
Abstract
Background
Patients with inflammatory bowel disease (IBD) tend to have smaller family sizes. Health care professionals (HCPs) may inadvertently provide inaccurate advice to patients resulting in voluntary childlessness or unfavourable pregnancy outcomes.
Objective
The study aims to objectively measure IBD-specific pregnancy-related knowledge of general practitioners (GPs) and obstetricians/gynaecologists (OB/GYNs) in comparison with gastroenterologists (GEs) using the validated Crohn’s and Colitis Pregnancy Knowledge (CCPKnow) questionnaire.
Methods
GPs, OB/GYNs and GEs in two Australian states completed the CCPKnow (range 0–17) and demographic questionnaires. The CCPKnow addresses issues pertaining to conception, IBD inheritance, risk of congenital abnormalities, medication use in the peri-conceptual period, pregnancy and breastfeeding, and mode of delivery.
Results
In total, 337 HCPs responded. GPs (n = 188/2086) and OB/GYNs (n = 94/228) had significantly lower knowledge than GEs (n = 55/165) for the composite CCPKnow (medians 11, 13 and 17, respectively, p < 0.001), and almost all domains. GEs were the only group to attain a median CCPKnow score in the top category (14–17). More than 70% of GPs and OB/GYNs expressed discomfort with initiation of IBD medications around conception/pregnancy. GPs (43.6%) and OB/GYNs (45.7%) perceived thiopurine use to be unsafe during pregnancy and to cause serious harm to the baby.
Conclusions
Our study demonstrates that GPs and OB/GYNs have inadequate and variable IBD-specific pregnancy-related knowledge including use of IBD medications. These results support the need for GEs’ prime role in a team-based management for IBD patients who are pregnant or planning pregnancy.
Introduction
Inflammatory bowel disease (IBD) commonly affects women and men during their reproductive years. At the time of diagnosis roughly half of patients are less than 35 years of age, and 25% become pregnant for the first time after the diagnosis of IBD. 1 The interactions between pregnancy and IBD are complex, presenting challenges both for patients and health care professionals (HCPs) who treat and advise them.
Women with IBD of childbearing age may encounter a variety of questions and dilemmas:2,3 whether to become pregnant and when; to continue, stop or change medications before attempting to conceive, or during pregnancy; to breastfeed or not; whether their IBD will put the child at an increased risk;4,5 and importantly, whether to or from whom they should seek accurate and appropriate information and advice.
Patients with IBD have smaller family sizes than the general population, commonly due to personal choice – also known as voluntary childlessness.6,7 This is despite fertility in patients with IBD being comparable to the general population except in patients who have undergone ileal pouch-anal anastomosis and in men on sulfasalazine.8,9 The cause of voluntary childlessness in patients with IBD is likely complex. Fear of pregnancy outcomes and fertility2,3 and lack of IBD-specific pregnancy-related knowledge are likely to play a role.10,11
Typically, pre-pregnancy and perinatal care is delivered by general practitioners (GPs) and gynaecologists (OB/GYNs). However, in order to avoid misinformation, voluntary childlessness and even adverse pregnancy outcomes, HCPs who provide advice and clinically manage patients with IBD of reproductive age require sound knowledge of IBD-specific pregnancy-related issues. Previously discomfort in managing IBD patients and a lack of correlation between comfort and knowledge was demonstrated in Australian GPs. 12 Due to their limited experience in handling IBD-related issues and limitations in their IBD-specific pregnancy-related knowledge, it is possible that inaccurate advice may be provided by GPs and OB/GYNs. Yet IBD-specific pregnancy-related knowledge has never been formally evaluated in these HCPs. Therefore, the aim of this study was to evaluate IBD-specific pregnancy-related knowledge among GPs, OB/GYNs and compare this to that of gastroenterologists (GEs). The hypothesis was that IBD-specific pregnancy knowledge of HCPs can directly influence an individual IBD patient’s choices and hence can directly influence the pregnancy outcomes.
Methods
Study design
GPs, OB/GYNs and GEs in two Australian states, New South Wales (NSW) and South Australia (SA), were invited to participate in the study by post. They were sent the study package, which included the 17-item Crohn’s and Colitis Pregnancy Knowledge (CCPKnow) questionnaire, questions on their demographics, comfort and attitudes and clinical practice relating to IBD-specific pregnancy-related issues, a letter outlining the aims of the study, privacy and consent information, and prepaid return envelopes. The CCPKnow is a recently developed and validated tool that assesses the level of IBD-specific pregnancy-related knowledge. 10 The questionnaire encompasses a wide range of IBD-related issues in pregnancy including inheritance of IBD, conception, medication usage (peri-conception, pregnancy and breastfeeding), mode of delivery, and risk of congenital abnormalities in babies born to IBD-affected mothers. 10 The total score range is 0–17 with 14–17 indicating very good knowledge, 11–13 good knowledge, 8–10 adequate knowledge and 0–7 poor knowledge as validated previously by Selinger at al. 10 The CCPKnow tool was validated in lay- and health care professionals with IBD specialist nurses considered the gold-standard of knowledge provision as they not only deal with professional medical advice but also cover holistic lifestyle issues deemed important in the overall management of pregnancy in the setting of IBD. When tested in 145 female patients (median age 32 years), 45% had poor, 28% adequate, 17% good and only 10% had very good CCPKnow scores, confirming the need for education from HCPs. 10 Questionnaire tool responsiveness was evident by significant score increases following a dedicated-educational program. 13 Given these characteristics, the CCPKnow tool was applicable and appropriate for the current research.
Invitees were asked to complete and return the survey within eight weeks. Invitees were identified from hospital referral databases, a public registry published by The Royal Australian and New Zealand College of Obstetricians and Gynaecologists (RANZCOG) (http://www.ranzcog.edu.au/womens-health/locate-an-obstetriciangynaecologist.html), and GE units of two teaching hospitals (Concord Repatriation General Hospital, NSW and Royal Adelaide Hospital, SA) and the surrounding metropolitan areas. They received up to two reminders during the eight-week return period by phone or email for surveys not returned by four and six weeks. Following the eight-week return period, surveys were not followed up further.
Sample size determination
A power calculation to detect one point size difference (medium effect, effect size f = 0.25) of the CCPKnow scores between GPs, OB/GYNs and GEs with 80% power and alpha value of 0.05 required recruitment of 159 participants in total. G*Power 3.1.7 tool was used to perform a priori power analysis.
Statistical analysis
The comparative knowledge of IBD-specific pregnancy-related issues amongst GPs, OB/GYNs and GEs was assessed with respect to the total CCPKnow score as well as individually for different domains of the CCPKnow questionnaire: inheritance, fertility, disease activity, safe use of drugs, mode of delivery, pregnancy outcomes and breastfeeding. Between-group differences were examined using the non-parametric Mann-Whitney U test, Spearman Correlation, and Kruskal-Wallis Test, where appropriate. A binary logistic regression analysis model was constructed to identify the independent predictors of very good knowledge and results were expressed as odds ratio (OR) and 95% confidence intervals (CIs). Statistical Product and Service Solutions 18 (SPSS 18) was used for data analysis (SPSS Inc, released 2009. PASW Statistics for Windows, version 18.0. Chicago: SPSS Inc, http://www.ibm.com/support/docview.wss?uid=swg21476197).
Ethics
The study was approved by the human research ethics committees (HRECs) of Concord Repatriation General Hospital (CRGH – HREC/11CRGH/28) and the Royal Adelaide Hospital (RAH – Protocol No: 111222). Return of the survey was taken as consent.
Results
Demographic characteristics of study participants
Demographic characteristics and CCPKnow scores: GPs
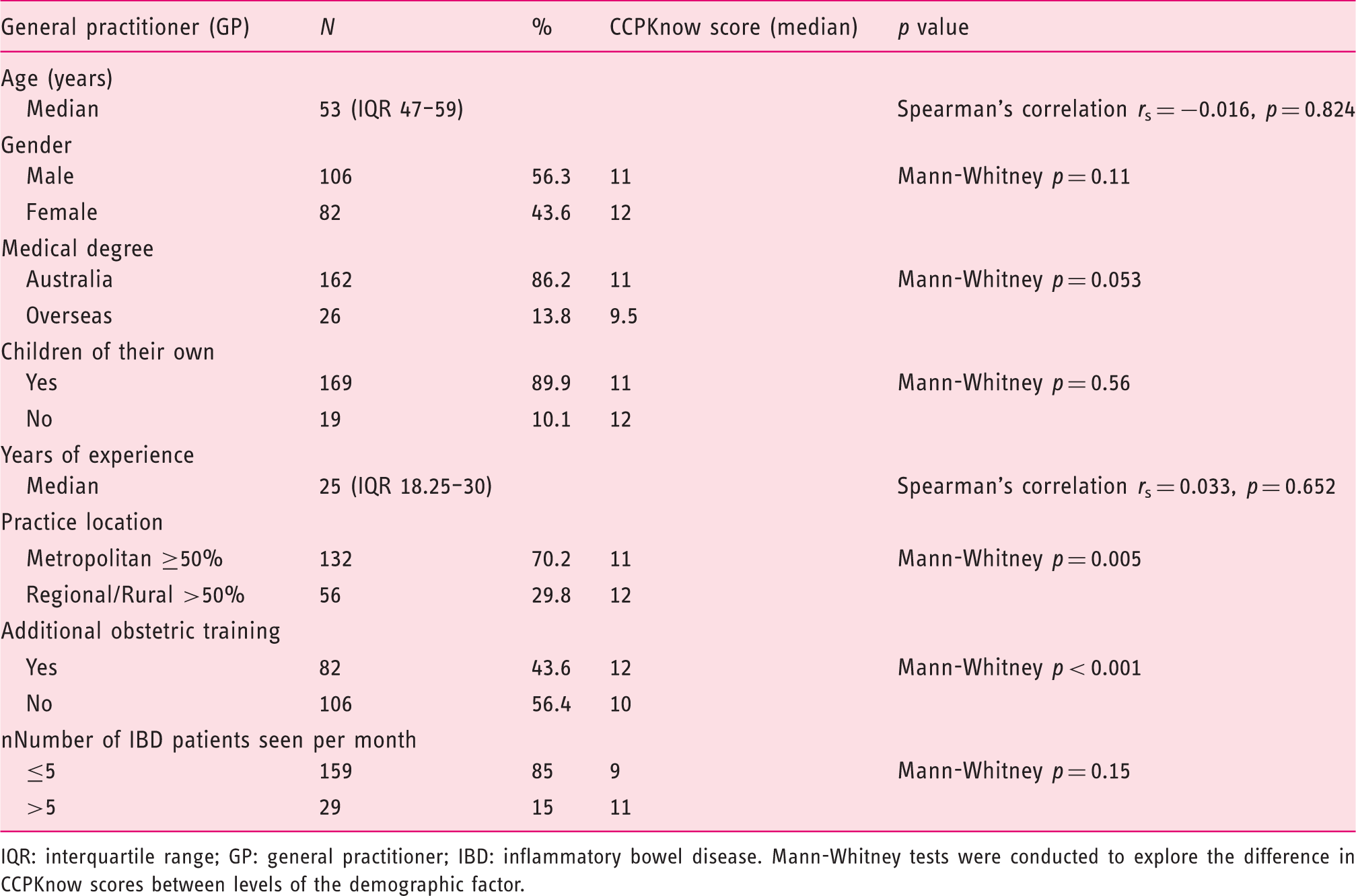
IQR: interquartile range; GP: general practitioner; IBD: inflammatory bowel disease. Mann-Whitney tests were conducted to explore the difference in CCPKnow scores between levels of the demographic factor.
Demographic characteristics and CCPKnow scores: OB/GYNs
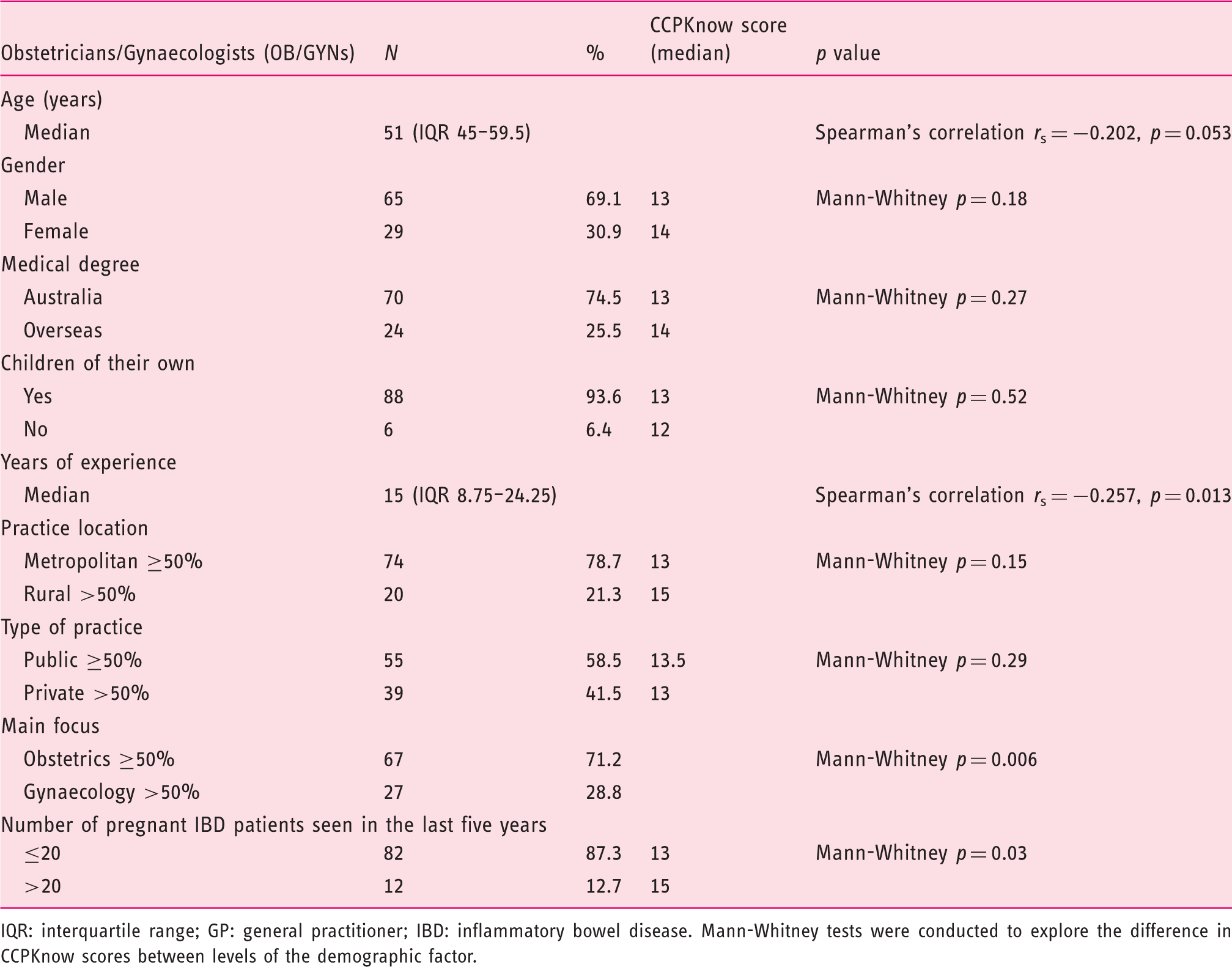
IQR: interquartile range; GP: general practitioner; IBD: inflammatory bowel disease. Mann-Whitney tests were conducted to explore the difference in CCPKnow scores between levels of the demographic factor.
Demographic characteristics and CCPKnow scores: GEs
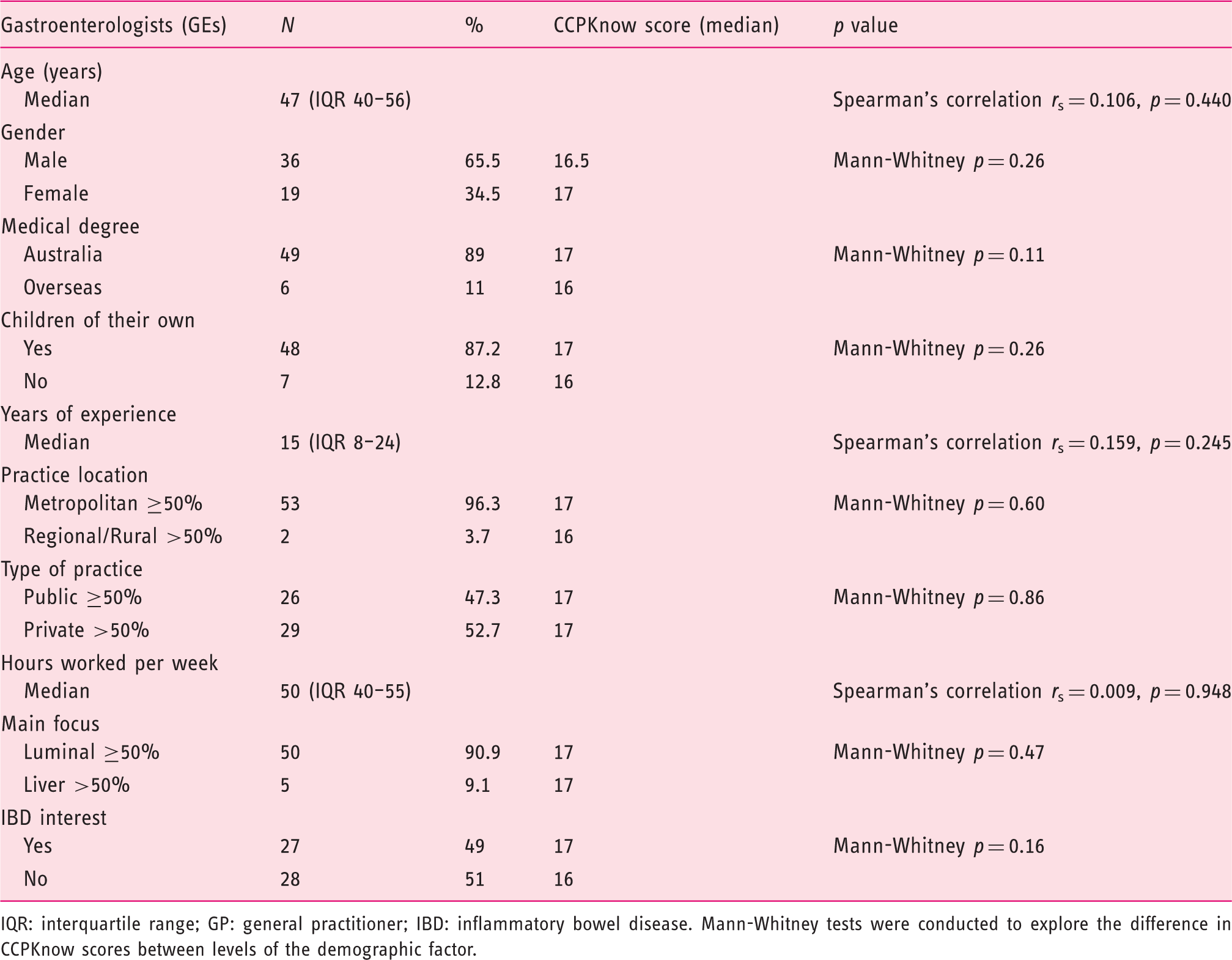
IQR: interquartile range; GP: general practitioner; IBD: inflammatory bowel disease. Mann-Whitney tests were conducted to explore the difference in CCPKnow scores between levels of the demographic factor.
CCPKnow scores
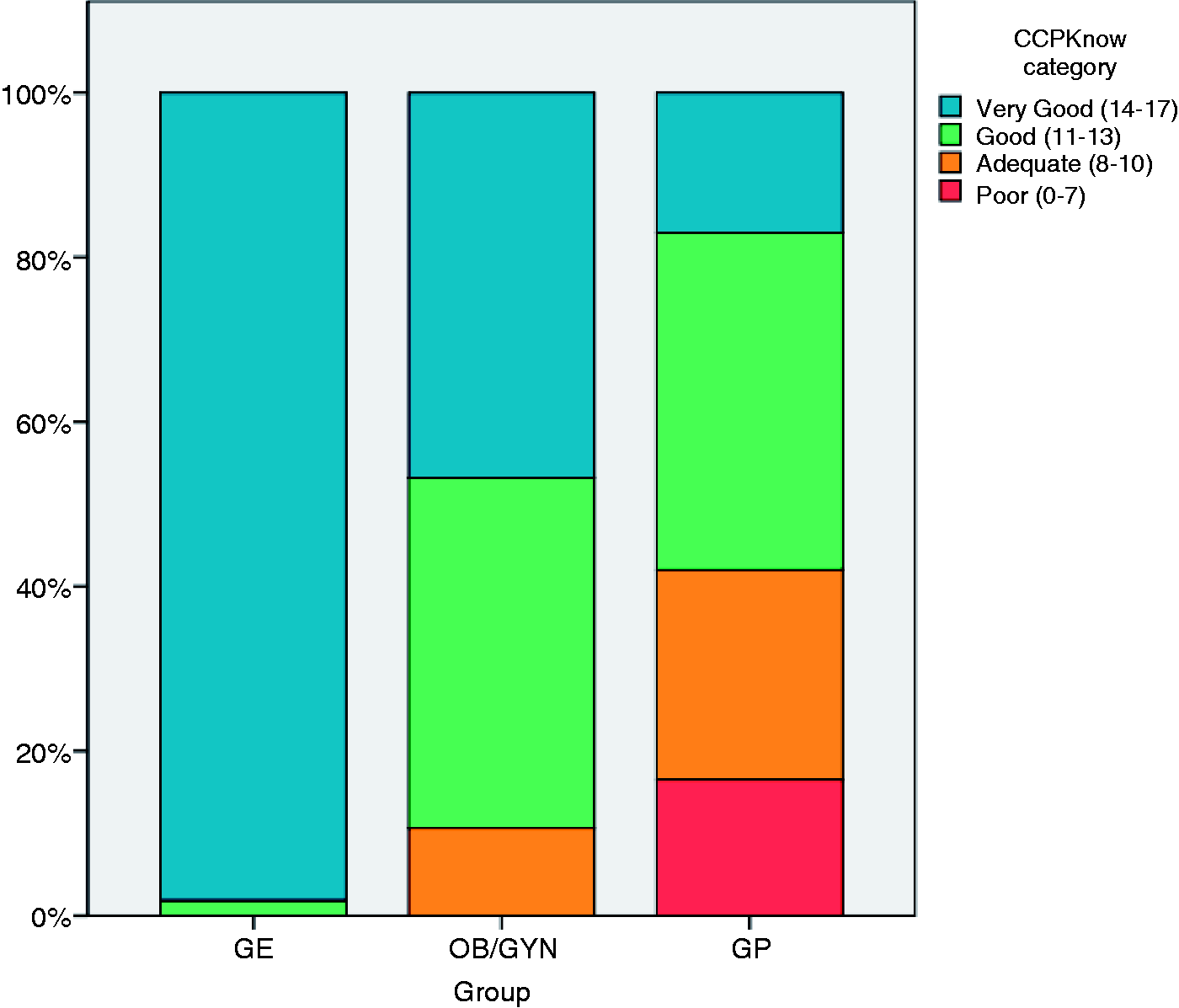
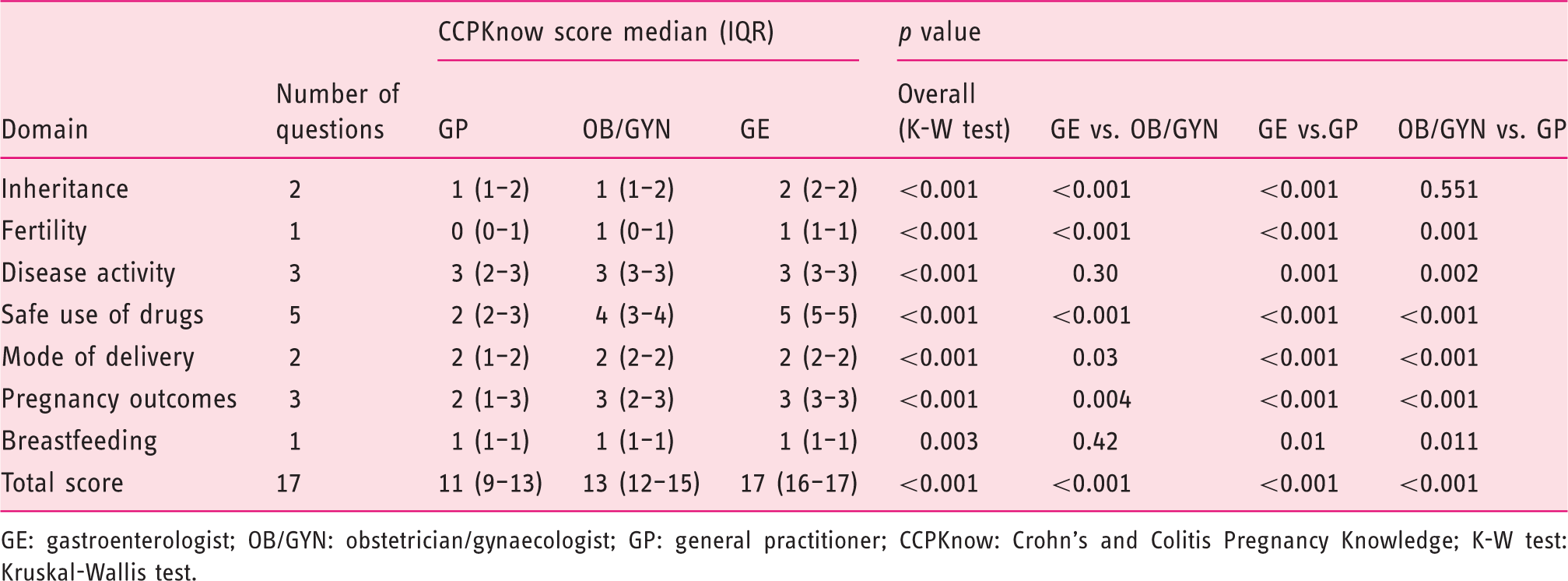
The median total CCPKnow scores for GPs, OB/GYNs and GEs were 11.0 (interquartile range (IQR) = 9–13), 13.0 (IQR = 12–15) and 17.0 (IQR = 16–17), respectively, p < 0.001. The overwhelming majority of GEs (98.1%) had a ‘very good knowledge’ level of IBD-specific pregnancy-related issues (CCPKnow score 14–17) compared to 17.0% of GPs and 46.8% of OB/GYNs (p < 0.001). The distribution and summary of CCPKnow scores in detail for participants are presented in Figures 1 and 2, respectively. GEs’ knowledge in domains of inheritance, fertility, safe use of drugs, and pregnancy outcomes was significantly higher than that of OB/GYNs; whilst for disease activity, mode of delivery and breastfeeding domains scores did not differ significantly (Table 4). GEs’ knowledge was significantly higher in all domains compared to GPs’ (Table 4).
Distribution of CCPKnow scores among health care professionals: GEs, OB/GYNs and GEs. CCPKnow scores and knowledge levels among GEs, OB/GYNs and GPs. CCPKnow individual domain scores among GPs, OB/GYNs and GEs GE: gastroenterologist; OB/GYN: obstetrician/gynaecologist; GP: general practitioner; CCPKnow: Crohn’s and Colitis Pregnancy Knowledge; K-W test: Kruskal-Wallis test.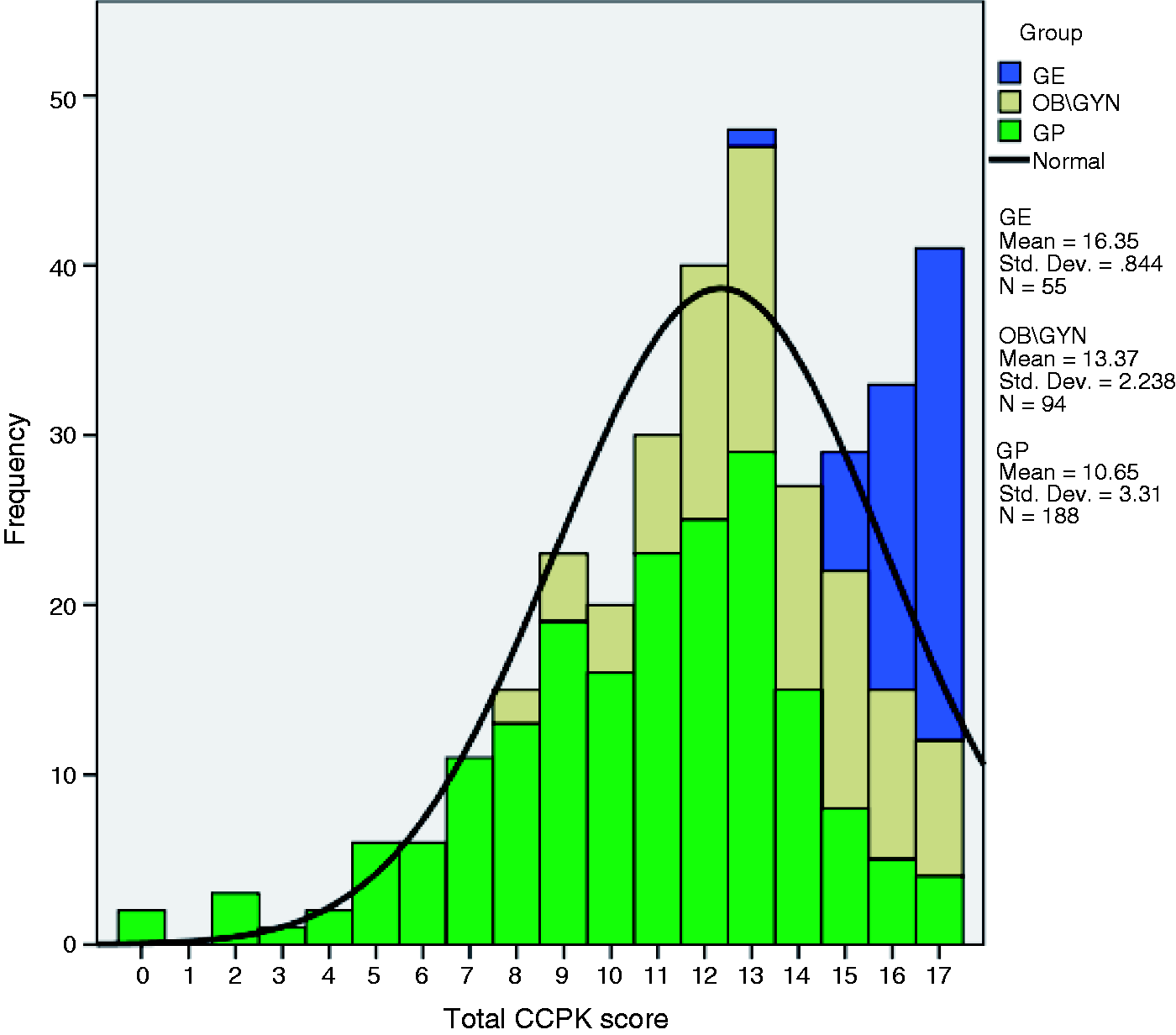
The CCPKnow scores were dichotomised to create categorical variables with score 0–7 being coded as 0 (not very good knowledge) and scores 14–17 being coded as 1 (very good knowledge). Binary logistic regression was performed to explore factors associated with very good knowledge. GEs had the highest chance of having ‘very good knowledge’ compared with GPs (OR: 390, 95% CI: 50.7–3005, p < 0.001) and OB/GYNs (OR: 75.7, 95% CI: 10.0–575, p < 0.001). We can observe high OR values and wide CIs, suggesting that small sample can be a limitation of this study.
Predictors of CCPKnow
GPs had higher CCPKnow scores when they reported seeing more than 10 pregnant patients per month over the last five years (median 13 versus 10, p < 0.001). GPs with additional training in obstetrics (43.6%) also had significantly higher CCPKnow scores than those without additional training (median 12 versus 10, p < 0.001).
Younger OB/GYNs had higher CCPKnow scores than their older counterparts with negative correlations between both age of the specialist and years in practice; and IBD-specific pregnancy-related knowledge (p = 0.01 and 0.003, respectively; Table 2). OB/GYNs whose main focus of practice was obstetric had significantly better knowledge than those with a more substantial gynaecology practice (p = 0.006; Table 2). Heavier case load of >20 pregnant IBD patients in the last five years significantly increased CCPKnow (median 15 versus 13, respectively, p = 0.03; Table 2). Additional variables examined did not correlate with CCPKnow score for either GPs or OB/GYNs.
Among GEs no demographic factor including an interest in IBD were significant predictors of CCPKnow and this is likely to be a ‘ceiling’ effect as almost all of GEs scored in the top category.
Medication use
In contrast to current guidelines,14–16 43.6% of GPs believed administering thiopurine during pregnancy might cause serious harm to the baby or was ‘considered unsafe’, while only 17% thought that the therapy could continue. Only 11% answered that infliximab and adalimumab were regarded as ‘probably safe’ to use during pregnancy. Among OB/GYNs, despite the encouraging global scores, nearly half (46%) thought that the use of azathioprine (AZA) or 6-mercaptopurine (MP) during pregnancy would cause serious harm to the baby or was ‘considered unsafe’. Only 32% thought that AZA/MP could continue, and only 32% thought that infliximab and adalimumab were regarded as ‘probably safe’ to use during pregnancy.
Comfort level with IBD management
Most GPs (79.3%) indicated that they would manage patients either alone or in consultation with other services and their knowledge was higher, but still unacceptably low, in comparison with those who would refer patients on to other colleagues or tertiary services (median CCPKnow 11.0 versus 9.0, respectively, p < 0.001; Supplementary Table 5). Despite the expressed confidence with IBD-specific pregnancy-related issues overall, the majority of GPs (78.7%) felt either very uncomfortable or uncomfortable in starting IBD-related medication prior to or during pregnancy. Almost all GPs would consult IBD specialists and obstetricians in managing IBD patients or their medication use before conception. However, most GPs felt either unsupported or unsure as to how to contact a tertiary IBD service (Supplementary Table 5).
The majority of OB/GYNs (86.2%) indicated that they would manage these patients either alone or in consultation with IBD specialists (96.8%), while the rest would refer to other tertiary services or colleagues (Supplementary Table 5). Despite this expressed general confidence, over 70% of OBs reported feeling either very uncomfortable or uncomfortable to start IBD-related medications prior to or during pregnancy (Supplementary Table 5), showing a disconnect between their knowledge and confidence.
Discussion
This is the first study that objectively assessed IBD-specific pregnancy knowledge of all HCPs likely to be consulted by patients with IBD considering pregnancy. By including GPs, OB/GYNs and GEs, the full spectrum of the pregnancy journey is presented. It is clearly shown that only GEs have a reliably high level of knowledge, making it uncertain what information IBD patients will get depending on which OB/GYN or GP they encounter. GEs had significantly higher knowledge of IBD-specific pregnancy-related issues compared to OB/GYNs and GPs, as they were the only group with a ‘very good’ median score. GEs should therefore proactively engage all their IBD patients of childbearing potential in discussions of pregnancy issues, especially if patients do not express a desire for starting a family. A multidisciplinary team approach is advised to ensure consistency of information and to facilitate holistic care incorporating all elements of general practice and obstetrics. It is important that GPs and OB/GYNs notify and refer IBD patients to GEs as soon as they are found pregnant, and also during their pregnancy if they have any concerns about their disease. GEs must be mindful of the sources of information available to patients with IBD and ensure they are receiving accurate advice. Specifically, GEs have a key role in communicating to GPs and OB/GYNs evidence-based treatment plans and advice.
Both GPs and OB/GYNs had significantly lower overall IBD-specific pregnancy-related knowledge than GEs, with GPs having the lowest overall knowledge. This most likely reflects levels of training and experience. The knowledge was higher where OB/GYNs saw at least 20 pregnant IBD patients in the last five years, supporting the need for subspecialised high-risk obstetric clinics or individuals with subspecialisation or special interest. GPs and OB/GYNs often view IBD as an uncommon condition and feel that they cannot be expected to know the pregnancy issues surrounding the disease due to their limited exposure. 17 The results also demonstrate a striking disconnect between expressed comfort in managing IBD-specific pregnancy-related issues generally and assurance in the appropriate use of IBD medications (both initiation and maintenance) among GPs and OB/GYNs. Over 70% of GPs and OB/GYNs reported being uncomfortable or very uncomfortable in initiating IBD medications and nearly half of each group were misinformed with regard to the safety of ongoing use of thiopurines during conception and pregnancy.
Both GPs and OB/GYNs demonstrated poor understanding of the safety and use of thiopurines, infliximab and adalimumab, which may lead to inappropriate patient management, unnecessary and dangerous cessation of maintenance medications and/or failure to initiate medications when needed. Not only may this heighten patient anxiety and fears around pregnancy and reproduction, it may also jeopardise IBD disease control and pregnancy outcomes.15,17,18 Of concern, this lack of knowledge and comfort with regard to therapy is despite OB/GYNs and GPs apparently having understanding of the importance of disease control prior to, and during pregnancy, for both mother and baby.
The suboptimal IBD-specific pregnancy-related knowledge of GPs and OB/GYNs has the potential for the provision of harmful misinformation to patients with IBD. HCPs’ lack of knowledge was particularly marked in the areas of fertility, inheritance, safe use of drugs and pregnancy outcomes. Poor knowledge in these important areas is of concern as many patients themselves have poor knowledge. 10 Many patients with IBD already have significant IBD-specific pregnancy-related concerns,2,3 with 36% of patients believing IBD medications are harmful to unborn children. 11 Such views may increase levels of voluntary childlessness. Medical misinformation may not only contribute to poor IBD-specific pregnancy-related knowledge in patients but also create and enhance fear and anxiety in this group. Early and accurate advice from a GE can be recommended.
There appears to be an underuse of IBD specialist services with more than 70% of GPs feeling unsupported or unsure of how to contact IBD services. This may reflect the relative scarcity of IBD services, unawareness of services, referral pathways or an underestimation of the complexity of cases. IBD specialist nurses, whose knowledge was previously examined (median total CCPKnow of 16), 10 offer a high-quality, readily-accessible source of information for IBD patients that is also currently underutilised. Referral pathways should be made readily available and IBD services should regularly inform local GPs of their services.
This study had some limitations. Selection bias, inherent in survey studies, cannot be excluded. However, OB/GYNs and GPs interested in pregnancy-related issues in IBD may have been more likely to respond, thereby leading to over- rather than underestimation of knowledge. While the number of responders was less than hoped for, the statistical analysis has shown robust results. The low postal return (<10%) rate among GPs may reflect the relative rarity of them encountering pregnant IBD patients. The knowledge of GPs about IBD in general, 12 has been previously shown to be less than ideal, which is consistent with the results obtained in our study. This study was performed in the unique Australian care system that may not be true universally. However, other information from elsewhere suggests that anxiety and unwarranted fear in IBD patients resulting in voluntary childlessness and smaller family sizes are big issues universally.6,7,19
While CCPKnow was developed to assess IBD patients’ knowledge, it was validated by lay people and health care professionals including junior doctors and IBD specialist nurses. As such the use in professionals is within the scope of CCPKnow. Furthermore in our opinion CCPKnow tests for knowledge required to provide basic IBD care for pregnant patients rather than distinguishing IBD experts from non-expert GEs. CCPKnow is therefore the best suited tool to assess IBD-specific pregnancy knowledge in non-GEs.
In conclusion, this large study revealed significant gaps in IBD-specific pregnancy-related knowledge of GPs and OB/GYNs. The most concerning of these is the disconnect between their comfort and knowledge especially regarding the use of thiopurines and biological agents that are the mainstay of management for a substantial proportion of IBD patients.
GEs should take on pre-pregnancy counselling and lead proactive care for pregnant IBD patients rather than relying on reactive care approaches, which often put GPs and OB/GYNs under pressure to make treatment decisions for which some of them may be ill equipped.
Footnotes
Funding
Rupert W Leong is funded by a NHMRC Career Development Fellowship.
Conflicts of interest
Jane M Andrews has consulted for, been on advisory boards for and received speaker fees from AbbVie, Abbott, Janssen, AstraZeneca, Nycomed, Takeda, Vital Foods, Shire, Ferring, Fresenius Kabi, and Orphan. Christian P Selinger has received research grants from Shire, Nycomed, Ferring and Warner Chilcott. Matthew Roberts and Soleiman Kashkooli have nothing to declare. Rupert W Leong has served on advisory boards for Aspen, Ferring, AbbVie, Janssen and Takeda.
Acknowledgements
Study concept and supervision: Jane M Andrews
Study design: Matthew Roberts, Christian P Selinger, Rupert W Leong, Jane M Andrews
Data collection, data interpretation and manuscript preparation: Matthew Roberts, Soleiman B Kashkooli
Data statistical analysis and manuscript initial drafting: Soleiman B Kashkool
Manuscript critical revision, data interpretation: Rupert W Leong, Christian P Selinger, Jane M Andrews
Final version approval: Jane M Andrews, Rupert W Leong, Matthew Roberts, Soleiman B Kashkooli, Christian P Selinger
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.