
Abstract
Aim
Diagnosis of laryngopharyngeal reflux (LPR) has dramatically increased over the last years. For diagnosis of gastroesophageal reflux, a newly designed pharyngeal probe (Dx-pH) was recently introduced. It is also recommended to guide therapy decision in antireflux surgery. However, diagnostic results are questionable. Therefore, we establish a reliable reference group with asymptomatic patients after total gastrectomy and, thus, complete extinction of gastric acid production.
Methods
Pharyngeal pH monitoring was performed in 10 consecutive patients with history of total gastrectomy. All patients were off proton pump inhibitor (PPI) therapy and followed a non-acid diet during the complete measurement period.
Results
All procedures were performed without any complication. Six of the 10 asymptomatic gastrectomy patients (60%) had pathological results derived from the validated reference values (Ryan score) in pharyngeal pH monitoring.
Conclusion
Pathological pH values assessed by the Dx-pH device, usually interpreted as pathological aerosolized acidic gastroesophageal and/or laryngopharyngeal reflux, are obviously dissociated from gastric acid production. Further studies are required to determine diagnostic value of the new system. Therefore, the pharyngeal pH monitoring system seems currently not to be useful to guide any diagnostic or therapeutic decisions, in particular if surgical therapy is considered.
Introduction
Diagnosis of laryngopharyngeal reflux (LPR) has dramatically increased over the last decade.1,2 Patients report various symptoms, including chronic cough, globus sensations, hoarseness, asthma, sinusitis, and halitosis.3,4 Etiology of LPR remains unclear. It is assumed, that LPR symptoms are a result of laryngeal or pharyngeal alterations after exposure to acid gastric refluxate. Therefore recommended therapy consists of high dose acid suppression for up to six months. 5 For diagnosis of LPR, most reliable and safe tools are multichannel impedance monitoring in combination with pH monitoring (pH/II) and two-channel pH monitoring.6,7
Recently, a newly designed pharyngeal probe (Restech Dx-pH) which records pH values in the aerosolized laryngeal environment was introduced and is already commercially available. The main advantage of the new system is the comfortable position in the oropharynx above the upper esophageal sphincter (Restech Dx-pH, Restech, San Diego, CA, USA). Normal values and discriminating pH threshold were validated by a study group at University of Southern California. 8 Results are recommended to establish diagnosis of LPR and to guide daily clinical decisions. 9 There are also data suggesting that patients with pathological results in pharyngeal pH monitoring might benefit from antireflux surgery. 10
However, different study groups in Europe found substantial differences comparing impedance/pH monitoring and pharyngeal pH monitoring in simulations measurements.11–13 Differences were explained by the uncertain etiology of LPR with supposable extragastric acid production. 14 In a prospective trial, our study group could not detect relevant extragastric acid production in laryngeal epithelium of LPR patients. 15 So the role of pharyngeal pH monitoring including published reference values remains unclear.
The aim of this study was to establish a reliable reference group with asymptomatic patients after total gastrectomy and, thus, complete extinction of gastric acid production. This is of highest clinical interest since results in pharyngeal pH monitoring applying the postulated and widely accepted reference values are controversial.
Patients and methods
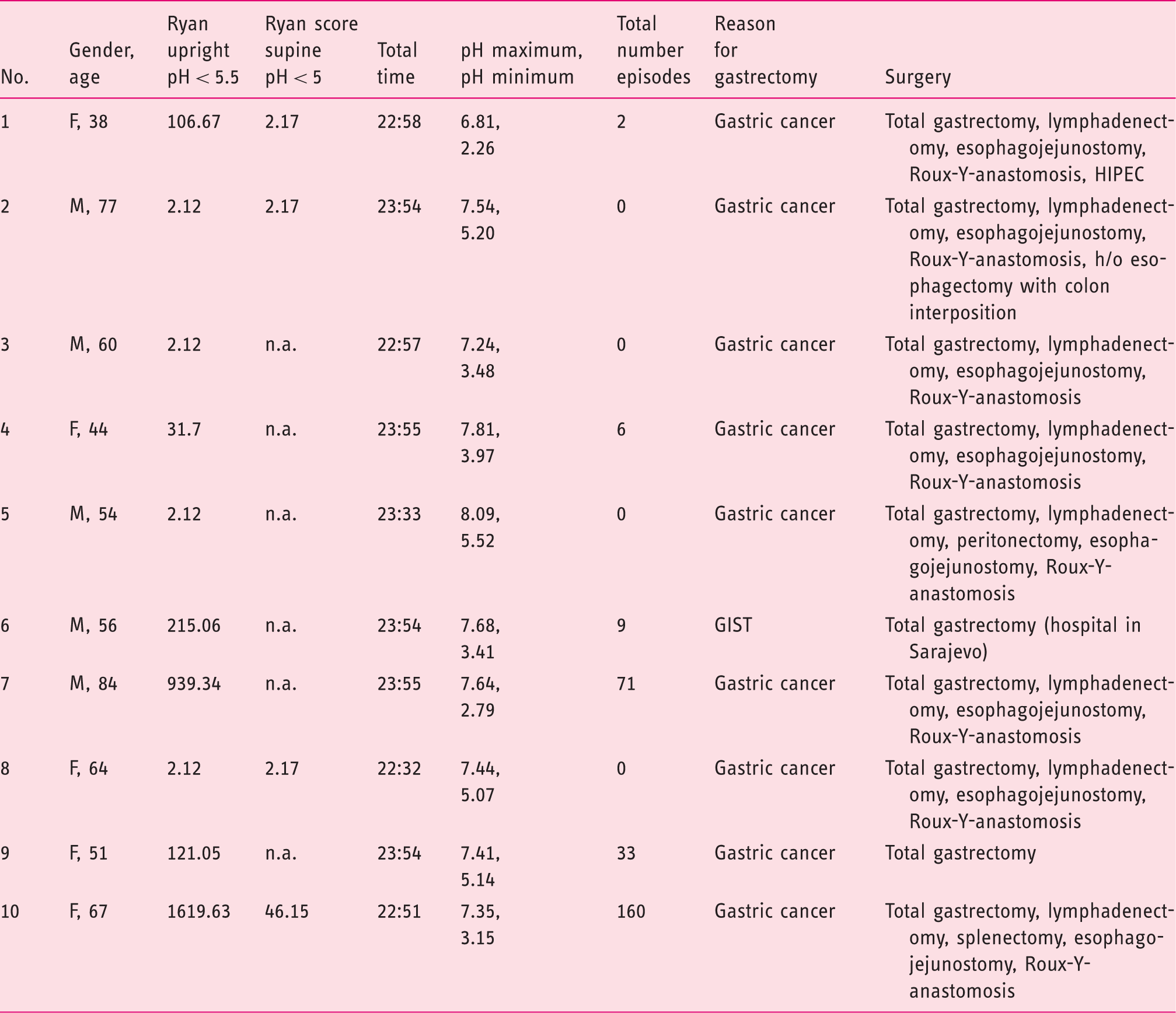
A total of 10 consecutive patients (male = 5 of age 54–84, av. 66.2 years, female = 5 of age 38–67, av. 52.8 years) all with history of total gastrectomy were included. No patient reported of any LPR symptoms or any gastrointestinal symptoms. The study was approved by the Ethics Committee of the Technische Universität München (study number 284/14). Complete informed consent to participate in the study and to evaluate the study data was obtained from all patients. All patients were off proton pump inhibitor (PPI) therapy and followed a non-acid diet during the complete measurement period.
After study inclusion, pharyngeal pH monitoring was performed in a standardized procedure as recommended by the provider and as described previously.12,16,17 For study evaluation, we used the Ryan score. The score combines the number of reflux episodes, the duration of the longest reflux episode, and the percentage of time below the respective threshold. 8 Criteria for pathological results are Ryan score > 9.4 in an upright position (pH < 5.5) or >6.8 in a supine position (pH < 5.0); pH monitoring was performed for a minimum of 22 hours.
Results
Patient data and results.
Discussion
In daily clinical routine we see more and more patients suffering from atypical reflux symptoms, presenting in our interdisciplinary gastroesophageal reflux disease outpatient clinic with a non-response to PPI and pathological results in Dx-pH monitoring. In most cases, the method was performed by ENT specialists and the presentation of the patients is initiated for evaluation of an interventional therapy (in most cases fundoplication). In recent studies, different research groups were able to show that the pathophysiology of atypical reflux symptoms is rarely understood and correlation of MII and Dx-pH is poor.
Therefore, we aimed to clearly question the value of the widely used Dx-pH monitoring applied as method for therapy guidance. So we established a reliable reference group with asymptomatic patients after total gastrectomy. Despite the lack of a standardized definition for pathological results in pharyngeal pH monitoring, we used the Ryan score for our study because it is widely accepted, used in a high number of recent publications and promoted by the producer. This is of highest clinical interest since results using the recommended, widely accepted and daily used reference values in pharyngeal pH monitoring are still controversial. These data might help to define the role of the new system in future. For study evaluation, we used the Ryan score because it is recommended by the manufacturer and by numerous previous trials.
8
To exclude supposable acid environmental factors, patient were additionally set on a non-acid diet during measurement although, due to the special shape of the new probe, manufacturer excludes any incorrect measurement by reason of food intake. The pH profile in our patients was very comparable to provided curves in previous publications interpreted as laryngopharyngeal reflux. There were no specific characteristics (Figure 1).
Representative pH profile in gastrectomy patients without any specific characteristics.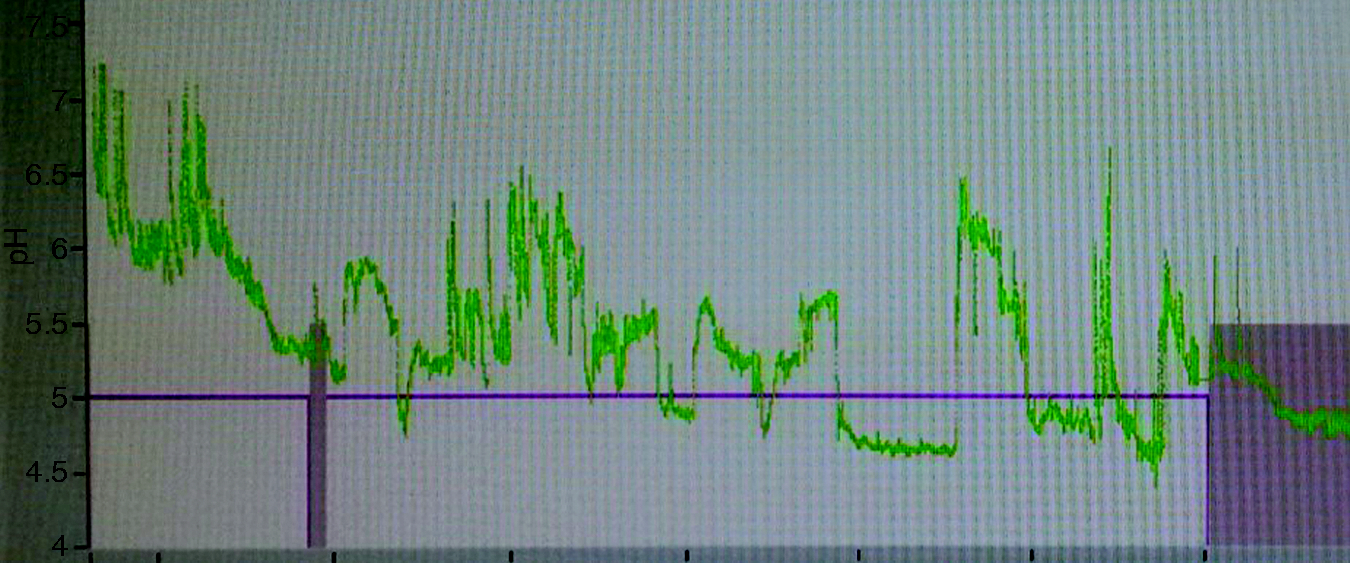
To avoid contribution of endogenous gastric acid production with consecutive acid reflux episodes we investigated only patients with a history of total gastrectomy. Pathological pH monitoring results in terms of gastric reflux in these patients must be regarded as incorrect. So, whatever we are measuring, it has nothing to do with gastric acid production.
Still, in six of the 10 gastrectomy patients (60%), the pharyngeal pH monitoring system detected pathological acid levels. These results are difficult to discuss. On the one hand, our results might support the theory of extra gastral acid production. On the other hand, in previous reports there is no evidence of clinical relevant laryngeal acid production by H+K+-ATPase proton pumps. 15 Another explanation might be the fact that the pharyngeal pH monitoring system detects for unknown reason higher numbers of pathological acid pH levels than other diagnostic tools. 18 This is somehow concordant with previous results of our study group detecting acid environment in the oropharynx in LPR patients without any correlation to gastroesophageal reflux episodes assessed by pH/impedance measurement. 12 Reason and etiology therefore remain unclear. Interestingly in our data, most pathological results were found in upright position, whereas in others report a drop of pharyngeal pH was more frequent and prolonged in the supine position. 8 Again, this raises the question what are we really measuring with this new device? At least, gastric acid reflux can be excluded because of the patient selection since any production of gastric acid is ceased with total gastrectomy. On might discuss an increased levels of non-acid reflux in patients after gastrectomy. However the current system does not allow any detection of non-acid reflux episodes. So, non-acid reflux cannot explain the pathological results of the pharyngeal pH probe.
As result of the uncertain etiology and controversial results in pharyngeal pH monitoring and esophageal pH monitoring one has to question antireflux surgery as a suitable therapy option in patients with LPR symptoms although a retrospective review reported symptom relief after surgical antireflux procedures more often in the group with pathological pharyngeal pH levels compared to the study group with pathological result esophageal pH levels after a median follow up of 18 months. 19
If 60% of patients with excluded gastric acid production have ostensibly pathological results in pharyngeal pH monitoring, it makes the diagnostic tool implausible. Based on our data, reference values described by Ayazi et al. need to be reconsidered, 8 and thresholds for LPR patient need to be redefined.
So far, the etiology of pathological values in gastrectomy patients remains unclear and further studies are needed to clarify these results. There is no conceptual reason why the system detects acid values after total gastrectomy with excluded gastral acid production. Based on our data, the pharyngeal pH monitoring system seems currently not to be useful to guide any diagnostic or therapeutic decisions, in particular if surgical therapy is considered.
Key messages
Diagnosis of laryngopharyngeal reflux (LPR) has dramatically increased over the last decade. A newly designed pharyngeal probe (Dx-pH) for detection of gastroesophageal and LPR was recently introduced. Study results are controversial using published reference values. We establish a reference group with asymptomatic patients after total gastrectomy and, thus, complete extinction of gastric acid production. Most of the asymptomatic gastrectomy patients (60%) had pathological results in pharyngeal pH monitoring More research needs to be done to determine diagnostic value of the new system. The Dx-pH system seems currently not to be useful to guide diagnostic or therapeutic decisions.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
Dirk Wilhelm has nothing to disclose. Alissa Jell has nothing to disclose. Hubertus Feussner has nothing to disclose. Roland M Schmid has nothing to disclose. Monther Bajbouj has received speaker honoraria and travel support from Restech and Neuwirth Medical Products (German distributor of Restech). Valentin Becker has received travel support from Restech.