 patients resumed oral intake and had their gastrostomy tube removed prior to the end of the follow-up period.
Complications
Complications and mortality following percutaneous endoscopic gastrostomy (PEG)
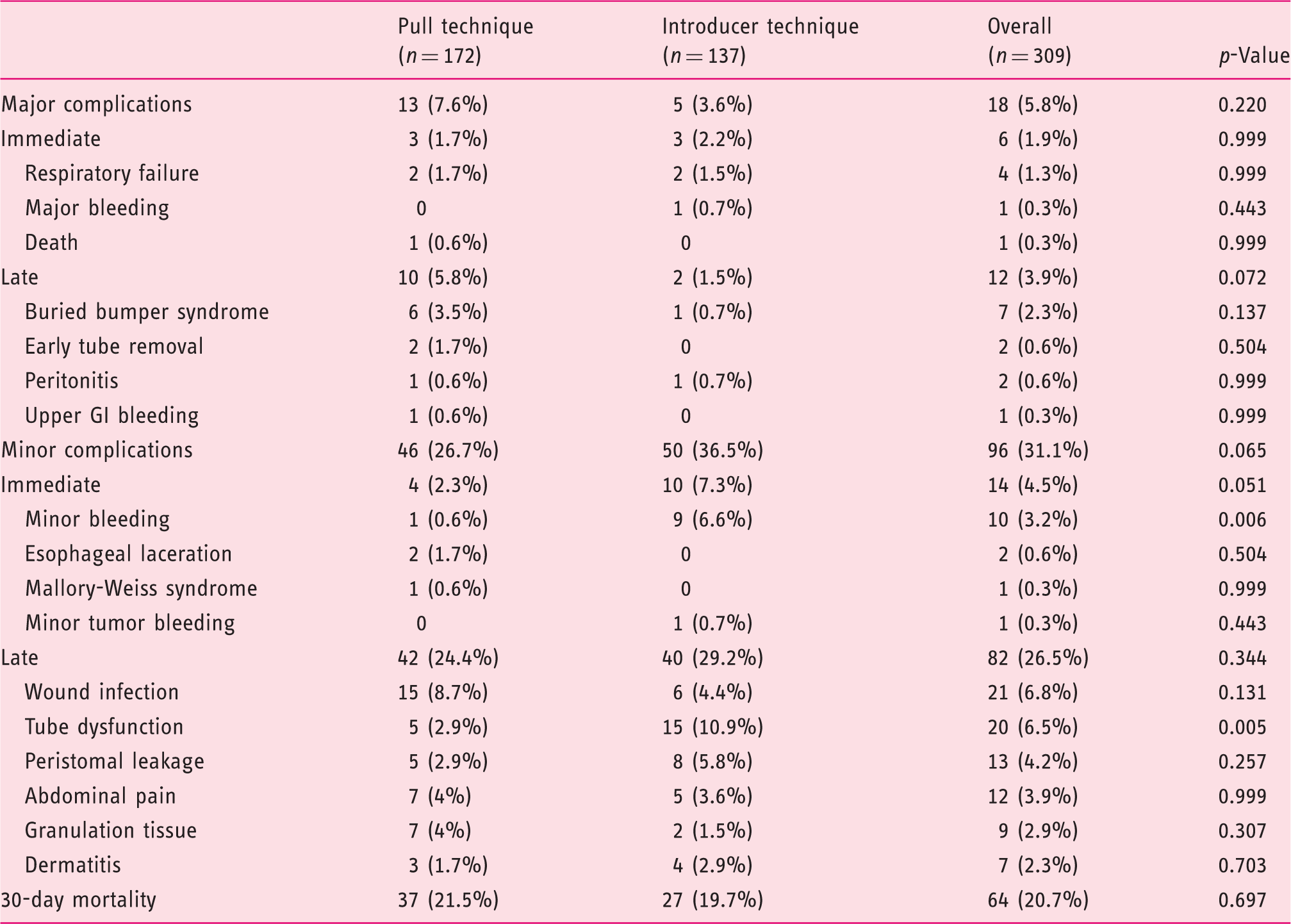
The immediate complication rate was 6.5%. Major immediate complications were observed in six (1.9%) patients, respiratory failure in 1.3%, major bleeding at the PEG site in 0.3% and death caused by aspiration due to tumor bleeding in 0.3%. Three of the patients with respiratory failure were intubated with the help of a broncoscope and the other had an emergency tracheostomy. The only case of major bleeding at the PEG site happened with the introducer technique and was controlled with traction of the gastrostomy tube. No transfusion was needed.
Minor immediate complications were observed in 14 (4.5%) patients, minor PEG-site bleeding in 3.2%, esophageal lacerations in 0.6%, Mallory-Weiss syndrome in 0.3% and minor tumor bleeding in 0.3%. Minor PEG-site bleedings were controlled by traction of the PEG tube. No specific treatments were needed to the other complications.
The late complication rate was 30.4%. Major late complications were observed in 12 (3.9%) patients, buried bumper syndrome in 2.3%, early tube removal in 0.6%, intraperitoneal leakage followed by peritonitis in 0.6% and upper GI bleeding due to an ulcer in the gastric wall opposite to the inner tube bumper in 0.3%. There was no case of PEG-site metastasis in our series. All cases of buried bumper syndrome could be managed endoscopically. Early tube withdrawal happened two and three days after PEG in patients in the pull technique group. Both patients were stable, without signs of peritonitis and sepsis. We tried to pass a guidewire to the stomach through the gastrostomy incision without success, so we decided to perform a transgastric exploration and PEG rescue as previously described by our group. 18 Both procedures were successful and the patients recovered uneventfully. Two patients required exploratory laparotomy for intraperitoneal leakage. One patient in the pull technique group presented severe abdominal pain with signs of peritonitis one day after the procedure. The exploratory laparotomy showed that the stomach was well attached to the abdominal wall and no cause for the peritonitis was found. The other patient was in the introducer technique group and presented gastric detachment of the abdominal wall during PEG tube replacement 60 days after the procedure. The hemorrhagic gastric ulcer was treated with a combined endoscopic therapy.
Minor late complications were observed in 69 (22.3%) patients but 12 of them presented more than one minor complication and the overall rate was 26.5%; wound infection in 6.8%, tube dysfunction in 6.5%, peristomal leakage in 4.2%, abdominal pain in 3.9%, granulation tissue in 2.9%, and dermatitis in 2.3%. Wound Infection was managed with local care and enteral antibiotics. Patients with tube dysfunction had their gastrostomy tube replaced. Non-opioid analgesics were enough to control abdominal pain in all patients. Peristomal leakage, granulation tissue, and dermatitis were managed with local care and tube adjustment when needed.
Comparison of techniques
When we compare the pull and the introducer PEG technique groups, age, sex, and albumin level were similar in both of them. However, in the introducer technique group, patients had a higher tumor stage (p = 0.038), a lower Karnofsky status (p = 0.019), and presented more frequently with tracheostomy (p = 0.003) and trismus (p < 0.001). The slim endoscope was used more often with the introducer technique (p < 0.001). The overall, major, minor, immediate, and late complications as well as 30-day mortality rates were similar in both groups. However patients in the introducer technique group presented a higher minor bleeding rate (p = 0.006). Most of these patients presented bleeding at the trocar insertion site, only one patient had bleeding at the gastropexy point. Tube dysfunction was also more common in the introducer technique group (p = 0.005). Although there was a higher infection rate in the pull technique group, it was not statistically significant (8.7% vs 4.4%, p = 0.131).
Discussion
PEG is the method of choice to provide nutritional support when long-term tube feeding is expected and the pull technique is the most commonly adopted one, probably due to its simplicity and efficacy. Pull PEG success rate in a general patient population is above 95%. 19 However, in patients with HNC it may be as low as 80% due to the presence of trismus, actinic or tumoral stenosis, and airway obstruction.5,20 Higher PEG-related complication and mortality rates were also reported in HNC patients.20–22 We present the largest study comparing two PEG techniques in HNC patients from a tertiary oncologic center. Our PEG success rate was 98.4% and it is probably explained by the high rates of the slim scope use (33.7%) and of the introducer technique (44.3%). In fact, the development of the introducer technique, the gastropexy and the slim scope raised the success rate in patients with HNC and now it is similar to the general patient population.5,21,22 The use of the slim scope allows transnasal passage of the scope in patients with severe trismus and avoids dilation and its complications in patients with actinic or tumoral stenosis. Furthermore, with the introducer technique there is no need to pass the internal bumper of the tube through the tumor, which decreases the risk of tumoral bleeding, perforation, wound infection, and PEG-site metastasis.5,12,21,22
Major complications in the general population occur in 1.5–9.4% after PEG, similar to 7.4% in HNC patients.20,23 In our series, major complications occurred in 5.8% of the procedures. Most of our immediate major complications were related to airway problems. These complications happened at the beginning of our series. Thereafter, all patients had a routine pre-procedure consultation with the anesthesiology team. When a possible airway problem was anticipated a tracheostomy or an alternative to PEG, such as a nasoenteric feeding tube, was offered. Special attention must be taken before sedation in patients with HNC as they have a high risk of airway obstruction and acute respiratory failure because of anatomic distortions caused by the tumor, surgery, or radiotherapy.24,25
Considering that, in our series, the introducer technique was mostly employed in patients with severe trismus or oropharyngeal stenosis, it is easy to understand that this group of patients presented with lower performance status, higher tracheostomy rate, and more advanced staging. We might expect a higher complication rate in this group of more compromised patients. However we observed that both the major and minor complications as well as 30-day mortality rates did not differ between the groups. Although the pull technique group presented a higher infection rate of 8.7% vs 4.4%, it did not reach a statistical significance (p = 0.13), a possible type II error. In a recent meta-analysis, Campoli et al. 6 showed that the pull technique is associated with higher infection rates. This could be explained by the contamination of the PEG tube during its passage through the oropharynx when the pull technique is used. This is especially true in patients with HNC that can present oral and hypopharyngeal bacterial overgrowth secondary to the tumor. 22 Antibiotic prophylaxis has been proven to decrease PEG wound infections and was provided in all our patients according to the American and Brazilian guidelines.26–28
Bleeding at the PEG-site is an uncommon complication and occurs in less than 1% of the procedures. 23 However, studies with the introducer technique have controversial results, with some studies showing higher bleeding rates and others reporting similar results. Koide et al. 29 showed a bleeding rate of 3.9% and multiple logistic regression analysis demonstrated an association with the introducer technique. Yagishita et al. 21 and Chadha et al. 30 also reported bleeding rates of 8.2% and 3.7%, respectively. Nevertheless, some studies comparing both the introducer and the pull techniques showed similar bleeding rates.12,13,22 Our bleeding rate was 3.6% with only one case of major bleeding that occurred in the introducer technique group. When we compared both techniques, the introducer technique presented a higher minor bleeding rate 6.6% vs 0.6% (p = 0.006) which can probably be explained by the four needle punctures needed to perform the gastropexy and by the use of a large 15Fr trocar, compared with only one needle puncture needed in the pull technique.
Early tube withdrawal (<7 days) after the pull technique carries a high risk of free perforation and peritonitis because the PEG tract is not yet mature. Surgical treatment by exploratory laparotomy or laparoscopy is usually advised, however an endoscopic tube replacement with retrograde technique or conservative treatment can be tried if peritonitis is not present.31,32 PEG rescue by the NOTES technique has been described as less invasive procedure than surgery.18,33 In both patients with early tube removal in our series, PEG rescue was performed with success and patients recovered uneventfully. Although early tube withdrawal is more frequent with the introducer technique because of the tube design, it is not a major concern, as gastropexy facilitates tract maturation and minimizes the risk of gastric dislodgment of the abdominal wall. Gastropexy should always be done before the introducer technique but it should also be considered in those confused and agitated patients submitted to gastrostomy by the pull technique.
One patient in our series, in the push technique group, presented gastric dislodgment of the abdominal wall during PEG tube replacement 60 days after the procedure. This is a rare complication with few reports in the literature. 32 Special care with tube replacement should be taken in malnourished and immunosuppressed patients, as the PEG tract takes longer to mature, and in lengthy (more than 6–8 h) PEG removal, the possible stenosis of the stoma may increase the force needed to place the tube. 32
PEG site metastasis is major concern following PEG in HNC patients. It occurs in about 0.5–1% of the procedures in pharyngoesophageal cancer patients.7,34 Cappell et al. 7 reported some risk factors for gastric metastasis. Pathologic factors included pharingoesophageal location, squamous cell histology, advanced cancer stage, poorly or moderately differentiated histology, and a large mass. Therapeutic factors included endoscopic gastrostomy with the pull technique and untreated cancer or known local recurrence. The most accepted explanation is the direct implantation of tumor cells brought by the gastrostomy tube that passed through the tumor.7,34 However, hematogenous or lymphatic dissemination to the PEG site are also plausible. Recently, the first of case of PEG site metastasis with the introducer technique was described. 35 We had no cases of PEG site metastasis in our series. However, our follow-up might have been too short to identify stomal metastasis. In a previously published study, the mean interval between PEG placement and PEG site metastasis was 7.8 ± 5.2 months. 7
Our tube dysfunction rate was 6.5%. The introducer technique presented a higher tube dysfunction rate 10.9% vs 2.9% (p = 0.005). This could be explained by the different tube designs. The gastrostomy tube used in the pull technique had a 24Fr diameter and an internal bumper while the tube used in the push technique had a 15Fr diameter and a 5 ml balloon in the tip. Probably the smaller diameter of the tube facilitated its occlusion and the small balloon facilitated the dislocation. Nursing care and orientation with the gastrostomy tube is essential to minimize complications and tube dysfunction. Flushing the tube after each meal minimizes the chance of obstruction and balloon checking avoids tube dislodgment. Tube rotation, mobilization, and external bolster adjustment may avoid buried bumper syndrome, peristomal leakage, and dermatitis.
PEG-related mortality among patients with HNC is reported to be 2.2% while in the general population it decreases to 0.53%.19,20,23 In our study we had only one death (0.3%) related to the procedure. However our 30-day all-cause mortality was 20.7%, higher than in general population (14.7%). 23 Half of our patients received a PEG after the definitive treatment. We hypothesize that some of these patients were in the end stage of their disease for whom PEG should not be indicated.
Comparative studies – pull versus introducer percutaneous endoscopic gastrostomy (PEG) techniques
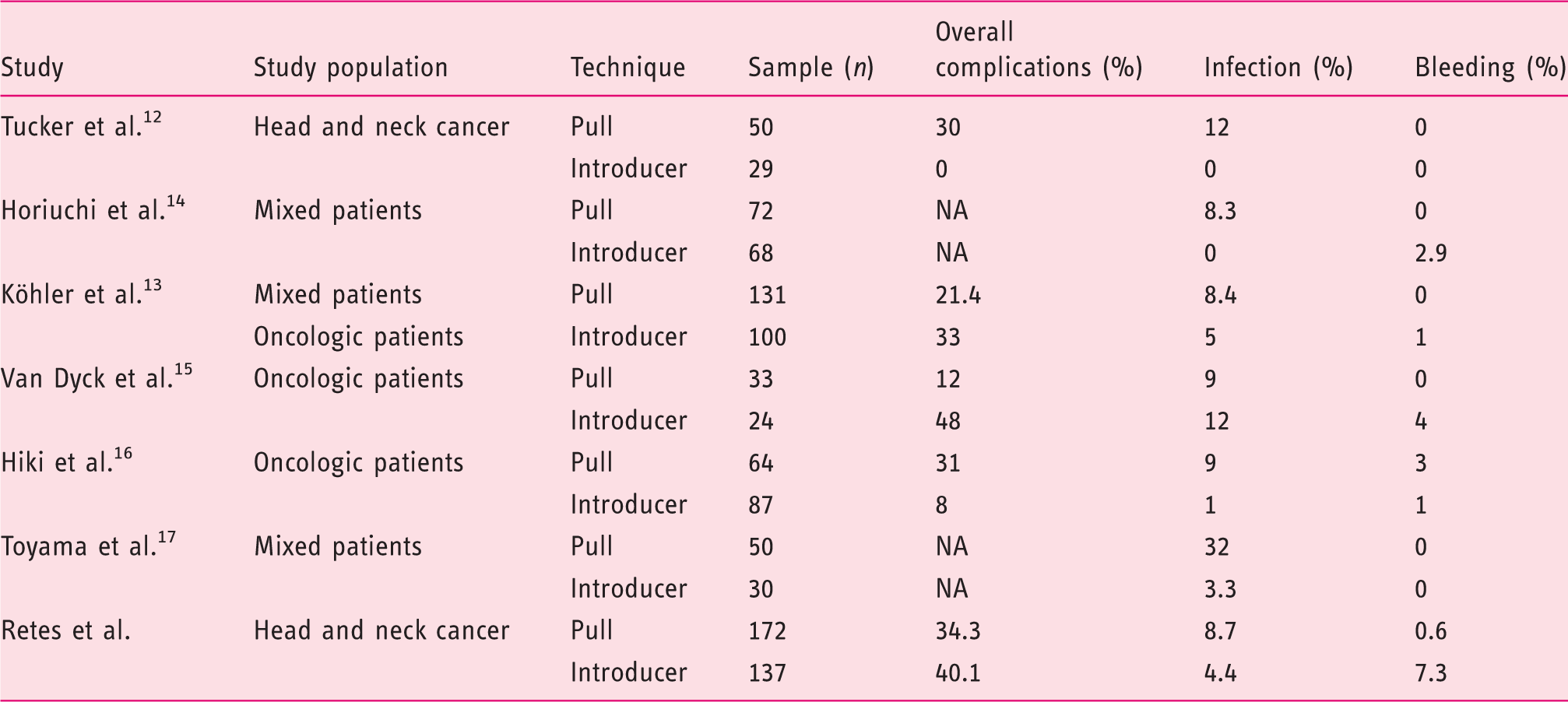
NA – not available.
The main limitation of the present study was the non-randomized design. However in the scenario of a randomized controlled trial, a major limitation would be the allocation of patients with severe oropharyngeal stenosis to the pull technique group. In this setting, even with the use of the slim scope, tumor dilation could be needed for the passage of the internal bumper of the gastrostomy tube which could cause major complications.
Our data support the view that, once the choice of the technique is customized, both push and introducer PEG techniques seem to be safe and effective in patients with HNC, but present different complication profiles. Patients with large tumors, severe trismus, confusion or psychomotor agitation, and immunosuppression should have PEG placed with the introducer technique. In addition, the risk of PEG site metastasis should always be kept in mind when performing PEG in head and neck cancer patients. Although this is a rare complication, it compromises patient's prognosis and survival. Therefore, whenever possible, the introducer technique should be considered the first option of gastrostomy technique in HNC patients. The pull technique should be reserved for HNC patients with small, non-obstructive lesions.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.